INTRODUCTION
A popular topic of sports medicine and performance enhancement research has been the pre-participation or pre-season athletic screen. Screens are often performed prior to the commencement of a training program or sport season to identify muscle imbalances, weaknesses, or movement patterns that may increase an individual’s risk for injury.1–7 Various methods have been used to identify asymmetries in athletes. Muscular strength asymmetries and balance have been a popular topic of research, and further investigation is warrented.8–17
The Functional Movement Screen (FMS™) is a screening tool used to identify dysfunctional movement patterns. The assessment consists of seven individual tests (deep squat, hurdle step, in-line lunge, shoulder mobility, active straight leg raise, trunk stability push-up, and rotary stability) which are scored on a scale from 0-3, with a possible composite score of 21 (higher scores indicative of better movement competence).18,19 Of the seven individual FMS™ tests, five compare the right side to the left side (hurdle step, in-line lunge, shoulder mobility, active straight leg raise, and rotary stability). This comparison allows for asymmetries, if present, to be identified. A participant may score a 3 on the right side, while scoring a 1 or 2 on the left side. When there is an asymmetry that occurs, the lower of the two scores is recorded for that individual test. If pain is present during the screen, the subject is scored as a 0 for that particular sub-test.18,19 The FMS™ has been used to predict injury risk and performance outcomes across populations, including professional American football players,20,21 elite track and field athletes,22 Marine officer candidates,23 adolescent children,24 young active adults,25 high school baseball players,26 junior and high school ice hockey players,27 high school athletes,28 and female collegiate athletes.29 Research involving professional American football players has identified individuals scoring lower than a 14 on the FMS™ are 11 times more likely to become injured than individuals scoring greater than or equal to 15.20 This research was one of the first to establish a cut-off score for injury risk using the FMS™. A recent meta-analysis has indicated there is conflicting evidence regarding the specific cut-off score used to predict injury risk.30 There are relatively few studies supporting the notion that individuals scoring lower than a 14 on the FMS™ are more likely to become injured than individuals scoring greater than or equal to 15.30 Thus, it appears that comparing the FMS™ composite score of an individual to a cut-score and associated injury risk is in question at the present time. Due to the conflicting nature of the previous research examined in the meta-analysis, additional research needs to be completed to examine the application of FMS™ scores for injury risk prediction.
One area of interest that has drawn limited research attention is the relationship between asymmetries identified during FMS™ testing and injury rates with participation in sport. Research on American football players with an FMS™ detected asymmetry had a 1.8 times greater risk for injury than those without an asymmetry.21 A 2016 study examined total FMS™ scores and the presence of asymmetries in NCAA Division II athletes and found that those with an asymmetry or individual test score of 1 were 2.73 times more likely to sustain an injury.31 A study performed with 237 elite junior Australian football players, identified that if participants demonstrated one or more asymmetry, they experienced a moderate increase in their risk of injury (hazard ratio = 2.2 relative risk = 1.9; p = 0.047). Additional analysis identified that the presence of two or more asymmetrical sub-tests was associated with an even greater increase in risk of prospective injury (hazard ratio = 3.7; relative risk = 2.8; p = 0.003).32 As such, asymmetries discovered during FMS™ testing may be useful in predicting injury risk in successive sport participation.
Despite these findings, no research has examined the effect of previous athletic participation on an individual’s performance on the FMS™, specifically identification of asymmetries. Therefore, the objective was to determine normative FMS™ scores, report frequency counts for FMS™ asymmetries, and determine if the number of sports seasons and number of different sports an individual participated in during high school varied between university students that showed FMS™ identified asymmetries. Since the FMS™ examines mobility and stability in multiple planes of movement, the researchers hypothesized that the various biomechanical demands of playing multiple sports may lead to fewer FMS™ asymmetries.
METHODS
Study Design
This study employed a retrospective analysis examining if the number of sport seasons and number of sports participated in high school was different between university students who had symmetrical or asymmetrical movements during FMS™ testing. Prior to the FMS™ testing, each participant completed a written questionnaire that included age, which school-sponsored high school varsity sport(s) the participant played in high school, and how many seasons the participant played each sport. At the time of study, participants were engaged in moderate-to-vigorous group exercise sessions each week as part of a university wellness class. Participants were excluded from the study if they had any injuries preventing them from engaging in the class exercise sessions.
Participants
A convenience sample of 100 healthy participants (57 females, 43 males) between 18 and 26 years of age (mean ± SD = 19.5 ± 1.7 years) were recruited from a university-level introductory wellness class. Participants included in the study participated in regular physical activity as part of the university wellness class, which consisted of two structured moderate-to-vigorous group exercise sessions each week. Any additional exercise performed by the participants outside of the university class was not assessed. Exercise sessions were a combination of circuit resistance training and cardiovascular exercise. Exclusion criteria included: any reported recent (within the prior six weeks) musculoskeletal or head injuries that may have affected their overall performance on the FMS™, which was assessed by a questionnaire. All participants provided written informed consent prior to completing the questionnaire and participating in the FMS™ screening. The study was approved in advance by the Institutional Review Board.
Procedures
The lead researcher was blinded to questionnaire results until after FMS™ testing was completed. The FMS™ has demonstrated acceptable interrater and intrarater reliability, with interrater test-retest intraclass correlation coefficients (ICC) at 0.6, and intrarater ICC at 0.946. Interrater reliability (Kappa) for individual test components of the FMS™ has demonstrated moderate to excellent agreement (0.40-0.95).33–35 All scoring was performed by the FMS™ Level 1 Certified lead researcher. The participants were asked to wear their usual workout clothing and athletic shoes. Each participant performed each of the seven tests (deep squat, hurdle step, in-line lunge, shoulder mobility, active straight-leg raise, trunk stability push-up, and rotary stability) three times.18,19 Each time the participant performed each of the seven tests, they were scored on a scale of 0 to 3.18,19 A score of 0 indicated that the participants reported pain during the performance of the specific test. A score of 1 indicated a failure to complete the test or a loss of balance during the test. A score of 2 indicated completion of the test, but with a movement compensation. A score of 3 indicated completion of the test, without a movement compensation. For each of the seven tests, the highest score of the three trials was given to the participant. For the tests with a bilateral assessment component (hurdle step, in-line lunge, shoulder mobility, active straight-leg raise, and rotary stability), the side with the lowest score was used for data analysis. An asymmetry within the FMS™ was defined as achieving an unequal score on any of the tests that assessed right versus left movements of the body. If an asymmetry was present, the researchers recorded it along with the participants’ total FMS™ score. The sum of the seven assessments provided an overall maximum score of 21. Three of the tests (shoulder mobility, trunk stability push-up, and rotary stability) within the FMS™ also have a clearing procedure associated with them. For each of the clearing procedures, the participant was given a positive if they reported pain during the clearing procedure or a negative if they reported no pain during the clearing procedure. Total FMS™ scores and number of asymmetries were calculated and compared to the results on the questionnaire for each participant for statistical analysis.18,19
Statistical analysis
Statistical analysis was conducted using IBM SPSS version 24 (IBM Corp., Armonk, NY). Summary analysis, Pearson correlation was utilized to investigate the relationship between number of sports played and number of sport seasons. Shapiro Wilk test for normality, and Mann Whitney U test was employed to investigate group differences in number of sports played with a priori alpha established at 0.05.
RESULTS
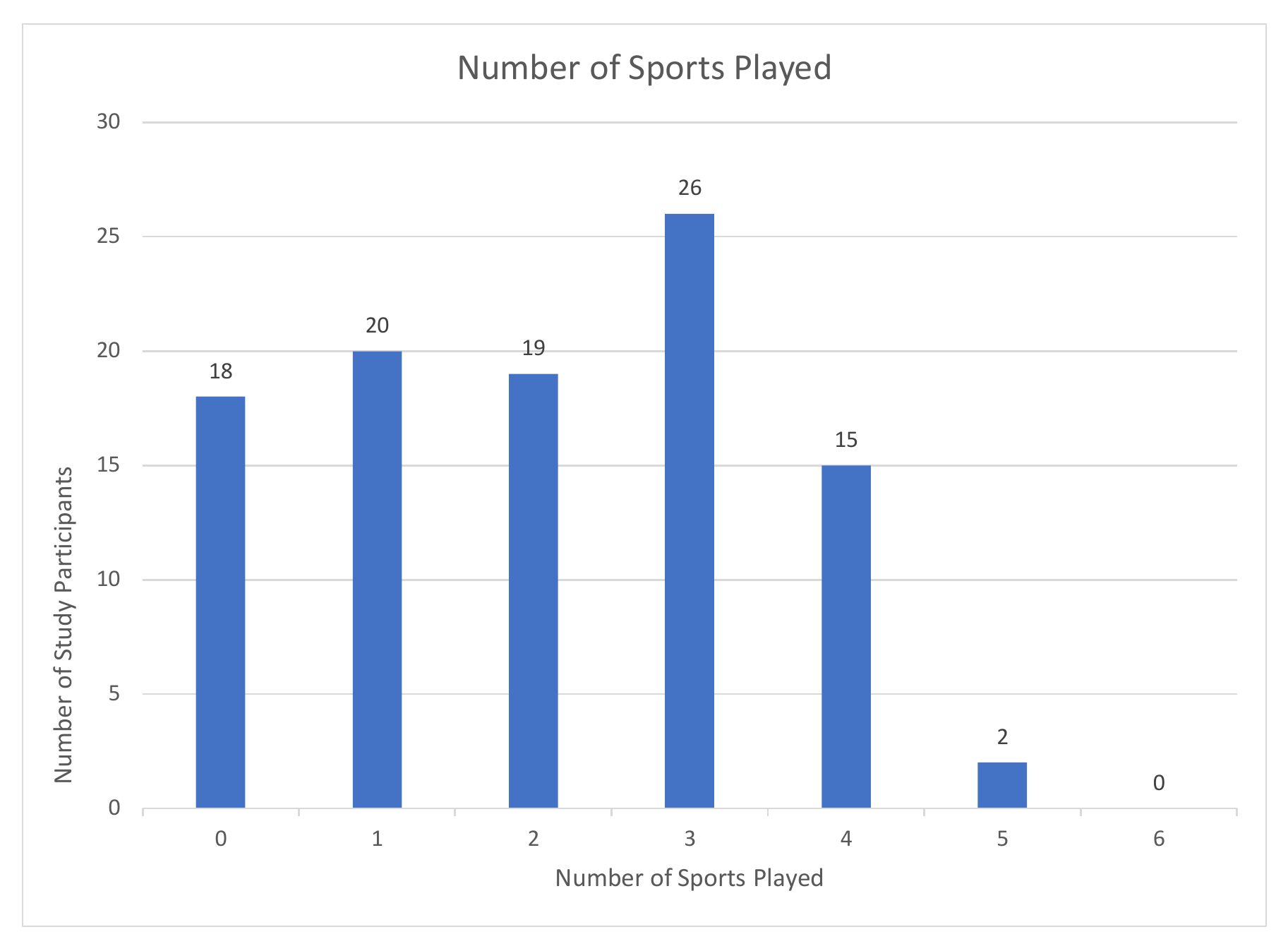
One hundred college-age study participants participated in the analysis including 43 males and 57 females. The study group (n=100) participated in diverse sports and a variety of sport seasons. FMS™ scores of the study participants ranged from 7 to 19 with the highest frequency scoring 16 (n = 19) on the FMS™. The mean score for the study sample was 14.40. FMS™-detected asymmetry was observed in 57 of the 100 study participants (28 males, 29 females) with multiple asymmetries occurring in 22 participants. Of the 57 participants with at least one detected asymmetry, nine were identified during the FMS™ hurdle step, 24 in the lunge, 25 in shoulder mobility, 10 in straight leg raise, and 18 in rotary stability.
_were_asked_to_indicate_the_number_o.png)
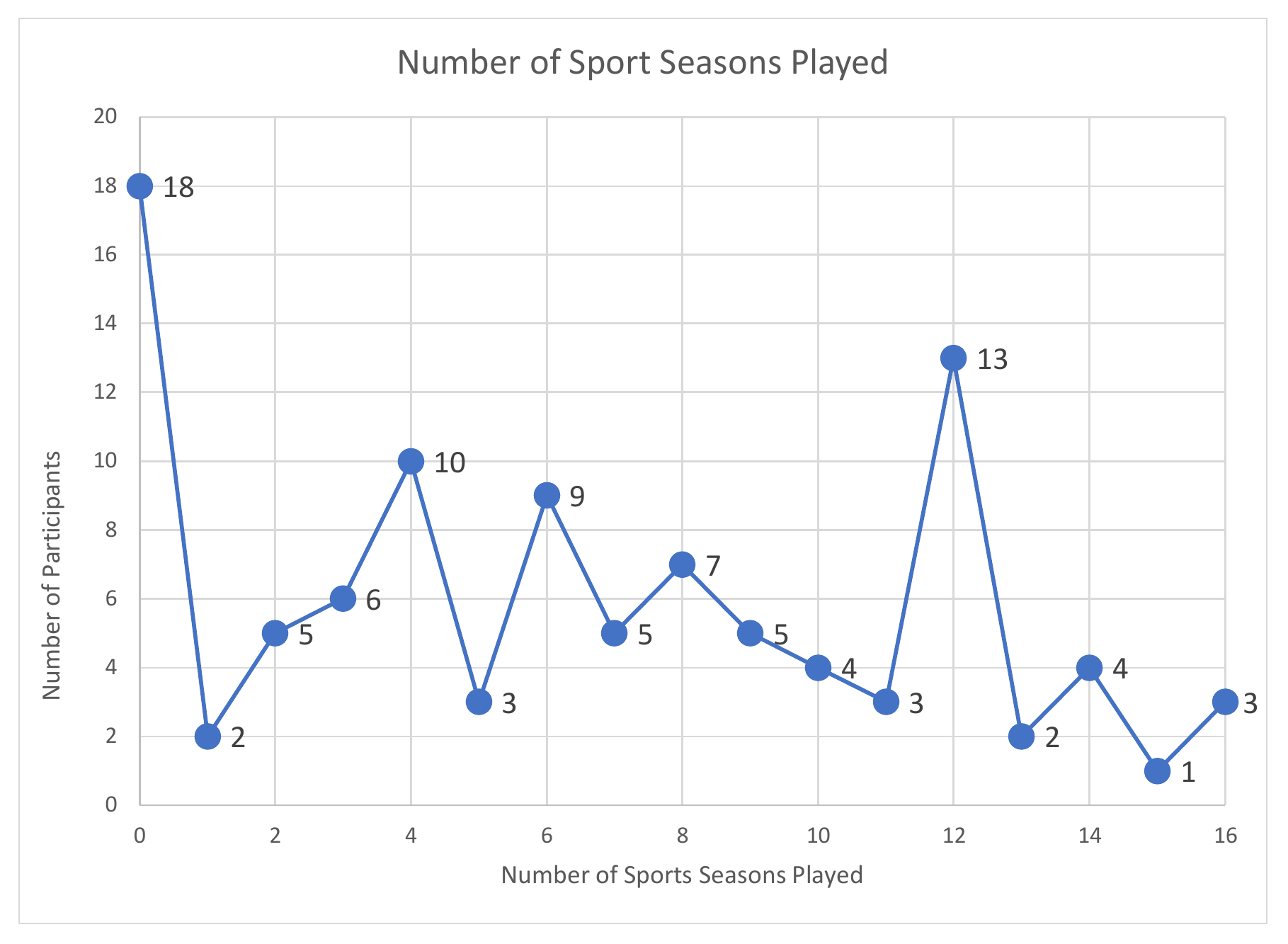
_were_asked_how_to_indicate_the_num.png)
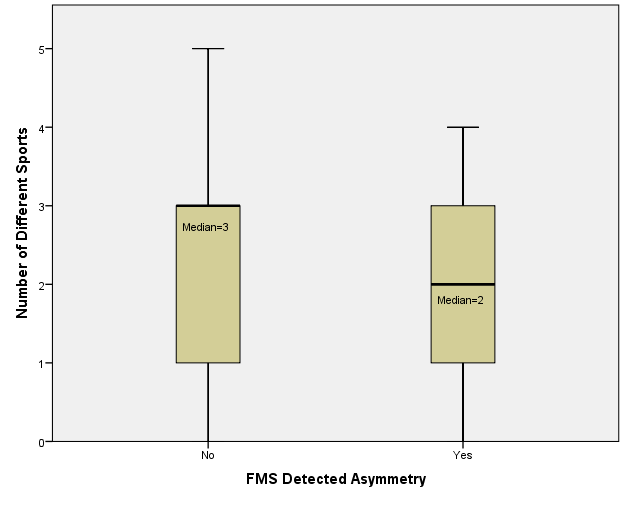
Shapiro-Wilk test was conducted to examine the normality of the distribution of FMS™ scores. The distribution for all FMS™ scores was found to be non-normal (p=0.03). Pearson correlation analysis revealed a statistically significant relationship between the number of sports played (r = .286, r2 = .08, p < 0.01) and FMS™ total score. While statistically significant, the number of sports accounted for only 8% of the variability in FMS™ total score. Independent samples Mann-Whitney U test was conducted to evaluate whether the number of sports were lower, on average, for participants with an FMS™ detected asymmetry compared to those participants without and FMS™ detected asymmetry. Results indicated that participants without an FMS™ detected asymmetry played three sports as opposed to two sports for participants with a detected asymmetry (U = 946.5, z = -1.98, p = 0.047), thus rejecting the null hypothesis (see Figure 3). Participants who did not display asymmetries played more sports than their counterparts with asymmetries. Combined with the correlational analysis between number of sports and number of sport seasons, data appeared to indicate that movement variety is related to improved FMS™ total score and reduced asymmetries.
_based_on_fms_detected_asymmetry_(iv).png)
DISCUSSION
The objective was to determine among university students normative FMS™ scores, report frequency counts for FMS™ asymmetries, and determine if the number of sports seasons and number of different sports an individual participated in during high school varied between groups that showed FMS™ identified asymmetries.
The mean FMS™ score of the current sample of 100 college-age students was 14. Other studies have reported mean FMS™ scores in active participants ranging from 13-16.2,25,36–38 While the sample mean was consistent with other reported data, it is important to note that the samples vary in demographic characteristics. Although many in the current study reported a history of sport participation, data was not collected on the sample’s current physical activity level or their present status as a collegiate athlete.
In the current study sample of 100 participants, the FMS™ detected at least one asymmetry in over half of the population (n = 57). While research has examined the possible association of FMS™-detected asymmetry and subsequent injury,31 minimal research was found that attempted to establish normative data for the prevalence of FMS™ detected asymmetry in a population of recreationally active college age adults.25
While a low, statistically significant relationship between both the number of different sports played and total FMS™ score was found, the number and different sports played could only explain a small part (8%) of the total FMS™ score. This is potentially related to the size of the study group, which limits the application of this finding without further investigation. There was a significant difference between the number of different sports played and whether FMS™ asymmetries existed, but the clinical significance of this remains unknown. Together, these results support the notion of increased levels of physical activity and the various biomechanical demands of different sports may lead to improved functional movement. Prior research has demonstrated that higher levels of exercise participation were associated with higher FMS™ scores.39 The results of this research highlight that not only does the level of activity influence functional movement, the diversity of movement through various sports may also play a role.
The current research may support current efforts by researchers examining the impact of single sport participation in young athletes. Literature suggests that those athletes who play one single sport or engage in year-round training longer than eight months per year have an increased risk of injury, burnout, and a loss in developing lifetime sport skills.40,41 The results show that those students who participated in varying sports were more likely to have higher functional movement screen scores and fewer asymmetries. This supports the notion that young athletes participating in more sports may improve movement quality. The authors offer this interpretation with caution as the study was not specifically designed to assess the effect of sport specialization on FMS™ scores. Future research should examine this relationship specifically.
LIMITATIONS
One of the limitations of this study was that the amount of time that had passed since each participant graduated high school was not controlled. The average age of study participants was 19.5 years (range 18-26 years) and suggests that most study participants may not have been far removed from high school sport participation, however some had not participated for multiple years. Another limitation of the study is that previous musculoskeletal injuries or surgeries were not assessed. Additionally, the researchers did not determine specific sport specialization. Finally, although all participants were engaged in two structured moderate-to-vigorous group exercise sessions each week as part of their university wellness class, physical activity frequency and intensity outside of class was not assessed. Some of the participants may have also been engaged in physical activity outside of the university wellness class, such as participating in club or recreational sports.
CONCLUSION
The results of the current study indicate that individuals that played more than one sport and for multiple sport seasons exhibited improved symmetry in their performance on the FMS™. This is important in that it demonstrates that college aged students who participated in a wider variety and in an increased volume of sport activities in high school were less likely to have FMS™-detected asymmetrical dysfunction in their movement patterns in college. Current sport culture tends to emphasize sport specialization; however, encouraging athletes to engage in more than one sport may reduce their likelihood of FMS™-detected asymmetry. Having athletes participate in various sports may contribute to more symmetrical movement performance and minimize injury risk throughout their careers. Coaches, athletic trainers, and strength and conditioning specialists at any level may benefit from gathering data on their athletes to understand how past participation in sports may affect current performance, movement quality, and injury risk. Identifying asymmetries early may also assist coaches and athletic trainers in customizing training programs to reduce athletes’ injury risk and asymmetrical function.
Conflicts of Interest
The authors do not have any conflicts of interest to report.