


INTRODUCTION
Glenohumeral joint range of motion (ROM) adaptations in IR and TROM have been identified in elite baseball and tennis players primarily in the direction of internal rotation (IR) and total rotational motion (TROM= External + Internal Rotation ROM).1–5 These changes or adaptations in glenohumeral joint ROM have also been reported in other unilaterally dominant upper extremity sport athletes such as tennis, volleyball players and swimmers as well, but have been studied primarily in baseball pitchers.3,5,6
It is well known that the overhead throwing athlete develops changes in shoulder ROM, specifically a loss of glenohumeral IR.7,8 This loss of IR ROM with an accommpanying increase in external rotation (ER) ROM can place the overhead throwing athlete at risk of injury.8 Previous authors have specified that glenohumeral internal rotation deficit (GIRD) in itself is not necessarily considered deleterious to throwing motion or risk of injury. Rather a change in the total arc of motion between dominant (D) and non-dominant (ND) arms is when GIRD can be pathologic.3,9–12
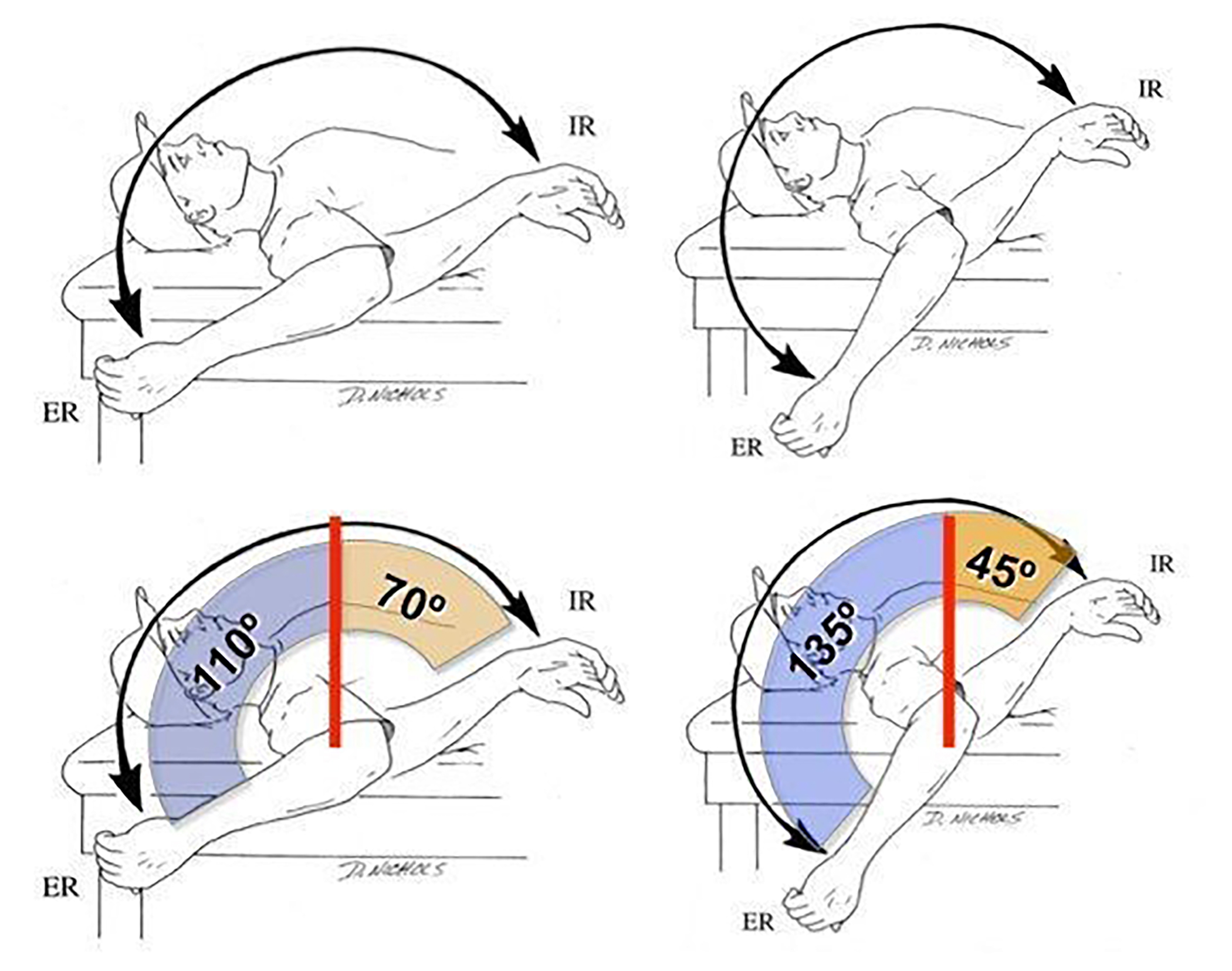
Total arc of motion is defined as the sum of ER and IR ROM (Figure 1) and has been reported to be a total of 160-180 degrees.12 Overhead throwing athletes notoriously have a shift in measured ER and IR ROM, with the D throwing arm presenting with limited IR and excessively increased ER in order to provide the necessary torque required to pitch.13–15 The ability to throw at high velocities requires adaptations to occur within the athlete’s shoulder complex that are not typically seen in the ND side of throwers, or in the shoulders of non‐throwing individuals.16 For example, a baseball pitcher with a D arm total arc ROM (105 degrees of ER + 55 degrees of IR = 160 TROM) versus ND arm (90 degrees of ER + 70 degrees of IR = 160 degrees of TROM) would be considered to have an anatomic GIRD / adaptation and this athlete would not be considered at risk for further shoulder injury due to symmetrical TROM.
.jpg)
Pathologic GIRD is defined as when there is a loss of glenohumeral IR greater than 18°‐ 20° with a corresponding loss of total arc of motion greater than 5° when compared bilaterally.9–13 For example, a baseball pitcher with a D arm total arc (110 + 50 = 160) and ND arm total arc (80 + 70 = 150) would be considered pathologic and at risk for future shoulder or elbow injury.5,13,16
In addition to changes in available ROM, muscle imbalances may occur of the rotator cuff and scapular stabilizers contributing to further asymmetry which relates to control of the throwing motion.13 Increased dominance of internal rotator muscles and impaired recruitment of external rotators, especially in eccentric control, may put throwing athletes at risk for injury.17 The late cocking phase and follow through phases are especially susceptible to excessive tensile load across shoulder structures.14,18–20 Dynamic control and proprioceptive input are critical in maintaining scapulothoracic and rotator cuff stability during the overhead throwing motion.12,14,21–23
Muscle timing and recruitment are key components in maintaining proximal stability for distal mobility during arm motion. Researchers have shown decreased output of the scapular stabilizers (such as the serratus anterior) to occur with dominance of internal rotators (such as the pectoralis major and minor) along with impaired strength of the posterior rotator cuff needed for control and deceleration of the arm in throwing.20,21
Most of the available research has demonstrated normative and descriptive data profiles for shoulder ROM and strength of the adult or older adolescent athlete, whereas minimal research is available for adolescent throwing athletes under the age of 12. Young athletes are often specializing in a single sport at earlier ages, dedicating their time year round to one sport and one position,22 despite the American Academy of Pediatrics recommending a minimum of two months off per year with a minimum of one day off per week to minimize overuse injuries in the adolescent athlete.23 Thus, the authors are aware of the fact that these overuse injuries are beginning to occur at younger and younger ages.24–27 We are less aware, however, of what age young overhead athletes begin to develop glenohumeral rotation deficits and rotational muscle imbalances. This information would be important to rehabilitation professionals working with young overhead athletes to perhaps reduce the risk for injury.26
The purpose of this research was to establish descriptive data by measuring shoulder IR and ER ROM, total arc range of motion (TROM), and isometric strength and determine if differences exist between the D and ND extremity in athletes 12 years of age or younger. Research identifying the descriptive profile of total arc range of motion in healthy, uninjured youth baseball players will allow clinicians and scientists to better interpret findings of preventative evaluations and during the examination of youth baseball players. It was hypothesized that youth baseball athletes aged 5-12 years old would show throwing-related adaptations in shoulder strength and ROM in the D versus the ND arm.
METHODS
Study participants were recruited from a local youth baseball league during opening day festivities prior to the start of the season. Subjects were included if they were between the ages of 5 and 12 and had no current shoulder pain or injury, and no history of shoulder or elbow surgery in either upper extremity. Participants were also excluded if they had any shoulder injury in the prior year that prevented baseball competition or training.
Procedures
All participants were measured on opening day of the 2012 baseball season. Before data collection, the parent/guardian read and signed the informed consent form approved by the institutional review board of Physiotherapy Associates, Exton, PA. Subjects were assigned a number that represented their involvement in this study. This number was used in lieu of their name to minimize the risk and ability of their identity being disclosed to persons other than the primary investigator. After informed consent was signed demographic information was collected (age, arm dominance). Participants were then instructed to report to either a strength or range of motion testing location for evaluation based on convenience. Subjects were measured bilaterally in a random order to prevent any effects of bias for both ROM and strength measures.
For ROM measurement, participants were placed supine on a portable treatment table without a pillow under their head, with the arm in 90 degrees of shoulder abduction and 90 degrees of elbow flexion. Subjects were asked to retract their scapulae bilaterally and then lie in a relaxed position for the duration of the testing. The superior border of the scapula was stabilized in a relaxed position by one hand of the examiner using a thumb on the corocoid process (Figure 3) to prevent/minimize scapular substitution.5,28 From this position the examiner passively moved the subject’s extremity into external rotation until first resistance was encountered (Figure 2). There was no overpressure applied to the extremity at any time. Gravity was used as a constant force to maintain the end-point position similar to the method used by the authors during measurement of glenohumeral joint internal rotation.1–3,6 From neutral rotation the examiner then moved the extremity into internal rotation until first resistance was encountered (Figure 3) using the exact procedure employed for external rotation measurement. A standard method was used with the same therapist collecting all of the ROM and strength measurements. An analog goniometer was then placed along the axial midline of the humerus with one arm vertical representing 0 degrees and the other arm of the goniometer parallel to the lateral border of the ulna. One trial of measurement was utilized to represent the subjects’ ER and IR ROM for this investigation. Bilateral measurement was performed using identical procedures.


Strength measurements were obtained with the use of a hand held dynamometer (Microfet 2, Hoggan Health Industries, Salt Lake City, UT-Figure 4) and recorded in pounds utilizing a “make” test.29,30 The strength tests were performed with the subjects in a standing position with a 3" ½ foam roll under the subjects’ axilla to provide sufficient spacing between arm and body.29,30 D and ND sides were randomly chosen and tested using a coin toss to determine which side was tested first. Internal and external rotation strength were tested in this position in neutral shoulder rotation by the same examiner. The hand-held dynamometer was positioned proximal to the wrist on the dorsal and volar aspect of the distal forearm for external and internal rotator strength testing, respectively. The process was completed bilaterally and recorded in a Microsoft Excel spreadsheet. In a random fashion, external and internal rotation strength in 90 degrees of abduction was also tested with the shoulder placed in the coronal plane. Testing took place in a standing position with the shoulder in 90 degrees of ER and 90 degrees of abduction bilaterally.

Data were stored on a Microsoft Excel sheet and SPSS was used to calculate descriptive statistics as well as compare differences between extremities using dependent t-tests. A Bonneferoni adjustment was applied due to the use of multiple t-tests (7 tests) to establish a level of significance of (p<.007) to minimize the risk of error.
RESULTS
Fifty youth male baseball players age 5-12 years old, mean age 9.02 years + 1.6 were measured in this cross-sectional study. Table 1 presents the available descriptive demographics for the youth baseball study participants.
Range of Motion
Table 2 presents the IR, ER, and TROM data from the 50 subjects included in this study. ER ROM was 102.2±7.7 degrees for the D and 96.6±7.4 degrees for the ND extremity. IR ROM was 34.4±9.0 and 37.5±9.5 for the D and ND extremity respectively. In a similar cross-sectional study of healthy baseball players aged 6-18, Hibberd et al31 also found inter-group ROM differences in players aged 6-10, 11-13, 14-16, and 16-18. Mean TROM was 136.7 ± 12.7 degrees and 134.3 ± 12.3 degrees for the D and ND extremity respectively. There was no significant difference between extremities for TROM. These data produced significantly greater ER (p<.001) and less IR (p<.006) ROM for the D as compared to the ND extremity.
Muscular Strength
Table 3 displays the internal and external rotation strength data for both the neutral and 90-degree abducted testing positions. Mean strength measurements in neutral were 13.6 ± 3.4 and 12.8 ± 3.6 lbs for ER, and 18.0 ± 6.0 and 15.7 ± 4.7 lbs for IR for the D and ND extremity respectively. Mean strength measurements at 90 degrees abduction were 12.3 ± 3.4 and 12.5 ± 4.3 pounds for ER, with 16.3 ± 5.6 and 15.0 ± 5.7 pounds for IR for the D and ND extremity respectively. No significant differences were found in ER strength in the neutral or 90 degree abducted position between the D and ND extremity. In contrast, significantly greater (p<.001) IR strength was found on the D arm in both neutral and 90 degrees of glenohumeral joint abduction. External rotation/internal rotation strength ratios (ER/IR ratio) of the D extremity were 0.76 and 0.75 at neutral and 90 degrees of abduction, respectively. ER/IR ratio for the ND extremity was 0.82 and 0.83 at neutral and 90 degrees of abduction, respectively.
DISCUSSION
Increased glenohumeral external rotation ROM, decreased internal rotation ROM, and maintenance of total rotation of the D throwing arm compared to ND arm in uninjured baseball players has been consistently documented at the professional,8–10,13,28,32–35 collegiate,36,37 high school,31,38,39 and little league levels.11,31,40,41 A consolidated summary of shoulder range of motion in healthy baseball and tennis players from other authors can be found in Table 4.3–5,11,13,28,31,33,34,37–48 In this study, there was no significant difference in TROM in D vs. ND arms but significantly higher ER ROM and lower IR ROM of the D arm (p= .000, .006 respectively). The shoulder ROM findings of this study on youth baseball players with a mean age of 9 are consistent with the established pattern of increased ER and decrease IR. While such ROM characteristics are present in younger age groups, as youth baseball players mature there appear to be gradual yearly alterations in shoulder ROM documented using cross-sectional observations of such populations. Meister et al11 found average external, internal, and total rotational ROM to decrease in both D and ND arms as age increased in healthy youth baseball players aged 8-16. For example, at 8 years of age, Meister et al11 found ER to be 152 and 145 deg, IR as 39 and 42 deg, and TROM as 191 and 187 deg in D and ND respectively, while at 16 years of age ER to be 143 and 137 deg, IR as 35.9 and 41.8 deg, and TROM as 179 and 178 deg in D and ND arms respectively (Table 4). This study confirms the findings of Meister et al regarding symmetrical total rotational motion quantities despite ER and IR ROM differences between D and ND arms. With the exception of ER of the D arm, all rotational shoulder measures were significantly lower in the 16-18-year-old group versus the 6-10 -year-old group (Table 4). Additionally, in a study considering the influence of age and skeletal maturity on shoulder ROM in healthy aged baseball players aged 8-28, Levine et al41 found ER, IR and TROM of D arm to peak in quantity in the 13-14 year group, who were considered to be at a point of maximal growth during skeletal immaturity, versus both the 8-12 and 15-28 age groups. With such ROM measures consistently changing as a youth baseball player matures, the influence of bony and/or soft-tissue structures on shoulder ROM is important to consider.
Multiple studies considering the effect of humeral retroversion on shoulder rotational motion in groups of baseball players of varying skeletal maturity have been conducted, which demonstrate the presence of bony adaptations that account for changes in GIRD, external rotation gain, and TROM.10,28,31,36,37,48 In skeletally immature baseball players, Hibberd et al31 found both GIRD and humeral retroversion to increase with age and concluded humeral retroversion to be a primary source of age-related increases in GIRD. Similar findings in studies of healthy college,36,37 and professional baseball players,10,28 have led to general agreement on bony morphology as the primary influencer of side-to-side shifts in rotational shoulder motion.
This study found no significant differences in isometric ER strength with the shoulder positioned in both neutral and 90 degrees of abduction in the D versus ND throwing arms. Conversely, IR strength in the D arm was 13% higher in neutral and 9% higher in 90 degrees abduction compared with the ND arm (p=.000, 0.001). In a study of risk factors for elbow injury in baseball players aged 9-12, Harada et al49found no significant differences in ER or IR strength (neutral and 90 deg. abduction) between D and ND arms but did find ER strength exceeding 80N and IR strength exceeding 100N to be risk factors for elbow pain (Odds ratios: 4.11, 2.04 respectively). In a comparison of baseball players (average age 15.7) with and without history of shoulder or elbow pain in the previous season, Trakis et al50 found the group with injury history showed increased IR strength of D arm versus ND arm (19% vs. 6%, p < .05). In a population of 11-12 year old baseball players with throwing-related pain, there were no side to side differences in strength or ROM.51 To the authors knowledge, there is little published normative data regarding rotator cuff muscle strength in healthy youth baseball players aged 5-12 and the findings of this study can serve to inform clinicians of descriptive values for such a population.
ER/IR strength ratios have been used as a means for studying rotator cuff muscle balance in the comparison of strength characteristics within throwers D and ND extremities, and between D extremities in groups of throwers.17,42,52–60 In the present study of healthy male youth baseball players aged 5-12, D and ND arms were found to have different ER/IR ratios at neutral and 90 degrees of abduction (0.76 vs. 0.82 and 0.75 vs. 0.83 in neutral, 90 abd for D and ND arms respectively). These findings align with the ratios published by Ellenbecker et al56 in a study of healthy elite junior tennis players aged 12-17. Ellenbecker et al found isokinetic ER/IR strength ratios at 90 degrees abduction of 0.69 for the D arm and 0.82 for the ND arm.56 With no significant differences found between ER strength in D versus ND arms in the present or Ellenbecker et al56 studies, dissimilar ER/IR strength ratios in the extremities is explained by relative increase of IR strength in the D compared to ND extremity. Byram et al53 reports the majority of studies of throwers D arm ER/IR strength ratios to range from 0.60-0.80, although research on professional baseball pitchers reveal higher ratios ranging from 0.83-1.19.17,52,58–60
Currently, there is minimal published data to inform clinicians of normative values of bilateral shoulder external and internal rotation ROM and strength in youth baseball players 12 years of age and younger.11,31 As stated earlier, shoulder ROM among throwers takes on a consistent pattern across baseball players of all ages with a characteristic ER gain, IR loss, and TROM maintenance in the D arm of such athletes. The findings of this study on youth baseball players with a mean of nine years of age, help to strengthen understanding of the age ranges such ROM patterns can be expected to present clinically. If a youth athlete should present with throwing-related pain, routine ROM measures can help to guide intervention strategies including ROM restoration programs including stretching and manual therapies if indicated.
The use of hand-held dynamometers in the evaluation of isometric rotator cuff strength testing is clinically feasible, time efficient, and offers an objective means of tracking strength changes. For youth baseball players, clinicians may expect increased IR and equivalent ER muscle strength of the throwing arm versus non-throwing arm. These characteristics may be quantified using ER/IR ratio calculations to identify throwers falling outside of the accepted 0.60-0.80 strength ratio. Rotator-cuff specific strengthening programs can be employed to increase ER/IR ratios and have been shown to be effective for such goals.54 Additionally, the monitoring of ER/IR ratios may guide clinicians on appropriate timing of return to throwing following throwing-related injury.53
The limitations of this study include a relatively small sample size of 50 participants ranging from 5-12 years of age. As a result, the authors were unable to run ROM and strength analyses of specific age groups within this broad age range of athletes up to seven years apart. Additionally, the influence of descriptive information including height, weight, years of baseball experience, and injury history on the ROM and strength measures collected is unknown. All strength and ROM measures were taken in a single trial which may increase the risk of measurement error.
CONCLUSION
The results of the current study indicate that youth baseball players with a mean age of 9.02 years (age range 5-12) demonstrated no significant difference in total rotation ROM between extremities, however had significantly greater dominant arm ER and significantly less dominant arm IR. There were no significant differences in ER isometric strength between extremities both in neutral and in 90 degrees of abduction. However, significant increases in dominant arm IR isometric strength were identified in both neutral and 90 degrees of abduction. These results are consistent with findings reported in many other studies in older, more developed and mature overhead throwing athletes, indicating sport specific ROM and strength adaptations. These data can assist clinicians who work with athletes in this population and age range to inform prevention and treatment of overuse throwing injuries.
Conflicts of Interest
The authors certify that they have no affiliations with or financial involvement in any organization or entity with a direct financial interest in the subject matter or materials discussed in this article.
Acknowledgements
The authors would like to thank Jessica Endo, DPT, Sports Resident at Los Gatos Orthopedic Sports Therapy for her contribution with helping us bring this to publication. Without her work, effort and persistence, we would not have been able to accomplish the endeavor.