

INTRODUCTION
Non-contact injury to the anterior cruciate ligament (ACL) in female athletes has been investigated quite extensively. Despite the plethora of investigations, females are two to eight times more likely to suffer this traumatic injury as compared to males.1 Although the proposed etiology of non-contact ACL ruptures appears multifactorial, improper landing mechanics in female athletes has been cited as associated with increased injury risk.2–4 Furthermore, a second ACL rupture is more likely in athletes within two years after ligament reconstruction following return to sport that involve jumping and landing activities where aberrant landing patterns were shown.5–7
The best strategy for identifying these aberrant landing patterns and the most effective intervention for their remediation is debatable. Augmented feedback using external sources (ie. use of video display and verbal cueing and instruction based on expertise from an instructor) is most often employed in the clinical setting due to their relative ease of implementation. Traditionally, clinicians attempt to modify athletes’ landing mechanics by providing instructions to promote more optimal body postures and joint alignment; however, these types of instructions often only produce transient changes in landing mechanics.8 As a result, there appears to be a need for more advanced methods of athlete feedback. Post-performance video feedback has been shown to promote changes in landing patterns that may reduce ACL injury in female athletes (e.g. lower vertical ground reaction forces, less knee abduction).3,4,9–16 This is encouraging, as video can be recorded in clinical or field settings using widely available, low-cost equipment such as smartphones, tablets, etc. However, the information obtained from such videos is subjective and does not provide insight into the forces experienced during landing. In addition, most standard video cameras sample data at rates that are too low for dynamic movements such as drop landings.
Assessments that incorporate three-dimensional (3-D) analysis of drop landings have also been used to identify kinematic and kinetic measures that may be related to a higher risk of non-contact ACL injuries in female athletes.3,8,15,17,18 Post-trial feedback has been shown to be effective in modifying neuromuscular risk factors in drop landing and can provide more accurate and objective kinematic and kinetic information which may serve to better identify risk factors for injury or re-injury.15 However, many of these investigations have used expensive and elaborate laboratory-based methods to provide such feedback4,19–21 that would be impractical to implement large scale especially in field settings. Therefore, this type of performance-based feedback may not have the ability to reach the target population (ie. adolescent female high school athletes).
There appears to be a need to develop landing assessment and training tools that can provide immediate post-trial feedback relevant to an athlete’s performance that is both objective and qualitative. The purpose of this study was to investigate the effectiveness of a single training session using a custom portable feedback training system that provides performance cues to promote changes in impact kinetics and lower extremity position during landing in female athletes. Feedback provided during training was based on kinetic/kinematic data recorded via the system and individualized cues from an investigator.
METHODS
Subjects
This study was approved by the University of Wisconsin La Crosse’s Institutional Review Board. Prior to participation in this study, all subjects or parent provided their written informed consent in accordance with University guidelines.
One hundred fifty females at regional high schools between the ages of 13-18 years old participated in this single session study. Age, height, body mass index, and Tegner level22 was recorded. All were actively participating female athletes. Exclusion criteria for the study included (1) any current lower extremity injury, (2) knee pain at rest or during running or jumping, (3) pregnancy, (4) any cardiovascular abnormalities or medical condition that limited training as indicated by a physical activity readiness questionnaire (PAR-Q).23 All participants utilized their own athletic footwear and wore comfortable athletic clothing during the study.
Procedures
Participants were asked to complete a drop landing from a 50 centimeter (cm) platform. Prior to testing, athletes were given verbal instructions for the landing task including: 1) jump forward with both feet off the raised platform and land with both feet while having one foot near the center of each force platform, (2) jump bilaterally rather than stepping off the box, (3) land as to not fall forward off of the force platforms, (4) return to standing from landing position and maintain that position for two seconds. During data collection, trials were discounted if those requirements were not met. Participants were allowed up to three practice trials to familiarize themselves with the task. Data were collected generally in a gymnasium or common space with a ceiling height that could accommodate the experimental setup.
Kinetic data were obtained from two custom, high impact force plates designed for these in situ data collections. Each force platform was positioned adjacent to one another and 25 cm in front of the 50 cm platform. Each force platform was custom made with 4 calibrated load cells (ntep-1klb shear beam load cell) capable of measuring vertical force. Bilateral vertical ground reaction force (vGRF) data were sampled at 2000 Hz and normalized to each participant’s body weight. Validation of the system was performed in a pilot investigation of 20 participants where the custom force platforms were placed directly on top of two commercially available force platforms (Model 4080, Bertec Corporation, Columbus, OH) and sampled at 2000 Hz on both systems. The peak vGRF was within 5% of that obtained with the commercially available force platforms. This accuracy criteria are likely considered reasonable regarding force plate accuracy for a portable system during a dynamic impact situation such as landing.24 Frontal plane video of each participant focused on the lower extremities were recorded from a high-speed camera at 100 Hz (DFK 23UV024, The Imaging Source, LLC, Charlotte, NC, USA) during each performance trial. The camera was positioned on a tripod at a height of 65 cm and at a distance of 130 cm from the force plates. Custom scripts were implemented within commercial software (Innovative Sports Training, Inc., Chicago, IL, USA) and used on a digital monitor in front of the performer to provide immediate post-trial feedback. (Figure 1)

Athletes completed 30 landing trials divided into five blocks of six trials with one minute of rest provided between each trial block. During the initial block (Pre-test), participants were blinded to any form of feedback to determine their baseline landing performance. Prior to beginning the training blocks, the athletes were provided with a brief overview of the information they would receive on the visual feedback display post each trial. This information included peak vGRF displayed in body weight, symmetry of lower extremity vGRF demonstrated through a seesaw/teeter totter display, and frontal plane video that was replayed by the investigator to depict a qualitative impression of the performer’s lower extremity alignment and overall body position during landing (Figure 2)
__vgrf_symmetry_and_in_.jpg)
The baseline test was followed by the first training block (Training 1) where participants received post-trial feedback based on these data coupled with cues for improving landing performance from an investigator. Athletes were provided with both externally focused feedback first (e.g. “try to reduce the vGRF value”, “try to land quieter or more softly”) and then internally focused feedback (e.g. “try to keep your knees over your toes,” “try to land with your knees out”). The feedback provided was individualized and dependent upon what was observed based on the peak vGRF, vGRF symmetry and general impression from the video of the athletes’ frontal plane landing kinematics. The general order of the feedback was based on the order of processing of these data on the display (peak vGRF, vGRF symmetry and then video of performance). These data were available within 20 seconds after each landing. The video was available in second window initially behind the force display and was available last due to computer processing requirements associated with recording these images at high speed. Athletes were given time to review the data and then relevant cues were provided by the investigator. The next trial was then immediately performed such that the entire testing and training session took approximately 20 minutes. The general training and feedback used was systematic where once that variable such as vGRF showed substantial improvement, the next variable was selected for feedback. During the second training set (Training 2), the feedback from the investigator was gradually withdrawn and the athletes were asked to self-evaluate their peak vGRF, loading symmetry and body alignment and position projected to the display. Participants were encouraged to incorporate strategies that they felt were most helpful for performance improvement based on their first training block. Following completion of Training 1 and Training 2, a post-test (six trial block) was completed without any verbal or visual feedback. Finally, a transfer task was examined where a dual task landing was performed without feedback. During the dual transfer task, participants were required to attend to catching a ball while landing. Six trials were performed with a tester either throwing the ball or faking a throw. The order of the testing condition (throw or fake throw) was randomized for each participant. Outcome data from the transfer condition performance trials were pooled.
Data Processing
Kinetic data were exported and processed in Excel where peak vGRF in body weight for each trial were determined. Scaled video data were analyzed within Kinovea (https://www.kinovea.org) to determine knee to ankle separation ratio (K:A ratio).25 Kinovea is a software program that allows various video formats to be opened, scaled and points where points on the image can be used to calculate various kinematic measurements. This approach to measuring knee abduction has shown high intra and interrater reliability (0.97 and 0.92 respectively).25 From a force threshold of 10 N, a single video frame was selected 100 ms26 after impact for analysis of frontal plane knee motion. K:A ratio was the distance from the estimated knee joint center to ankle joint center.25,27,28 K:A ratios of less than 1.0 are indicative of more knee valgus positioning during landing.25,27,28
_i.jpg)
_ratio_for_the_pre-te.jpg)
STATISTICAL METHODS
The dependent variables of interest were peak vGRF and K:A ratio. Means for peak total vGRF in multiples of body weight and K:A ratio were calculated for the three blocks of six trials (baseline, post-test, and transfer task). A repeated measures analysis of variance (ANOVA) (alpha set to 0.05) was then performed to examine differences in trial blocks (baseline, post-test, and transfer task) in vGRF and then on K:A ratio. Post hoc comparisons were performed using the Bonferoni approach. Effect sizes (Cohen’s d) were calculated between the same trial blocks. Statistical analysis was completed utilizing SPSS, version 25 (IBM Corporation, Armonk, NY, USA).
RESULTS
Demographic data on participants are provided in Table 1. Means and standard deviations for these participants were: age of 14.94 ± 1.61 years, height of 1.67 ± 0.08 m, weight of 60.95 ± 11.09 kg, and body mass index of 20.86 ± 3.58. Athletes reported a Tegner level22 of at least 5/10 and were currently competing in competitive volleyball and/or basketball programs at the high school or club level since the goal was to test actively participating female athletes.
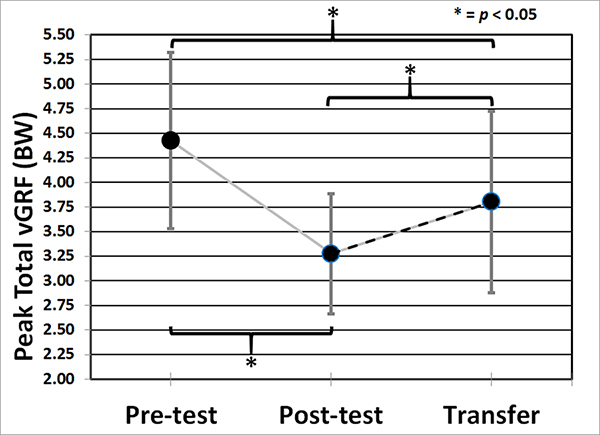
Mean vGRF were different from baseline, post-test and transfer task trial blocks (F(2,298)=181.68, p < .0001).The mean (standard deviation) peak vGRF in multiples of body weight for the pre-test, post-test and transfer task respectively were 4.43 (0.90), 3.28 (0.61), and 3.80 (0.92). Post hoc comparisons showed that baseline vGRF was 29.96% higher than post-test and 14.22% higher during the transfer task but the transfer task was 15.85% greater than the post-test (all p<.0001). The effect size for vGRF from baseline to post-test was 1.52, baseline to transfer was .69 and post-test to transfer was .68.
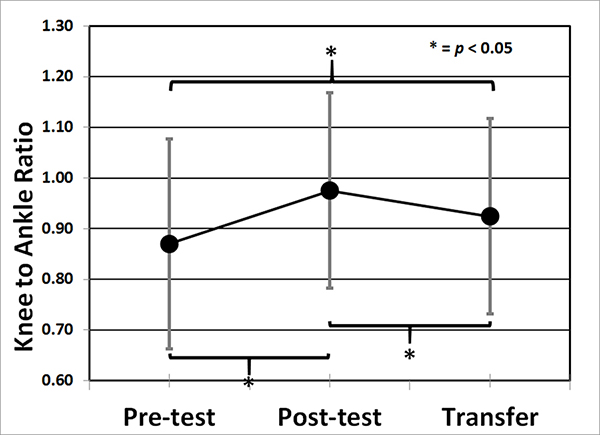
Mean K:A ratio were different from baseline, post-test and transfer task trial blocks (F(2,298)=63.47, p < .0001). The mean (standard deviation) K:A ratio for the baseline, post-test and transfer task respectively were 0.87 (0.21), 0.98 (0.19), and 0.92 (0.19). Post hoc comparisons showed K:A ratio during the baseline was 12.64% greater than post-test and 6.12% greater during the transfer task but the transfer task was 5.75% reduced compared to the post-test (all p<.0001). The effect size for K:A ratio from baseline to post-test was 0.55, baseline to transfer was .25 and post-test to transfer was .32.
DISCUSSION
Findings of the current study indicate that using a portable force plate system interfaced with a digital camera is an effective tool for providing feedback to promote immediate positive changes in vGRF and K:A ratio of adolescent female athletes. The participants in the study demonstrated a reduction in peak vGRF and higher K:A ratio (indicative of less knee abduction) following a training session which included visual feedback related to vGRF, vGRF symmetry and video of frontal plane landing kinematics, as well as cueing for an investigator. Effect sizes were large and moderate for baseline to post-test for vGRF and K:A ratio. Despite these variables regressing toward baseline values, these improvements persisted during the transfer task however both of their effect sizes were between small to medium. Positive transfer of an improved movement pattern to an untrained task, in this case, the dual-task where a ball was randomly passed to the performer is considered an indicator of motor learning.29 Despite previous investigations suggesting that augmented feedback is effective in eliciting improvements in landing mechanics, and this is the first time a portable system has been used that provides salient data that participants appear to respond to that can be used to alter landing mechanics for neuromuscular training on-site with athletic teams.4,10,13–15,28,30–33
The present findings differ in part from Munro and Herrington14 who also evaluated changes in vGRF and knee abduction angle using augmented feedback. In their study, the authors incorporated a combination of strategies including video demonstration of correct landing form, individualized post-trial expert video assessment and a checklist for self-analysis of the performance. Subjects were rated on kinematic variables such as trunk lean, knee valgus and knee flexion during landing. Using video analysis to determine the knee frontal plane projection angle (FPPA), the authors found a 23.9° reduction in knee abduction angle post feedback but no change in vGRF.14 In the current study, a decrease in K:A ratio was also found immediately after training, but these findings differed from Munro and Herrington14 in that the subjects in the present study displayed a nearly 30% decrease in peak vGRF after a single session. However, the present study’s findings do become more tempered as baseline vGRF were only 14.22% higher compared to the transfer task. One reason for these differences may be related to the type of feedback that was utilized for the training session. Both studies used feedback strategies that emphasized key kinematic risk factors with expert feedback for performance improvements; both also utilized self-directed assessments of landing mechanics. However, in the current study, implicit feedback that focused on the performance outcome also incorporated using vGRF and vGRF symmetry. As the participants demonstrated an understanding and mastery of targeted biomechanical variables, verbal cuing by the expert evaluator was withdrawn and the reliance on self-correction using external feedback increased. Studies have suggested that using external cues for skill acquisition may accelerate the learning process by facilitating movement automaticity and enhance the production of effective and efficient movement patterns.33–36 It has also been postulated that a new skill acquired using an external focus of attention is more resilient under psychological and physiological fatigue.33,37–41 Biomechanically, greater knee flexion angles and lower peak ground reaction forces have been reported when landing instructions invoke an external focus of attention.31,42,43 Therefore, in the present study, the utilization of the externally focused performance variables projected on the screen during the landing training may have resulted in reduced vGRFs during landing with feedback withdrawal and during the transfer task.
Previous research has reported that changes in landing mechanics achieved through augmented feedback may be transferrable to a new task. Stroube et al.44 reported that high risk landing mechanics that were identified during a tuck jump with subsequent feedback and training provided over 8 weeks resulted in 37-40% reductions in knee valgus angles during a drop landing. They did not measure ground reaction force nor force symmetry directly but did report changes to “excessive landing noise” and “foot contact timing not equal”. Etnoyer et al.10 showed that participants that received augmented feedback during a box drop-jump task were able to maintain greater peak knee flexion angles during a running stop-jump task compared to controls during a single training session; however, no kinematic differences were reported during a sidestep cutting maneuver. In the current study, reductions in both K:A ratio and vGRF values were found during performance of a transfer task of catching a ball during landing compared to baseline. Compared to baseline, the athletes in the present study demonstrated a 5.75% decrease in K:A ratio during the transfer task. Similarly, the vGRF changes were maintained throughout the transfer task with a 14.22% decrease in force attenuation after training compared to baseline. These findings are important as a transfer task may be more representative of an athletic activity in which the focus of attention is on multiple environmental cues often occurring simultaneously. Instructional sessions that rely solely on internally focused feedback may interfere with an athlete’s ability to apply the newly acquired movement strategies to a less controlled or unstructured task. It has been suggested that incorporating unknown patterns of movement to a training program may enhance the athlete’s motivation during training and stimulate the premotor cortex to find more optimal solutions to unanticipated events during performance.31 Although the results of the transfer task activity show promise, it is speculative to apply these findings to actual athletic competition. Because only a single session of training was provided, the maintenance of any change in performance or how multiple sessions of training can further influence skill learning are currently unknown. Future studies should focus on longer term retention of the biomechanical changes and how landing performance changes during more complex movement patterns that more closely mimics athletic activities.
The feedback training system utilized in this study overcomes many of the barriers associated with conventional laboratory-based equipment, as it is relatively easy to use, inexpensive to develop, and portable. This contributed to the ability to assess/train a large number of athletes in the field. There have been preliminary attempts to explore the potential utility of lower cost gaming systems (e.g. Wii Balance Board or Microsoft Kinect) for movement assessment and feedback training.45,46 These systems overcome the barriers associated with laboratory-based equipment; however, they have technical limitations (e.g. low sampling rates, limited sensor range) that restricts their accuracy for dynamic tasks such as landing. The researchers believe that there is a need to continue to develop/utilize systems such as this which are conducive to testing/training in the field, but also overcome the technical limitations of other systems.
Findings from this investigation appear to indicate that a portable force plate interfaced with a digital camera provide promise to promoting biomechanical changes that may reduce an athlete’s relative risk for ACL injury. Several researchers have reported that greater vertical ground reaction forces at impact and increased knee valgus predispose female athletes to non-contact ACL injuries.3,47–51 Greater impact forces have been associated with anterior tibial accelerations.32 In vitro and modeling studies have reported greater ACL strain and tibial shear with landing patterns that lack adequate knee flexion to absorb impact forces.26,52–55 Increased knee valgus angle during landing has been associated with increased risk for ACL injury in females.3 These kinetic and kinematic findings have led to the development of neuromuscular programs aimed at mitigating these risk factors.4,13,15,32,56 However, most preventative programs do not utilize visual feedback training. The effect of combining of this type of feedback system into a more traditional neuromuscular training program offers promise and appears to warrant further investigation. It is plausible that the use of an augmented feedback system may provide a more effective avenue for neuromuscular training that incorporates the principles of motor learning in skill development.
The present study has limitations. Although the use of a drop landing is widely used in research studies to evaluate kinematics and kinetics that may be related to knee injury, the task may lack external validity. Similarly, the transfer task utilized in this study of a random “catch” or “no catch” may not provide a close enough parallel to the multiple simultaneous environmental cues and motor planning required for sports. Lastly, this study was conducted over a single testing session therefore the long-term retention effects of these performance changes is unknown.
Conclusions
The results of this study indicate that using a portable clinical feedback system may be an effective tool in reducing peak vGRFs and knee abduction angles during a drop landing and transfer task in adolescent females. Future studies should focus on the retention effects of using augmented feedback systems on performance modifications.
Conflicts of Interest
Authors present no conflict of interest associated with this work.