
Introduction
Athletic lower extremity injuries are common,1–3 with ankle sprains being the most prevalent.3,4 Nearly 75% of athletic ankle sprains are recurrent,5 burdening the sports medicine provider and health care system.6,7 Research has suggested that limited ankle dorsiflexion (DF) range of motion (ROM) increases ankle and overall lower extremity injury risk.8–11 In addition, limited ankle DF is a common injury sequela. Therefore, sports medicine providers have a need for easy to use on-field ankle screens.9,12
Ankle DF ROM has conventionally been assessed in the open-chain position; however, open-chain ankle testing has poor reliability.13 Furthermore, athletic movement and competition are performed in the closed-chain position.13,14 Normal ankle DF allows for lower extremity advancement, running, and proper jump landing.11,15 Thus, performing closed-chain ankle measurements allows for more functional clinical testing.10,16 Previous closed-chain ankle DF testing has been performed in the half kneeling position17 and in a modified lunge position both with high reliability and validity.18,19 However, these tests require other devices, such as an inclinometer, which are not always readily available.20 This decreases the utility of those tests, as well as the ability of sports medicine providers to effectively and efficiently screen ankle DF. A screen is used to quickly identify if there is a potential problem whereas a measure requires equipment and gives a numerical result. As a result, there is a need for an ankle DF screen that requires minimal equipment and can be implemented quickly and efficiently. Researchers have examined the reliability and validity of a novel ankle DF screen, but used half kneeling dorsiflexion as the referent standard.21 Since the ankle dorsiflexion screen is in the standing lunge position, additional analysis comparing measure in that position is warranted.
The purpose of this study was to determine the reliability and discriminant validity of a novel closed-chain DF ROM test, the standing ankle dorsiflexion screen (SADS). It was hypothesized that the SADS would have high reliability and discriminant validity.
Methods
Subjects
A convenience sample of university students was utilized. Subjects were recruited using fliers on a university campus. To be included in the study, subjects needed to be over 18 years of age and ambulatory without an assistive device. Exclusion criteria consisted of participants with a previous lower extremity orthopedic surgery, current pain or injury, or diagnosed neurological disease. Informed consent was obtained from each subject prior to data collection. The University of Evansville’s Institutional Review Board approved study procedures.
Modified Lunge ROM Measurement
The modified lunge position (Figure 1) was used for the discriminant measurement.18,19 Closed-chain ankle DF ROM was measured using an electronic inclinometer (Clinometer Android App version 2.4 by PlaincodeTM on Samsung Galaxy s9) in a standing modified lunge position with the subjects in a tandem heel to toe stance (Figure 1).18,19 For balance, participants held a dowel rod in the contralateral hand. The inclinometer was placed two centimeters below the inferior aspect of the tibial tuberosity on the back lower-limb. Prior to ankle DF testing, subjects were instructed to drop their back knee as far down and forward as possible while taking the back knee as far as possible beyond the back toes, without lifting the back heel. The raters then recorded the dorsiflexion measurement in degrees from tibial vertical for each trial.17

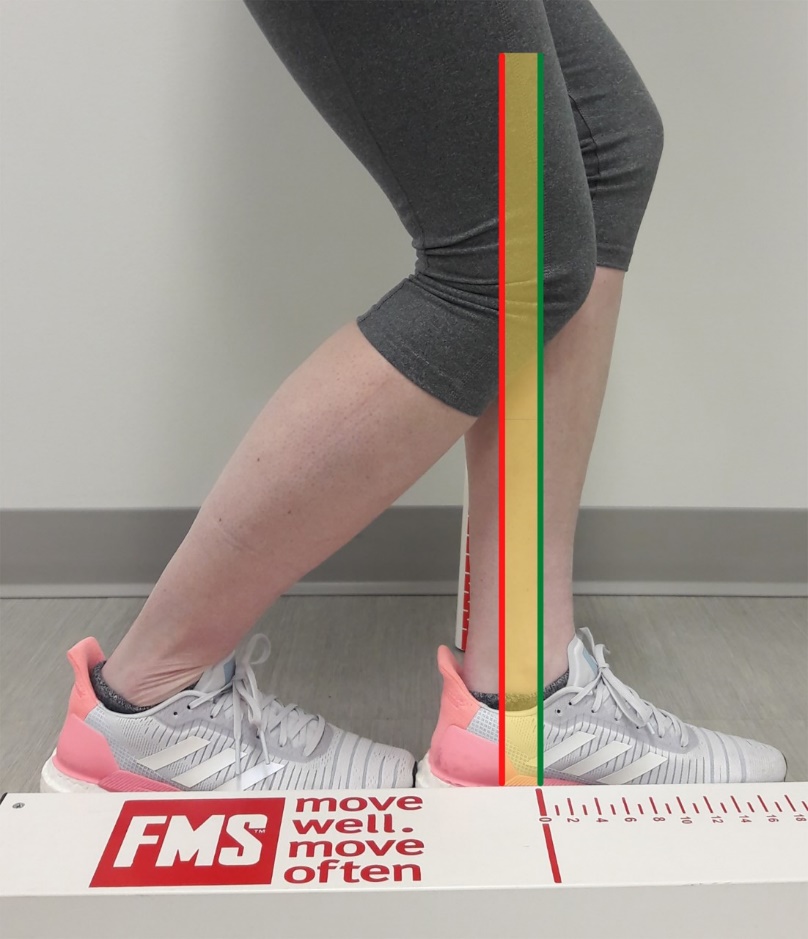
Standing Ankle Dorsiflexion Screen
The SADS was completed using the same position for the modified lunge measurement. The back ankle DF was scored by identifying how far forward the back knee moved in relation to the front medial malleolus. The SADS was scored on an ordinal scale of three categories, behind, within, and beyond (Figure 2).

Ankle Range of Motion Measurements and Screening
Seven raters were utilized for all measurements; each rater was a physical therapist who specialized in outpatient orthopedics and sports medicine. All raters were trained prior to ankle DF measurements that consisted of demonstration and verbal instruction by an instructor who helped develop the screen and had 20 years of orthopedic physical therapy experience. Following the initial demonstration, each rater performed at least three trials with feedback from the instructor. This was repeated and compared to the instructors’ measurements until the instructor determined that the measurement was being taken according to the instructions.
Upon arrival of each subject, their age, height, and weight were recorded. Each subject was randomly allocated through a coin flip to first be measured with the modified lunge or SADS. The modified lunge ROM and SADS category measurements were taken two times per ankle with five minutes between measurements to prevent a treatment effect.22 Two raters measured ankle DF ROM using the modified lunge position. Four raters measured ankle DF via the SADS categories of behind, within, and beyond. All raters were blinded to other rater’s measurements.
Statistical Analyses
Descriptive statistics (age, height, weight) were calculated for subjects using means ± standard deviations. Each ankle was analyzed independently. The intraclass correlation coefficient (ICC 2,2) with a 95% confidence interval was used to determine interrater reliability for goniometric ROM measurements where a score of less than 0.40 was deemed poor, 0.40 to 0.59 moderate, 0.60 to 0.74 good, and greater than 0.75 excellent.23 Kappa coefficients were utilized to determine interrater reliability for the SADS categories, where <0.40 was deemed poor, 0.40-0.59 moderate, 0.60-0.74 good, and >0.75 excellent.23
The modified lunge measurements in degrees of dorsiflexion ROM were then averaged between trials. The SADS behind and within categories were dichotomized into one category (behind), while beyond remained the same. Discriminant validity of the SADS categories was assessed with an independent t-test (p<0.05), using the mean values on the modified lunge ROM of the behind and beyond categories. A significant difference in modified lunge ROM between the behind and beyond categories would indicate that the screen can discriminate between individuals with satisfactory ankle dorsiflexion and individuals with limited ankle dorsiflexion. All analyses were conducted in SPSS 24 (IBM SPSS Statistics for Windows, Version 24.0. Armonk, NY: IBM Corp).
Results
The convenience sample consisted of 37 ambulatory subjects (74 ankles), including 27 females (age: 23 ± 1.1 years; height: 167.2 ± 10.2 cm; body mass: 66.9 ± 11.5 kg) and 12 males (age: 22.9 ± 0.7 years; height: 178.3 ± 9.1 cm; mass: 77.6 ±10.3 kg). The interrater reliability was excellent for the modified lunge electronic inclinometer measurements, with an ICC value of 0.95 (95% CI: 0.92-0.97). The kappa coefficient was high for the SADS categories (range: 0.61-0.81), with percent agreement ranging from 86 to 94% (Table 1).
There was a statistically significant difference in closed-chain ankle DF ROM between the behind and beyond categories regardless of rater or trial analyzed (behind: 41.3° ± 4.7°; beyond: 51.8°± SD 6.1°, SEM 1.36, p<0.001).
Discussion
Limited ankle DF is an injury risk factor and common sequela after injury.3,4 Many ankle DF measurement techniques are not performed in a standing position and require expensive equipment.13,20 Thus, there is a need for an easy to administer ankle screen that requires no equipment. The purpose of this study was to determine the reliability and discriminant validity of a novel closed-chain DF ROM screen, the SADS. Supporting the hypothesis, the SADS was observed to have excellent interrater reliability and discriminant validity. Furthermore, there was a distinct DF ROM difference between the subjects with behind and beyond SADS nominal scores.
The SADS demonstrates discriminant validity. In this study, a digital inclinometer was used. Venturni et al.24 compared the reliability of ankle DF measurement using both a standard bubble goniometer and a digital inclinometer. The results indicated high (ICC=0.83) interrater reliability for the digital inclinometer and moderate (ICC=0.72) interrater reliability for the bubble goniometer.24 This corroborates the decision to study the SADS discriminant validity with an inclinometer. A significant difference in modified lunge ROM between the subjects in the behind and beyond categories was observed, though the mean for the behind category was higher than expected.
Using a functional closed-chain position for ankle screening was found to have high reliability compared to the modified lunge tests. This supports previous research in which a functional closed-chain position was found to have the greatest reliability.22,25,26 Munteanu et al.22 found that ankle DF measurements in a knee extended weight-bearing position had high interrater and intrarater reliability in both novice and experienced raters.22 Five positions for measuring DF were compared by Krause et al.,25 with the modified lunge having the greatest intrarater (ICC=0.88-0.89) and interrater (ICC=0.82) reliabilities. The authors concluded that the modified lunge position may best assess end-range ankle DF.25 This highlights the fact that performing an ankle screen in a functional closed-chain position may best assess potential differences in ankle DF ROM.
Closed-chain ankle DF measurements in the modified lunge were similar to previous studies.8,21,27,28 The SADS behind score mean was 41 degrees. Malliaras et al.8 found an increased risk of patellar tendinopathy was associated with less than 45 degrees of closed-chain DF in volleyball players. Athletes with repeated ankle sprains have been observed to have decreased ankle DF ROM.14,29 The SADS beyond score mean was 51.8 degrees. Driller et al.27 observed that healthy subjects demonstrated over 50 degrees of ankle DF during the weight-bearing lunge test. Dill et al.28 found that healthy subjects with normal ankle motion had 51 degrees DF in the weight-bearing lunge position, while limited ankle DF subjects had 39 degrees of ankle DF. In the study previously examining the reliability and validity of the SADS using half kneeling dorsiflexion as the referent standard, there were differences between DF ROM measurements.21 The half kneeling DF ROM measurements were 33.5 ± 2.0 degrees for behind, 38.6 ± 1.2 degrees for within, and 43.0 ± 0.78 degrees for beyond compared to the standing lunge measurement of behind 41.3° ± 4.7° and beyond 51.8°± 6.1.21 However, the reliability was similar in this study ranging from 0.61 to 0.81with percent agreement from 86% to 96%.21
There were limitations in this study. This study was limited to subjects who were all injury-free at time of testing and were college aged students. However, these participants may have had chronic ankle instability, chronic Achilles tendinopathy, or plantar fasciitis, which may demonstrate long-term ankle or foot impairment. Therefore, the generalization of results outside these ages and to subjects current ankle and/or lower extremity injuries is not possible. Further research should include diverse age ranges, sports, and individuals with ankle and/or lower extremity injury to increase external validity. Additionally, prospective studies are required to determine the SADS injury risk identification ability.
Conclusion
The SADS is a reliable and valid ankle screen for assessing closed-chain ankle DF ROM. Ankle DF ROM differences between the subjects with SADS nominal scores behind and beyond, were significantly different. The SADS can be used as a quick and efficient closed chain ankle DF ROM screen.
Conflict of Interest Statement
Drs. Kiesel and Plisky have equity in Functional Movement Systems LLC who owns the rights to the ankle screen used in this study. Other authors have no conflicts of interest.
Acknowledgements
Funding provided through the Ridgway Student Research Award from the University of Evansville