Introduction
Increased valgus loads at the elbow joint while pitching has been shown to lead to medial elbow instability, chondral degradation at the radial head and capitellum as well as at the olecranon, and ulnar collateral ligament injury.1–8 The increased valgus loading produces tensile stresses along the medial elbow as well as compressive and shear forces along the lateral and posterior elbow.3,8–11 This development is a result of the inability of the elbow to produce sufficient varus torque to balance the accumulating valgus torque created by increasing valgus loads.8–11 Elbow valgus loading is at the most extreme when the pitching shoulder is in maximum external rotation during the late cocking and early portion of the acceleration phase.3,8–11
The accumulation of valgus loads can subjugate the ulnar collateral ligament (UCL) to injury either through a sudden rupture or prolonged repetitive stress.3,12 Specifically, pitchers are highly vulnerable to increased valgus loading and are at a higher risk to develop medial elbow pathology and undergo a UCL reconstruction 5.9 times greater than their non-pitching counterparts.13 Epidemiological studies demonstrated that the average rate of UCL surgeries performed in Division 1 baseball following the 2017 season occurred at rate of 0.86 surgeries per collegiate program with 85.8% of those surgical cases being pitchers.13 Additionally, the increased valgus loading will also increase the stress along the cartilaginous structures of the capitellum and the posterior-medial aspect of the olecranon leading to lateral compartment chondrosis and posterior-medial impingement during the deceleration phase.8,11
Aguinaldo et al.,7 found that kinematic variables such as early trunk rotation, increased shoulder external rotation (ER), and decreased elbow flexion have been shown to increase valgus loads at the medial elbow.7 Additionally, Di Giovine et al.,14 demonstrated that increased shoulder abduction during the late cocking phase resulted in increased valgus loading at the medial elbow.14 Furthermore, Werner et al.,15 looked at 37 kinematic and kinetic variables and found that pitchers with increased shoulder horizontal adduction angular velocity and shoulder abduction angle at lead foot contact, elbow angle at peak valgus stress and peak shoulder external rotation torque had increased elbow valgus loading during the late cocking phase.15 In addition to these established kinematic predictors of elbow valgus loading, lower extremity range of motion (ROM) also contributes to the kinetic chain of the pitching motion.16–18
Specifically, restrictions in hip rotational ROM can influence performance and increase risk for medial elbow pathology.7,16,19,20 Restricted lead and trail hip ROM can affect the pitcher’s shoulder positioning.21,22 Decreased hip ROM causes the pitching arm to be out in front of the pitcher’s body forcing the pitcher to throw across their body.22,23 This scenario theoretically leads to a dampening of the transfer of energy from the lower extremities. The results lead to a potential reliance on the upper extremities to produce force needed to achieve ball velocity, leading to increased medial elbow valgus torque.21,22 Too much hip motion and the pitching arm will lag behind the already rotated trunk.22,23 In this scenario, the overhead athlete will compensate for early trunk rotation by increasing shoulder ER ROM. Increased shoulder ER ROM has been associated with increased valgus loads at the medial elbow.7,21,22
Given the interaction between hip motion and pitching mechanics, a salient link may exist between restrictions in hip rotational ROM and medial elbow dysfunction. Thus, the purpose of this exploratory study was to measure the relationship between hip rotational ROM and kinematic variables that influence elbow valgus loads in Division 1 collegiate pitchers. Determining if a relationship exists between hip ROM and valgus forces at the elbow may aid in developing interventions to address poor pitching mechanics, while improving pitching performance.
Materials and Methods
Participants
A total of seven Division 1 collegiate baseball pitchers (mean age, 19.57 1.1 years; mean height, 1.89 .6 cm; mean weight, 93.3 6.8 kg) consented to participate in this study. (Table 1) Five subjects were right-handed dominant and two subjects were left-handed dominant. All subjects were healthy at the time of testing, currently active, reported no trunk, upper or lower extremity injury in the past six months or had history of upper or lower extremity surgery. Prior to participation, all subjects signed a written informed consent approved by the University of Florida Health Science Center Institutional Review Board (IRB-01).
Procedures
All subjects were tested prior to the beginning of preseason workouts. All hip rotational ROM measures were performed by the same two American Physical Therapy Association (APTA) board sports certified specialist physical therapists. One to stabilize and one to record measurements. Hip ROM testing occurred prior to kinematic testing at the University of Florida Human Dynamics Laboratory.
Hip Rotational ROM Measurements
Hip ER and internal rotation (IR) ROM measurements were taken with a bubble inclinometer while the subject was placed in a prone position with hip of interest in 0 degrees of extension and abduction with knee in 90 degrees of flexion.24,25A two-examiner method was utilized. One examiner placed one hand on the testing hip greater trochanter and pelvis to minimize excess movement and used the other hand to grip the subject lower leg to passively move the hip until first resistance was detected. The second examiner placed the bubble inclinometer proximal to the medial malleolus aligned with the shaft of the tibia to record ER and IR ROM. Total hip rotational ROM was calculated as the sum of hip ER and IR ROM. This measuring method has shown good interclass correlation (ICC = .98).24
Pitch Biomechanics Preparation
Motion capture set-up was based on previously validated methods.26,27 Motion analysis was captured with a high-speed, 12-camera optical motion capture system (Motion Analysis Corp, Santa Rosa, California). Data were captured at 200 Hz. Fifteen reflective markers were applied bilaterally at the lateral tip of the acromion, lateral humeral epicondyle, greater trochanter, lateral femoral epicondyle, lateral malleolus, and hallux; additional markers were placed on the radial and ulnar styloid processes of the dominant hand with one marker placed on the non-dominant radioulnar joint.26,28 Reflective tape was placed on a standard NCAA collegiate ball.
Each player was instructed warm-up based on their standard team regulated stretching and throwing preparation routine. The players received standardized instructions to pitch ten game-effort pitches from the wind-up position off an indoor mound (with a standard slope of one inch in height for every foot nearer to home plate); all pitches were 2-seam fastballs. Each player pitched into a marked area along a wall net that was the same size as home plate (43.18 cm X 43.18 cm). Data was collected from the three pitches with the greatest accuracy and velocity. Ball velocity was measured with a radar gun.
The pitching cycle (lead foot contact to ball release) was normalized to 100%.26,29 The variables calculated included: 1) three joint angles (maximum shoulder ER during the pitching cycle, shoulder abduction angle at foot contact, and elbow flexion angle at ball release); 2) one angular velocity (maximum shoulder horizontal adduction angular velocity); and 3) two variables (initiation of maximum trunk angular velocity and initiation of maximum elbow flexion). These variables were calculated as the percentage of the pitching cycle at which the event occurred. These variables were chosen based on their influence on elbow valgus loading during the cocking and acceleration phase.7,14,15,22,30
Statistical Analysis
All statistical analyses were performed with SPSS (version 22.0; IBM Corp., Chicago, IL, USA). Descriptive statistics (mean and standard deviation) were calculated for Hip ROM and kinematic variable measurements. (Table 2) Pearson’s product correlations were used to evaluate the association between lead and trail hip IR, ER, and total rotational ROM and the six kinematic variables. Correlations were deemed significant if p was less than 0.01.
Results
The correlations between Hip ROM and biomechanical variables are shown in Table 3.
Relationship between Trail Hip ROM and Biomechanical Variables
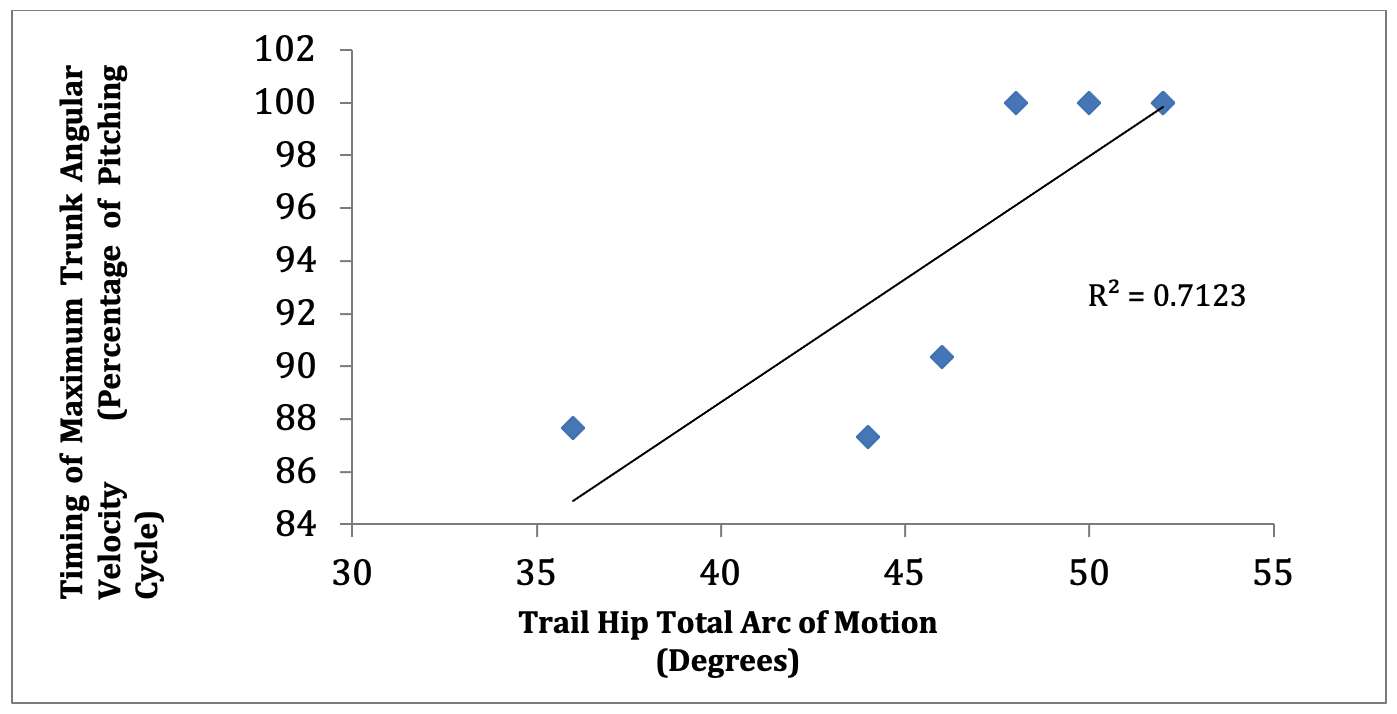
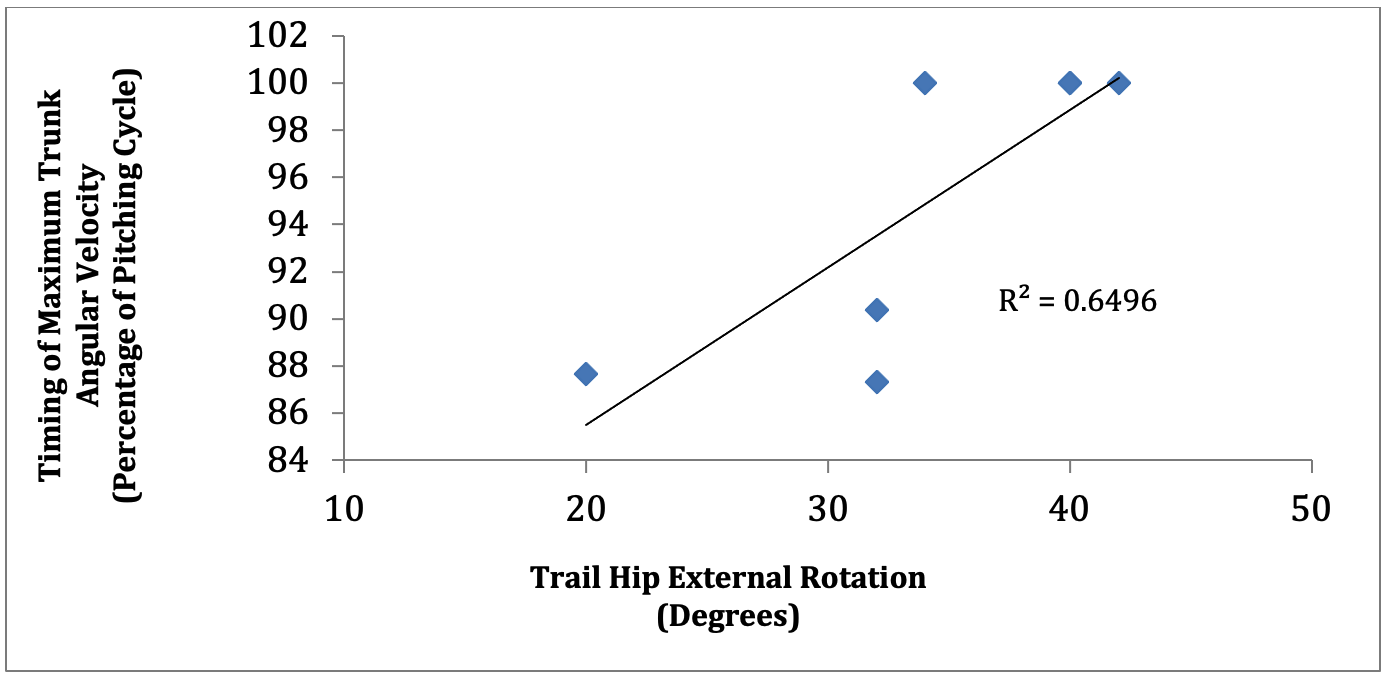
The trail hip TRARC was significantly related to the onset of trunk angular velocity (r = .712, p =.003). There was also a significant correlation between trail hip ER and the initiation of trunk angular velocity (r = .650, p=.009). (Figures 1A and 1B)


Relationship between Lead Hip ROM and Biomechanical Variables
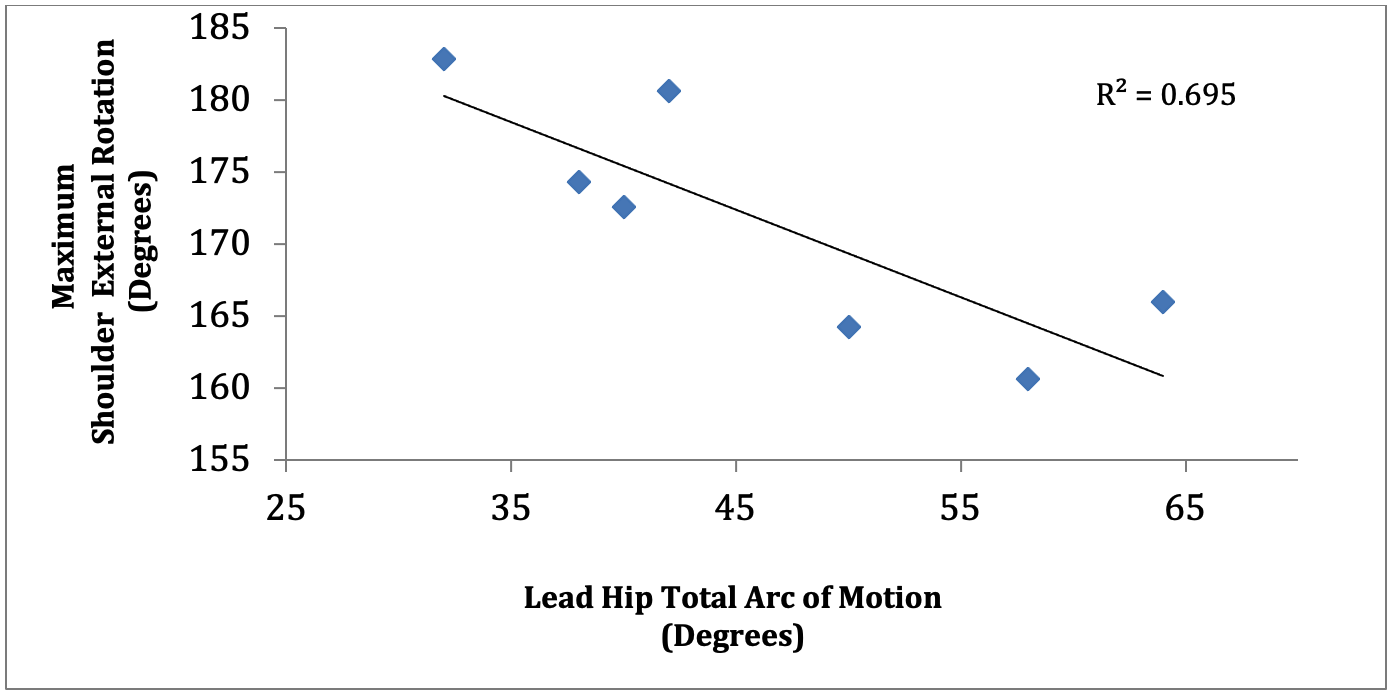
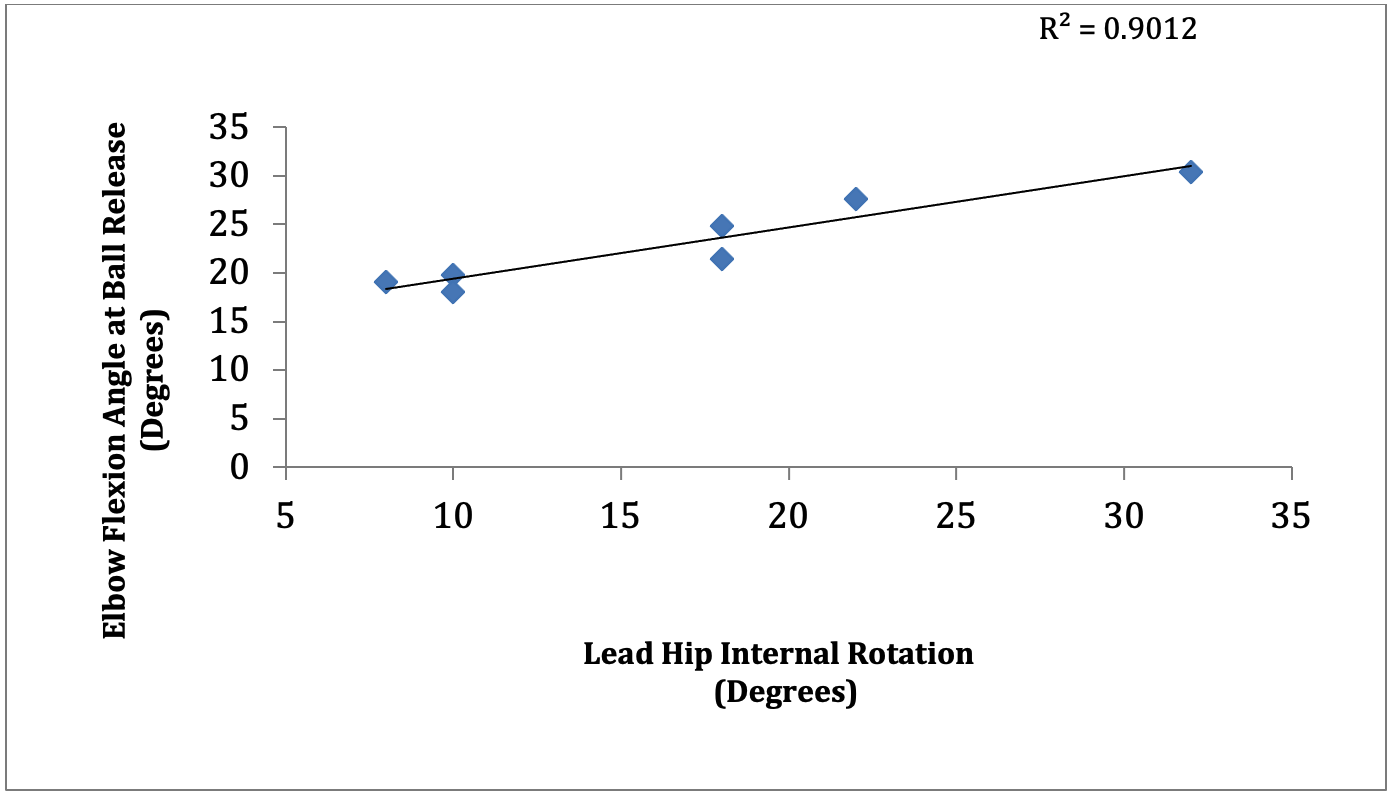
The lead hip total arc of motion was significantly related to maximum shoulder ER (r = 695, p = .005). (Figure 1C) There was a significant correlation between elbow flexion angle at ball release and lead hip IR (r = .952, p= .001). (Figure 1D)


Discussion
The influence of hip ROM is vital to developing obligatory trunk and upper extremity torque and ball velocity during the pitching motion.19–21,31,32 Most collegiate pitchers will either generate power through their stance leg in a load and drive strategy or by converting the force generated by their body moving towards their intended target into ball velocity by rotating around their stride leg.8,19,31,32 A decrease in hip ROM may initiate a series of compensatory actions within the pitching motion which may lead to increased elbow valgus torque and loading.2,7,10,14,16,19,22,32 The current findings suggest that there may be an association between hip ROM and established kinematic influencers of increased elbow valgus torque during the pitching motion.
Lee et al.33 described the hip as being the principle structure initiating the spine to rotate.33 From a kinematic perspective, the trail hip will initiate pelvic rotation which will be followed by trunk rotation which will influence lead foot contact position and overall pelvic orientation. If there is too much hip rotation, then the lead foot and pelvis will be in a more open position.21–23,34 Conversely, if there were too little hip rotation, the lead foot and pelvis would be in a more closed position.21–23,33 Fortenbaugh et al.,35 described that improper timing of pelvic rotation and trunk rotation would decrease pitching performance and increase stresses on the anterior shoulder and medial elbow.35 The authors reported that pelvic rotation should occur between 28% and 35% of the pitching cycle while trunk rotation should occur between 47% and 53% of the pitching cycle.35 The current findings demonstrated a correlation between trail hip total arc of motion and trunk angular velocity, which may provide further support showing that hip rotational ROM is correlated to pelvic orientation and trunk rotation and velocity. Additionally, decreased trail hip ER will restrict the forward movement of the pitcher’s trunk over the lead leg dampening the transfer of energy from the lower extremities leading to increased shoulder ER. However, the current findings did not demonstrate a correlation between lead hip rotational ROM and trunk angular velocity. We believe that our findings were due to our small sample size and although the results did not reach statistical significance, they did demonstrate that pitchers who rotated their trunks earlier in the pitching cycle appeared to have increased lead hip total arc of motion.
The current findings demonstrate that there is an association between lead hip total arc of rotational motion and maximal shoulder ER. This finding is consistent with previously reported findings showing that diminished as well as excessive lead hip rotational ROM can influence throwing shoulder ER during the late cocking and early acceleration phase.7,36 For example, inadequate lead hip ROM can cause a domino effect leading to decreased stride length and damped lower extremity force production.16,21 The pitcher will be forced to throw across his body to compensate for the lack of force production by increasing shoulder ER to generate ball velocity.19 As a result, the pitcher may rely on shoulder rotation as the primary force generator while pitching. This method of force generation relies on increasing shoulder ER to rapidly move into IR to generate ball velocity, which has be shown to increase shoulder ER and elbow valgus torque, which may not only have a detrimental effect on pitching performance, but may lead to medial elbow pathology.7,8,10,22 Increased lead hip ROM will lead to the opposite effect, where the pitching shoulder lags behind the early rotating trunk.22,23 In this scenario, the pitcher will also have to compensate for reduced ball velocity by increasing shoulder ER. In this instance however, due early pelvic rotation, the pitcher has to compensate by speeding up the pitching arm to compensate for the de-rotated trunk. Again, due to early trunk rotation, the shoulder rapidly rotating from ER to IR would generate ball velocity. In both instances, shoulder ER is increased which may lead to increased medial elbow tensile stresses.7,8,22
The current data also showed that lead hip IR correlated to elbow flexion angle at ball release. Aguinaldo et al.,7 demonstrated that a decrease in elbow flexion angle was linked to an increase in elbow valgus torque.7 The authors surmised that this occurred because increased elbow flexion would reduce the lever arm (throwing arm) around the trunk as the pitcher moves toward the intended target.7 The shorter lever arm would lead to decreased elbow valgus torques compared to a more extended elbow, which would act as a longer lever.7 A more extended elbow during the pitching motion may be indicative of a throwing shoulder that lags behind a rotating trunk.7 This shoulder lag can be linked to excessive lead hip IR. However, the findings of the current study demonstrated an average lead hip IR of 16.9 degrees, which is a smaller angle that previous research has shown to be ideal for pitchers.35,37 Such findings would suggest restricted lead hip IR in this cohort. Sekiguchi et al.,38 found that decreased lead hip IR was significantly associated with an increased risk for shoulder and elbow pathology in a 9-12 year pitching cohort.38 Although younger than the current cohort, the authors believe that a similar situation may occur in the studied population, where decreased lead hip IR would lead to early pelvic rotation speeding up ball delivery and therefore altering the timing of elbow flexion at foot contact and may increase valgus loading along the elbow.
The current findings did not demonstrate a correlation between lead and trail hip ROM and maximum shoulder horizontal adduction angular velocity and shoulder abduction angle at foot contact. Previous published research has demonstrated that pitchers with excessive horizontal adduction during late cocking in a situation where the pitcher leads with his elbow will increase medial elbow stress due increased varus elbow torque.35,39–41 In addition Matsuo et al.,42 showed that at late cocking pitchers with an angle less than 90-100 degrees of abduction during foot contact would demonstrate increased elbow varus torque.35,42 Both scenarios, a pitcher leading with his elbow and or with decreased shoulder abduction would increase deleterious stresses along their medial elbow and diminished ball velocity.
The results can be used to gain preliminary insight to the relationship between hip ROM and pitching kinematics related to elbow valgus loading. Although it may be difficult to address and measure pitching kinematics or kinetics within the clinic, a thorough understanding of hip anatomy, pathomechanics, and muscle physiology can assist with making informed decisions regarding the genesis of injury when evaluating the pitcher. While, the current study was not powered to determine injury risk, there seems to be a relationship between hip ROM as a clinically modifiable factor and pitching kinematics related to elbow valgus loading.43,44 These findings suggest hip ROM should be examined as part of the overhead athlete assessment during the evaluation process.
This study has several limitations when interpreting the results. The sample size is limited in number and consisted of seven Division 1 baseball pitchers, which may have been too small to accurately assess relationships. However, collegiate pitching populations are historically small and accessibility to this population and measurements within a lab can be quite difficult to ascertain. Additionally, the results cannot be extrapolated to other age (youth) or level (professionals). Furthermore, intra-rater reliability was not assessed when measuring hip ROM in the prone position in this study. However, reliability has been previously reported for the hip ROM measurements positioning and technique that we incorporated. The authors utilized the same two clinical examiners in the same role, one to stabilize and one measure for every athlete.24,25 Kinematic variables were acquired in a laboratory using an artificial mound, which is not identical to pitching on the field.
Conclusion
In conclusion, previous literature has described the relationship between specific kinematic and kinetic variables and medial elbow valgus loading.7,8,10,22,36,39,42 The findings of the current study elucidate the relationship between hip ROM and specific kinematic predictors of medial elbow valgus loading; i.e. initiation of trunk rotation, increased maximum ER, and increased elbow flexion angle at ball release. Understanding the relationship between hip ROM and pitching kinematics related to increased medial elbow valgus loading is instrumental for healthcare and performance providers to understand how alterations hip ROM may affect the pitching motion and consequentially predispose the pitcher to injury and decreased performance. Additionally, hip ROM should be screened by practitioners when determining prevention and rehabilitation programs for collegiate pitchers.
Disclosures
This study was approved by the University of Florida Health Science Center Institutional Review Board (IRB-01). The authors certify that they have no affiliations with or financial involvement in any organization or entity with a direct financial interest in the subject matter or materials discussed in the article.