Introduction
Dancers are a population that needs to combine the qualities and skills of both athletes and artists. To reach a pre-professional or professional level, many years of intensive training are required.1 The demanding training volume, paired with the repetition of powerful movements at the limit of a dancer’s range of motion, could explain the high injury incidence reported in the literature.1–4 Injuries and pain pose a threat to dancers’ physical and mental health, as well as their career.5 The musculoskeletal pain and injuries sustained by dancers affect mainly the lower limbs (66-91%) and the lumbar region (8-16%).1,3,4 Most injuries in dancers occur in the ankle, the leg and the foot.1,3,4 The structures injured are predominantly ligaments, muscles, tendons and fascia.1,3,4 These injuries will occur due to overuse in 66-79% of cases.1,3,4,6 There is therefore potential for prevention through preseason musculoskeletal screening and functional performance testing.1,7 Due to the significant impact and high number of injuries among dancers, screening could be a valuable way of preventing an important portion of injuries.
Few risk factors for musculoskeletal pain and injuries have been identified for dancers in the literature.8 A recent systematic review of lower limb strength and injuries among dancers highlighted that strength at the hip and knee could have a protective role, but the heterogeneity of the study designs and low quality scores of the studies included prevented the authors from drawing any valid conclusions. They therefore emphasized that more studies were necessary to identify risk factors for musculoskeletal injuries and to guide the development of preventive strategies.9 Activation of the deep abdominal musculature is another potential predicting factor of injury that has raised interest among dance researchers.10,11 Roussel et al. found that dancers who had sustained an injury to the lower back had more difficulties recruiting their transversus abdominis (TrA) compared to dancers without low back pain.11 Thus, the assessment of both hip strength and activation of deep abdominals could be relevant in the prevention of dance injuries. However, focusing on isolated segmental muscle assessment might not be sufficient since dancing requires the body to work in an integrated manner.
Recent authors have highlighted the importance of implementing functional performance tests during preseason preparation.12–14 Studies by Cook et al. as well as Bonazza et al. have determined that the Functional Movement Screen (FMS™) has predictive value for injuries in athletes.15–17 There is an abundance of literature on the FMS™, but its predictive value has been questioned.15–19 The Movement Competency Screen (MCS) has also been investigated in a study on ballet and modern dancers that yielded predictive results.20 Indeed, Lee et al.20 conducted a prospective study which established a cut-off score of 23 under which dancers were more likely to become injured. It is particularly useful for dancers since it uses movement repetitions and plyometric components which would replicate more adequately the conditions of the sport compared to the constructs that are screened in the FMS™. Even if the MCS is able to evaluate the ability to achieve fundamental movements without compensation in dancers, additional research is needed to establish it’s validity.
Both the FMS™ and MCS consist of observing movement patterns while considering the mobility and stability continuum to assess whether the athlete is able to complete fundamental movements without pain and compensation. These movements are hypothesized to require the activation of the deep abdominals and strength of the hip muscles. In fact, Hodges et al. suggest that the transversus abdominis (TrA), which is a deep abdominal muscle and an important lumbar stabilizer, should activate prior to the movement of limbs in order to allow performance of a functional task without any compensation, as those required in the MCS.21 The importance of the hip muscles in stabilizing the pelvis and lower extremity during functional movement performance is demonstrated by evidence that weakness of these muscles affect the incidence of lower limb and back injuries.22 Asymmetry in hip muscle strength is common among athletes: right handed athletes often exhibit greater strength in the left hip extensor muscles and right hip abductor muscles.23 These asymmetries impose a greater demand on the weaker hip muscle groups during the execution of fundamental movements that can lead to compensation and/or misalignement observed at the trunk, pelvis or lower limb.24 In other words, trunk stability cannot be achieved without pelvis stability. Although the trunk muscles including the TrA play an important role in lumbar stability during execution of fundamental movements, activation of these muscles alone does not prevent compensatory trunk motions correlated with weak hip muscles. The relationship between the MCS and basic abilities that are necessary to perform movements without compensation, such as the activation of deep abdominals and hip muscle strength, has not been investigated.25 The current study is therefore an early step in improving the quality of literature concerning the MCS.
This study aimed to investigate the validity of the MCS for use in dancers by 1) examining the correlation between the score of this movement screen and the activation of deep abdominals and hip strength (convergent validity) and 2) investigating the correlation between its scores and those of the FMS™ which also evaluates the capacity to perform fundamental movements (criterion validity).
Methods
Study design
This cross-sectional study is the first step in a larger longitudinal project. The data for the current study were collected during an evaluation session scheduled at the beginning of the dance season in multiple dance schools and companies in two large metropolitan areas. This project was approved by the institutional review boards of the Centre de recherche du CIUSSS de l’Estrie-CHUS and Cégep de St-Laurent. All participants gave written informed consent prior to participation.
Participants
Included participants were ballet or contemporary dancers, aged 16 years or older, enrolled in a pre-professional program or employed by a dance company or a dance program, and able to read and speak fluently in French or English. They also had to dance for more than 10 hours per week. This threshold was selected to ensure that all dancers achieved a similar baseline for dance exposure. Dancers were excluded if they presented with an injury preventing them from dancing at the time of the evaluation. Women were excluded if they were pregnant, since pregnancy impacts the lumbopelvic muscles.
The sample size was calculated in relation to the first objective assessing convergent validity. A total of 19 participants were needed considering an expected correlation coefficient of 0.7 (which characterizes an acceptable correlation26), a power of 80% and an alpha of 0.05. Since this study was part of a larger research project requiring 118 participants, sufficient power for the analyses conducted was obtained. The guide established by Akoglu was used to qualify correlations (<0.4=weak, 0.4-<0.7=moderate, 0.7-0.9=strong, >0.9=very strong correlation).27
Recruitment
Pre-professional schools and professional companies were first approached by a physiotherapist member of the research team to explain the objectives of the study and to seek approval to recruit among their students or employees. Once the organizations agreed, a presentation was then scheduled at each institution to inform professional and pre-professional dancers about the objectives of the project as well as the inclusion and exclusion criteria. Participation in the research study was voluntary. Dancers interested in participating could either schedule the initial evaluation at the end of the presentation or leave their contact information so that the physiotherapist performing the evaluations could contact them. Participants were screened for inclusion and exclusion criteria at the beginning of the first evaluation.
Data collection
Each evaluation was conducted individually in a closed room by a physiotherapist who had two years of experience with the evaluation and treatment of dancers. The evaluations took place at the school or company to minimize inconvenience for dancers. They were scheduled in the span of six weeks at the beginning of a season, and lasted between 60 and 90 minutes. Dancers first gave informed consent, filled out a demographic questionnaire including questions about their dance background, and then completed the physical evaluation.
Convergent validity: transversus abdominis activation and hip strength
In order to evaluate the convergent validity, the activation of the TrA as well as strength in hip muscles were measured on both the dominant and non dominant side. The TrA is one of the core trunk muscles responsible for maintaining trunk stability by preventing the loss of balance during limb movement, which is necessary to perform the tasks in the MCS.28–30 Theoretically, the position and function of the hip muscles contribute to the alignment of the pelvis and lower limb, which is of paramount importance in the performance of the movements in the MCS.
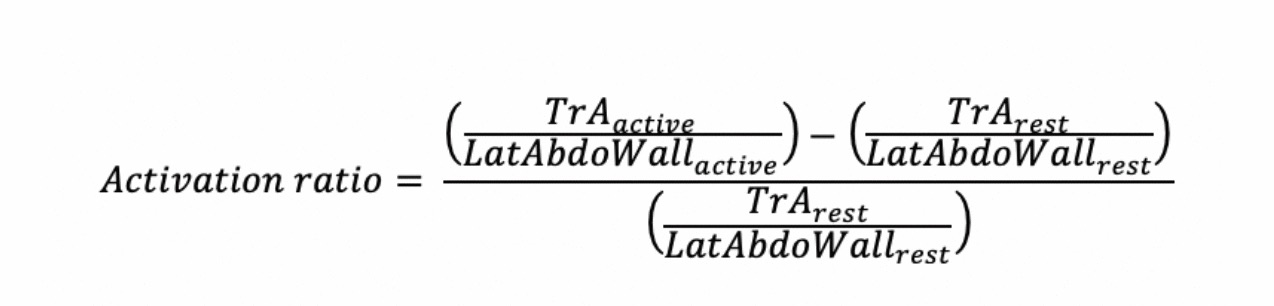
The transversus abdominis activation was evaluated using an ultrasound device (GE LOGIQ E, GE Healthcare, Milwaukee, Wisconsin, 13 MHz linear probe in B-mode). The probe was in a transverse plane and positioned at the mid-distance between the 12th rib and the iliac crest. The physiotherapist started at the linea alba and moved the probe laterally past the rectus abdominis and in between the mamillar and axillary lines until all three abdominal muscle layers, the external and internal oblique and the transversus abdominis, could clearly be seen. A single researcher took all the measurments. The angle of the probe was adjusted to optimize image quality. This non-invasive technology allows the visualization of the changes in thickness of the muscles compressing the abdominal wall when they activate. All participants were assessed in a standardized supine position with knees bent at 90° and were given standardized hollow-in instructions.31 Images were taken at the end of the expiration for both rest and activation measures. For clinicians with minimal experience in ultrasound imaging of the TrA, it was previously found that the intra-rater reliability ranged from 0.87 to 0.99 and the inter-rater reliability ranged from 0.80 to 0.92.32 This method was validated to assess the transversus abdominis activation by calculating an activation ratio as seen in Figure 1.31

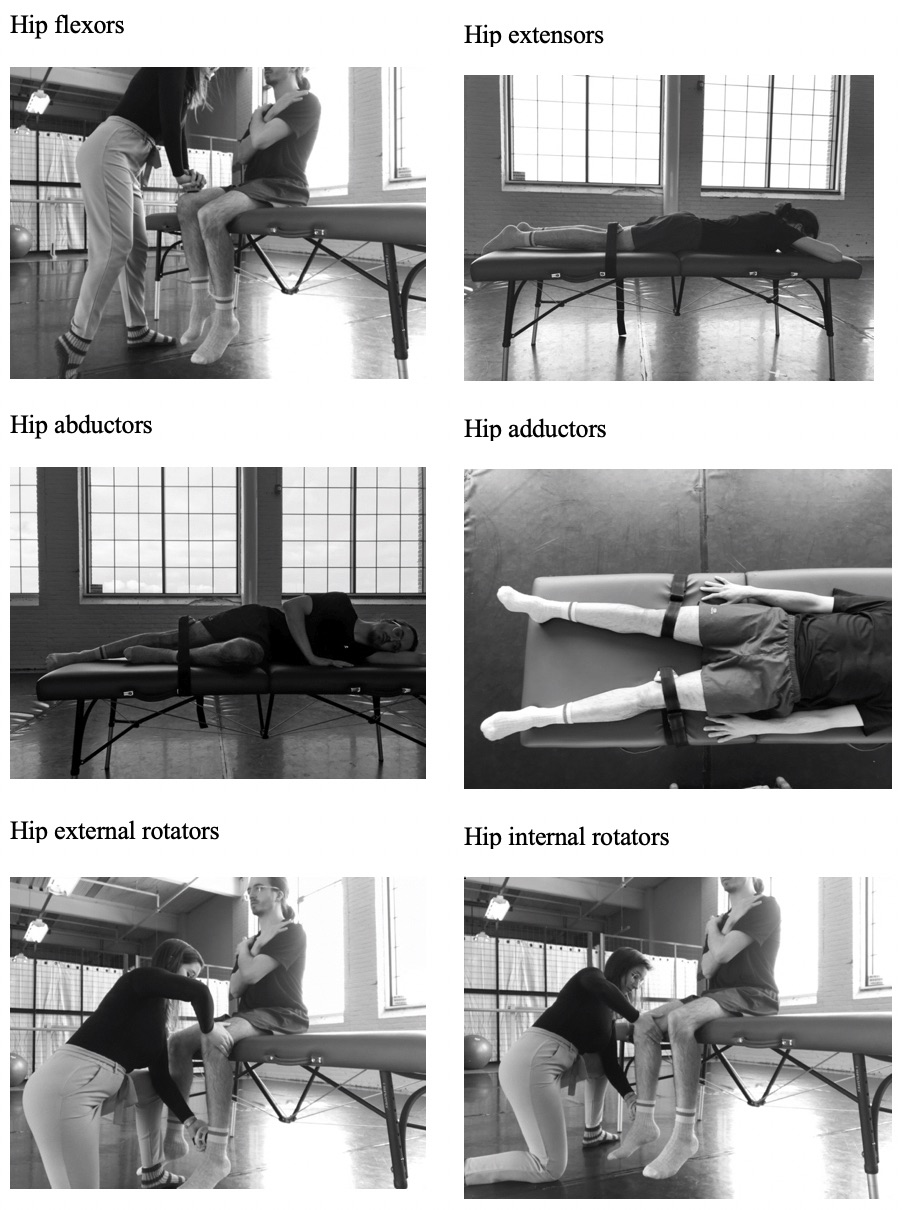
Strength was evaluated for all six muscle groups of the hip, in this order: abductors, adductors, extensors, flexors, external rotators and internal rotators. Each muscle group was tested three times with a 30-second pause between measurements. The average of the three measures was used to calculate correlations. A handheld dynamometer (MicroFET, Hoggan Scientific LLC, Salt Lake City, Utah), and straps were used to provide a fixed resistance for the participant as they exerted a maximal voluntary contraction. The intra and inter-rater reliability of the MicroFET has previously been shown to be excellent for hip muscles.33 Every muscle group was evaluated in a standardized position as seen in Figure 2. The positions used were those validated by Krause et al.33


Functional tests
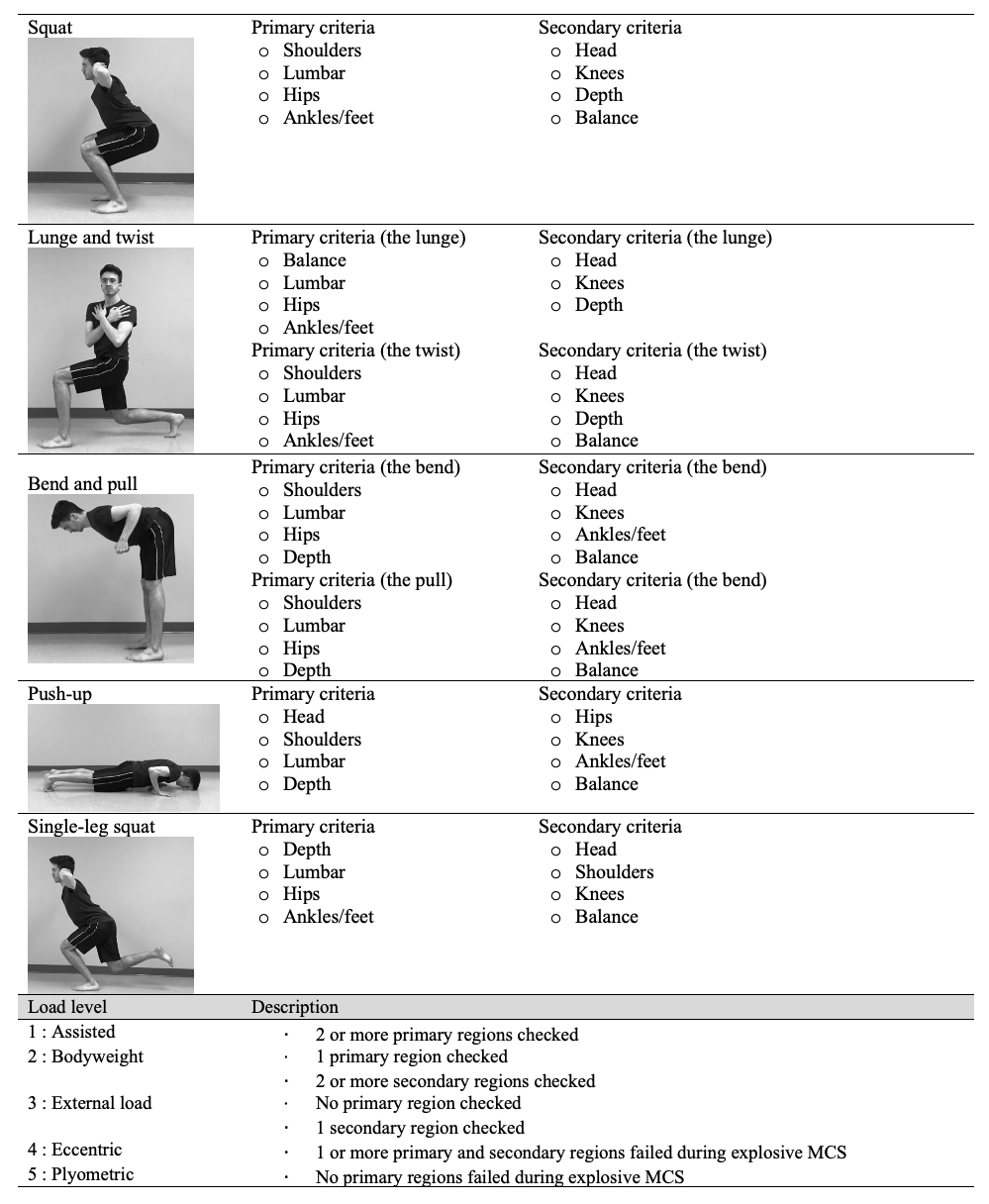
To assess the criterion validity of the MCS, it was investigated whether the dancers’ scores on this test were related to their score on the FMS™. These two functional tests assess the ability to perform fundamental movements without pain and/or compensation. The MCS is composed of five fundamental movements : body weight squat, lunge and twist, push-up, bend and pull, and single-leg squat.25 Each movement has its own load level, which can range from assisted (1) to plyometric (5) (Table 1). Each task is rated using a list of primary and secondary body regions to assess for compensations. The primary compensation checkpoints are the most important for a given movement. Compensations for every checkpoint are detailed in the thesis of Kritz25 and the study of Lee et al.20 A lower score indicates poor movement competency and a higher score indicates high movement competency. Movements were evaluated in both the sagittal and frontal planes. This test was validated for the evaluation of movement-related risk factors and has excellent intra (Kappa = 0.93) and inter-rater reliability (79%).25 The final score is calculated by taking the sum of the lowest score out of the two sides for each item.25
The FMS™, which has been extensively studied in athletes,17–19 uses seven fundamental movements: squat, hurdle-step, in-line lunge, shoulder mobility, active straight-leg raise, push-up and rotary stability.15–18 Each task is rated on an ordinal scale from 0 to 3, with the highest score indicating that the athlete can achieve the movement without any compensation. All tasks were evaluated in the sagittal and frontal planes. It has an excellent intra (ICC=0.81) and inter-rater reliability (ICC=0.81).17 Despite the identification of a cut-off score for a certain number of studies,17,34,35 not all researchers have been able to support the use of the FMS™ as a predictive tool.18,36
Statistical analysis
Descriptive analysis was used to characterize the sample for baseline characteristics, deep abdominal activation, hip strength and functional test scores. Since our population was heterogenous, we also conducted t-tests to compare the MCS total score between contemporary and ballet dancers as well as professional and pre-professional dancers. Bivariate correlations and hierarchical regressions were used to explore the correlation between the MCS and FMS™ as well as the correlation between the MCS and the activation of TrA and hip strength (objectives 1 and 2).26 The model used in hierarchical regressions was based on what was obtained in bivariate correlations. If the correlation between the variable and the MCS score was significant (i.e. p≤0.05), the variable was included in the regression.
Results
Participants
A total of 77 participants were recruited from three companies and six pre-professional schools. There were 41 contemporary dancers and 36 ballet dancers. Dancers were aged 21.23 ± 4.86 years old and had been dancing for an average of 13.40 ± 5.75 years. The sample was composed of 66 women and 11 men. The majority of participants were pre-professional dancers (n=61) compared to professionals (n=16). The participants’ characteristics are presented in Table 2.
Functional test scores
Table 3 depicts the mean total scores (± standard deviation) for the FMS™ and MCS as well as the scores for each item of the tests for the whole sample. Further analyses revealed no differences in the functional test scores between ballet and contemporary dancers, as well as professional and preprofessional dancers.
Relationship between the FMS™ and MCS
The scoring of the two functionnal tests were moderately correlated (r=0.489, p<0.001).27 Since three items from both tests were similar, additional correlations were established for them. The squat items were not correlated (r=0.085, p=0.460). The correlation was weak for the lunge items (r=0.234, p=0.040) and moderate for the push-up items (r=0.587, p<0.001).27
Relationship between functional tests, transversus abdominis activation and hip strength
The total score on the MCS was weakly correlated with activation of the TrA. The correlation of TrA activation with the MCS total score was r=0.239, p=0.036. Individual items from the MCS were not correlated with the activation of the TrA.
The MCS total score was also weakly and positively correlated with the strength of hip abductors (r=0.293, p=0.010), adductors (r=0.267, p=0.019) and external rotators (r=0.249, p=0.029). The other muscle groups, which included hip flexors, extensors and internal rotators, were not significantly linked to MCS total score.
Explaining the variance of the MCS
Hierarchical regressions, presented in Table 4, showed that the activation of the transversus abdominis and the strength of hip abductors, adductors and external rotators explained 14.1% of the variance of the MCS total score (F4,76=8.623, p=0.005). Both the activation of the transversus abdominis and the strength of hip abductors were correlated with the MCS total score (p<0.028). The activation of the transversus abdominis explained 3.3% of the MCS total score while the hip strength explained 10.8%.
Discussion
This study aimed to develop new knowledge about the validity of the MCS for dancers. It was established that there were weak correlations between the MCS and the activation of deep abdominals and hip strength. It was also found that the MCS and FMS™ scores were moderately correlated.
Relationship between MCS, TrA activation and hip strength
A significant (albeit mild) positive correlation was observed between the MCS total score and the TrA activation. It was found that better TrA activation was correlated with a higher score on the MCS. These findings concur with those found in multiple studies conducted by Hodges et al.28 In healthy, non-injured individuals, trunk muscles including the TrA contribute to the maintenance of trunk stability by making a sequence of postural adjustments before the distal movement to prevent any loss of balance.28 Since the tasks of the functional tests require trunk stability, a significant correlation between TrA and functional movement performance test was anticipated. It should however be emphasized that the correlation was weak, which may be explained by compensatory movements. For example, some participants may have completed the functional movement tests by activating other muscles such as the rectus abdominis, the internal and external obliques, and the multifidus or gluteal muscles. Others may have successfully activated the TrA but could have had difficulty performing some of the tasks because TrA activation taken in isolation is not the only parameter to consider. Indeed, when performing a movement, the ability to activate the TrA in a supine position does not guarantee that the dancer will perfom a movement in a different position adequately. However, it has been reported that the activation of the TrA in the same participant does not vary according to the assessment position.31 Since the participants were evaluated in a supine position for the TrA activation test and in various positions for the functional tests, this could have contributed to a reduced correlation between tests.37 Similarly to the TrA activation, the measurements for all hip muscle strength tests were performed in different positions than those used for the MCS tasks, which could explain lower correlations.
In order to advance our understanding of the MCS total score, a hierarchical regression was conducted based on the results from the bivariate correlations. The model could significantly explain 14.1% of the variance. While the activation of the TrA explained 3.3% of the variance, the combination of hip abductors, adductors and external rotators strength explained 10.8%. Similarly, Mitchell et al. found that abdominal strength could explain 12% of the variance of the FMS™ score.30 However, this study was conducted in children and did not account for lower limb strength. Moreover, core strength was measured with functional movements such as prone and side planks. In the current study, the assessment was extended to examine whether the activation of deep abdominals, the main stabilizers of the lumbar region, and hip strength, also stabilizers to the lumbopelvic region, could indeed affect the MCS score.
Relationship between functional tests
This is the first study to examine the correlation between the MCS and FMS™, and a moderate correlation (r=0.489, p<0.001) was found between the two tests.27 The current study demonstrates that there is convergence between the two tests, particularly for the push-up and lunge items. The lower level of correlation could be explained by the fact that only three items were similar: the squat, lunge and push-up. The current study also shed light on the relationships between these similar items. No correlation was found between the squat items, indicating that they likely measure somewhat different constructs. The lunge items were poorly correlated and the push-up items were moderately correlated. The low correlations between the squat and lunge items could be explained by the fact that both were evaluated rather differently from one test to the other. The squat item in the FMS™ requires that a dowel held over the head remains in line with the ankles, which was not required in the MCS item. In the same way, the lunge item in the MCS required a twist of the trunk at the end of the movement that is not a part of the FMS™ task.
Study limitations
A few limitations should be acknowledged. It should be noted that the evaluation, including the tasks from the functional tests, always followed the same order. Therefore, FMS™ and MCS scores could have been influenced by this. Fatigue could have induced a systematic error. There was also a diversity in the dancers who were recruited. However, since no differences were found between ballet and contemporary as well as between professional and pre-professional dancers for the MCS total score, the impact would seem to be minimal on the conclusions drawn for individual groups. Most studies have concentrated solely on pre-professional or professional dancers, often on a single dance style and in one institution. However, the diversification of level, dance style and institution helps strengthen the external validity of the results presented in this study. Future research should focus on longitudinal studies that address whether or not the MCS could be used as a predictive tool of injuries among dancers.
Conclusion
This pioneering study is the first to evaluate the convergent validity of the MCS by examining the correlation between the MCS and the activation of deep abdominals and hip strength for dancers. Significant correlations were found between the MCS total score, the activation of the TrA and the strength of hip abductors, adductors and external rotators. Although the correlations varied from weak to moderate, this supports a relationship between the functional movements score, TrA activation and hip strength. The MCS was also found to be significantly correlated with the FMS™, which supports the criterion validity of the MCS in dancers. These results are of great interest given the high proportion of injuries and pain among dancers and the need for screening and prevention. By corroborating the convergent and criterion validity of the MCS in dancers, this study is a step towards its use in preventing injuries in dancers.
Conflict of interest
All authors confirm that no prior or duplicate publication has been released elsewhere concerning this manuscript and that no commercial relationships which may lead to conflict of interest were associated with this work.
Funding
Funding from the Institut de recherche Robert-Sauvé en santé et en sécurité du travail was obtained (03SNT007).