INTRODUCTION
The lower extremities and trunk are critical components for power generation during throwing or hitting sports. When throwing a baseball, force is initiated by the legs, transferred to the trunk and then to the upper extremity for ball release. The proximal segments of the hip and trunk are estimated to contribute 50% of the kinetic energy and force during dynamic overhead arm activities.1,2 Any alterations in proximal segmental sequencing or force transfer can alter the kinetics and kinematics at the distal joints, leading to increased joint and soft tissue stress.2–4 Disruptions in the kinetic chain can increase forces at the shoulder and elbow, and these increased forces have been associated with arm injuries in baseball players.5–8
The hip abductor muscle group has a direct effect on motion at the hip via their proximal and distal attachment sites. They also have an indirect effect on motion at the trunk via the attachment of the gluteus maximus to the pelvis and lumbar spine, via the thoracolumbar fascia. During a dynamic single-leg landing task, individuals with hip abductor and extensor weakness had increased trunk lean towards the stance limb.9 Moreover, greater trunk lean occurred in participants with hip weakness despite increased activation of the trunk musculature. The hip abductor muscle group also has a direct influence on both lower extremities during throwing. On the trail leg (ipsilateral to the throwing arm) the abductors function to stabilize the pelvis and provide balance during the wind-up and early cocking phases.10–12 The lead leg (contralateral to the throwing arm) functions to decelerate the knee, provide a stable base, and absorb the force transferred from the deceleration and follow through phases.5 Hip abductors that exhibit high activity during pitching include the gluteus maximus and medius. The gluteus maximus is more active on the trail leg, while the gluteus medius is more active on the lead leg. Moreover, lead leg gluteus medius activity was inversely related to the rate of axial pelvis rotation during arm-cocking phase, as well as directly related to the rate of axial pelvis rotation at maximal external rotation, indicating a two-fold role of the gluteus medius, serving as a pelvic stabilizer and controlling the rate of axial pelvis rotation.13 Based on their action, weak hip abductors may cause compensatory dynamic knee valgus or pelvic drop leading to further movement compensations up the kinetic chain distally at the shoulder and elbow.
Single-leg dynamic tasks such as a squat, step-down, or stance are functional tests that can be used to assess trunk and lower extremity control.3,14–16 The lumbopelvic motion deficiencies seen during these single-leg dynamic tasks are related to altered pitching mechanics, performance, and incidence of arm injuries.3,4,14,16 The single-leg squat can detect lateral trunk lean deficits and predict the amount of trunk lean observed during pitching.16 The single-leg stance test has identified deficits in lumbopelvic control that are related to poor pitching performance and injury risk,14,16 and to increased shoulder horizontal torque and elbow varus torque during pitching.4 Movement deficits during single-leg dynamic tasks have implications for pitching, but it is unclear what factors contribute to these deficits. Moreover, movement deficits during dynamic tasks could theoretically also impact position player performance and injury risk; there is lack of evidence supporting this hypothesis.
The purpose of this study was to determine the relationship between hip abduction isometric strength and trunk lean, trunk flexion, knee valgus, pelvis drop, and hip flexion motions during a single-leg step down task (SLSD). It was hypothesized that hip abduction strength would be negatively correlated to the degree of motion deficits. Identifying the relationship of hip abduction strength to kinematics during a dynamic task will provide a foundation to understand why these motion deficits occur and enable the development of programs that minimize and prevent upper extremity injuries in baseball players.
METHODS
Participants
Data were collected for this prospective study as part of 2017 pre-season physical examinations on Minor League baseball players from a single organization. Participants were required to meet the following inclusion criteria: 1) free from injury at the time of testing, and 2) on a team roster in the participating organization for the full competitive season. The duration of time that the players were free from injury was not accounted for. Participants were excluded if any of the following criteria were met: 1) not cleared to participate in baseball activities, 2) currently receiving treatment for an injury, and 3) players not on a team roster with the participating organization for the full competitive season. Pre-season strength and conditioning program records were not available. Individualized strength and conditioning programs were performed during the season but the details were not available for analysis. This study was approved by the University of Southern California Institutional Review Board and all participants provided written informed consent.
Procedures
Pre-season assessments were performed at the organization’s Minor League training facility. A health questionnaire regarding current upper extremity injury status and upper extremity injury history for the past year was completed by all participants. Specific injury questions included body part injured, injury diagnosis, time lost due to the injury, and upper extremity surgical history. Each participant’s health history was reviewed by a member of the organization’s sports medicine staff to ensure accuracy. Demographic data such as age, height, weight, position, throwing arm, and years of Minor League Baseball participation were also collected. Participants next underwent testing for the SLSD and hip strength on both the lead and trail legs. The lead leg (stride leg) is defined as the leg contralateral to the throwing arm and the trail leg (stance leg) is ipsilateral to the throwing arm.
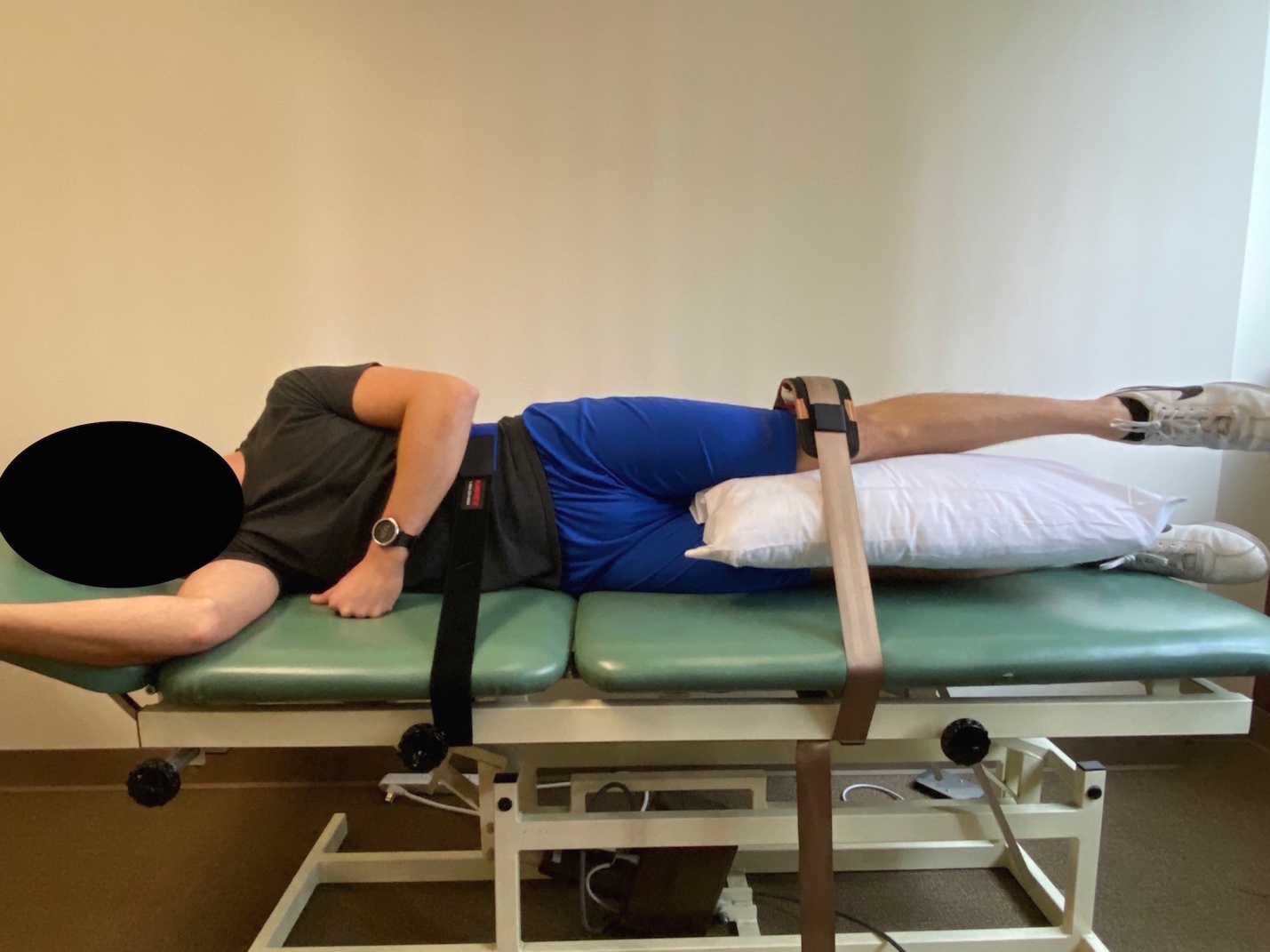
Hip abduction isometric strength was assessed with the participant in a side-lying position with the hip placed in approximately 20 degrees of abduction, legs fully extended in line with the trunk, and supported with a pillow between the knees (Figure 1). A strap placed just proximal to the iliac crest and secured to the table was used to stabilize the trunk. A hand-held dynamometer (HHD) (MicroFet 2, Hoggan Scientific, West Jordan, UT, USA) was placed 5 cm proximal to the lateral knee joint line and stabilized with a strap. Participants performed two maximal effort isometric contractions trials held for five seconds, with verbal encouragement given throughout each trial to help ensure maximal effort. Hip strength testing was performed as a “make” test, with participants meeting the resistance applied by the strap. Motion was visually monitored to ensure the participants did not attempt to compensate at the trunk or hip in the sagittal plane (flexion/ extension) or transverse (rotation). Leg length was recorded as the distance from the greater trochanter to the placement of the HHD. Hip abduction torque (Nm) was calculated by multiplying the HHD value by the leg length (m). Two trials were averaged for each leg, and used for data analysis. Test-retest reliability for hip abduction isometric strength was established in a prior pilot examination (n=7), and Interclass Correlation Coefficient (ICC 3,2) was 0.96, with a standard error of the measure (SEM) of 18.9 N and a minimal detectable change (MDC90) of 44.2 N.

The single-leg step-down (SLSD) task was performed twice on both the trail and lead legs. Reflective markers (n=9; 14.0 mm) were attached on the sternum, bilateral greater trochanter, bilateral anterior superior iliac spine (ASIS), bilateral fibular head, and bilateral lateral malleoli using double-sided tape. Participants stood on a single leg, on a 0.203 m (8 in) step, and lowered their contralateral heel to the ground over two seconds. Once the heel touched the ground, they returned to the starting position over two seconds, controlled with verbally counting ‘one-one thousand, two-one thousand’. Video cameras were mounted on tripods and placed 3.56 m from the box in the frontal and sagittal planes (Sony Handycam CX405 HDR, New York City, NY, USA).

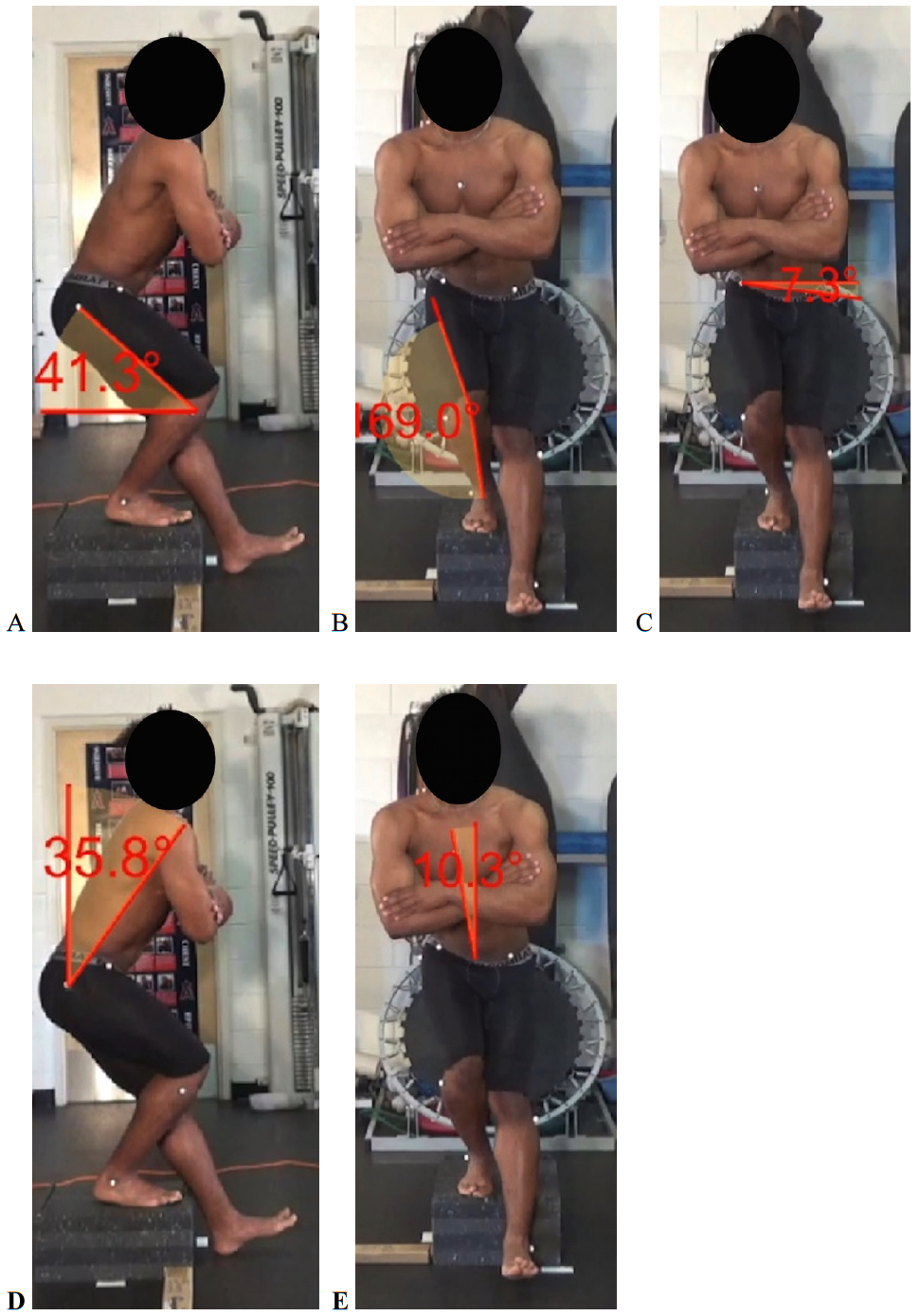
Dartfish software (Dartfish USA Inc., Alpharetta, GA, USA) was used to measure 2D hip flexion, knee valgus, trunk flexion, trunk lateral lean, and pelvic drop angles (Figure 2). Prior to analysis, the videos from the frontal and sagittal planes were synced, and the point of joint angle measurements were taken during the SLSD when the contralateral heel first touched the ground. Hip flexion in the sagittal view was defined as the angle between the horizontal global axis, and the line between the fibular head marker and the greater trochanter marker. Knee valgus angle in the frontal plane was defined as the frontal plane projection angle, by a line between the ASIS marker to the center of the patella, and a second line from the patella to the midpoint of the talocrural joint.17 A value of 180° indicated no knee valgus. Trunk flexion angle in the sagittal view was defined as the angle between the vertical global axis and the line between the greater trochanter marker that bisects the trunk segment. Trunk lateral lean angle was defined as the vertical global axis and a second line at the midpoint of the two ASIS markers extending to the sternal notch marker. Absolute trunk lean was assessed therefore the direction of lean was not considered, only the magnitude of lean either towards or away from the stance leg. Pelvic drop was measured in the frontal plane and was defined by the horizontal global axis beginning at the ASIS marker on the weight bearing leg and a second line extending to the ASIS marker on the non-weight bearing leg. Each variable was assessed for the two SLSD trials and the average was calculated for data analysis. Test-retest reliability for all SLSD joint angles was established prior to data analysis (n=10). The ICC 3,2 and standard error of the mean (SEM) for lower extremity kinematics during the SLSD were: hip flexion 0.9 (4.9°) with an MDC95 of 13.6° and knee valgus via the frontal plane projection angle 1.0 (1.3°) with an MDC95 of 3.6°. The ICC 3,2 and (SEM) for trunk flexion was 1.0 (1.04°) with an MDC95 of 2.9°. Trunk lateral lean angle had an ICC 3,2 and (SEM) of 1.0 (0.8°) with an MDC95 of 2.2°. The ICC 3,2 and (SEM) for pelvic drop was 1.0 (1.0°) with an MDC95 of 2.7°.
Statistical Analysis
Descriptive statistics were calculated for all demographic variables. Pearson product moment correlation coefficient analyses were performed to determine the relationship between hip abduction torque and motion variables of trunk lean, trunk flexion, hip flexion, knee valgus via the frontal plane projection angle, and pelvic drop during the SLSD. Separate analyses were performed for position players and pitchers for both the lead and trail legs. Statistical significance was set a priori at p < 0.05 and all analyses were performed using IBM SPSS Statistics Version 24.0 software (International Business Machines Corp., Armonk, NY, USA).
RESULTS
One-hundred and thirty Minor League baseball players participated, but 12 players did not complete all measures and were removed from the data set (Table 1), leaving 118 for data analysis. All measures and correlations between hip abduction torque and SLSD joint angles data are presented in Table 2. For position players (n=50), there were no significant correlations between hip abduction torque and SLSD variables. For pitchers (n=68) on the lead leg, decreased hip abduction torque was associated with increased knee valgus (r= 0.24, p=0.049). In the trail leg of pitchers, decreased hip abduction torque was associated with increased pelvic drop (r= -0.28, p=0.021).
DISCUSSION
Overall, the gluteal musculature needs to function as a whole in order stabilize the pelvis and control the femur during dynamic tasks. However, it is unclear what factors, specifically, contribute to observed movement deficits during single-leg dynamic tasks. Both the gluteus maximus and gluteus medius have been found to be important stabilizers of the pelvis in pitchers.13 The hip abductors, along with other musculature about the hip and pelvis, are associated with control of the pelvis and femur during the SLSD in pitchers. Specifically, hip abduction strength was found to be negatively correlated to frontal plane deviations of greater pelvic drop on the trail/stance leg and knee valgus on the lead/stride leg. In other words, there was greater knee valgus and pelvic drop with lower values of hip abduction strength, but only in pitchers. Although significant, the results demonstrate a weak relationship for which the clinical significance is unknown. This likely indicates that the abductors are only one contributor to the observed changes in knee valgus and pelvic drop. The strength of other muscles that contribute to lower extremity kinematics during the SLSD were not assessed. The movement deviations seen during the dynamic SLSD task related to hip abduction strength deficits may reveal compensations that affect pitching performance. If the deviations in pelvic drop and knee valgus are mirrored during throwing due to hip abductor weakness, there may be negative effects on the transmission of forces distally. This is only a postulate, as kinematics during pitching were not assessed in this study. The SLSD task detected deficits in dynamic control of the pelvis and lower limb. There may be potential value of the SLSD test to determine movement control and hip abduction strength deficiencies in baseball players, particularly in pitchers.
Knee valgus has been related to lower extremity injury risk during dynamic movement tasks.18–20 Specifically, female athletes with greater knee valgus during a jump landing task had a greater rate of a subsequent anterior cruciate ligament injury.18–20 Moreover, athletes sustaining a non-contact knee injury had increased knee valgus during a single-leg drop vertical jump compared to uninjured athletes.18 Hip abductor strength controls femoral abduction, a component of knee valgus,21,22 and hip abductor weakness can predict non-contact anterior cruciate ligament injuries.23 These studies suggest that knee valgus and hip abductor weakness are risk factors of knee injuries, but they have not been examined for their relationship to upper extremity injuries in baseball. The lower extremities and trunk are critical for the development of force during throwing and altered movement patterns can negatively affect force transfer in the kinetic chain.1,2,24–26 Knee valgus may lead to an unstable base of support that decreases force transmission to the shoulder and elbow and results in compensating that cause increased forces at these joints.25,27 Additional research may be helpful to correlate lead leg dynamic knee valgus and upper extremity injury to determine whether it is important to correct dynamic knee valgus in the throwing motion. The current study is the first to establish a relationship, albeit weak, between hip abduction strength and dynamic lower extremity valgus on the lead/stride leg in baseball pitchers, however, the clinical significance of these findings is unknown.
The hip abductor muscle group helps to control knee valgus via the femur and pelvis during dynamic lower extremity tasks.28 The gluteus medius and maximus abduct the femur, and weakness of these hip abductors can contribute to contralateral pelvic drop. This is of particular importance in baseball pitchers because the gluteals need to create an abduction moment on the trail limb to keep the pelvis level during single-leg support. Pitchers are in a position of single-leg support on the trail leg during the wind-up and early cocking phases. Abnormalities in pelvic motion can lead to kinetic chain alterations.29–31 A recent study reported relationships between deficits in lumbopelvic control during single-leg stance on the trail leg and increased shoulder horizontal and elbow valgus torques during pitching.4 Moreover, poor lumbopelvic control is related to a higher likelihood of missing more than 30 days due to an upper extremity injury and reducing pitching performance.3,14 Pitchers with better lumbopelvic control had fewer walks and hits per inning and more innings pitched during the season.3,14 The current study is one of the few to directly observe lumbopelvic motion in a functional dynamic task, and the first to relate these deficits in pelvic motion to hip abduction weakness. However, the clinical significance of these findings is unknown.
There was no relationship between hip abduction strength and deficits in knee valgus and pelvic drop in position players. This may in part because position players do not throw off the mound as pitchers do. Moreover, position players likely have more movement variability than pitchers, as their throwing patterns vary with throws from a variety of distances and positions. Perhaps the repetitive and consistent nature of pitching contributed to decreased movement coordination in the pitchers in responding to a novel task like the SLSD. Additional data collection including the number of sports played previously and number of years in each individual sport may provide insight into the effect of individual movement variability on lower extremity and trunk kinematics.
No deficits in trunk control during the SLSD were found. Trunk control is critical during throwing, as greater trunk lean is related to increased shoulder and elbow joint kinetics during pitching.32–34 Poor trunk control may contribute to injury at the shoulder and elbow. Trunk lean detected during a dynamic task such as a SLSD or similarly a single-leg squat can detect trunk lean deficits during pitching. Plummer et al16 found a correlation between trunk lean during the single-leg squat and the amount of trunk lean during pitching (r=0.53; p<0.001). However, the factors that contributed to trunk movement deficits in the single-leg squat and pitching were not clear. Interestingly in the current study, trunk lean was not related to hip abduction strength in pitchers or position players. This is surprising due to the observed relationship with pelvic drop. Theoretically if pitchers with decreased hip abduction strength had increased pelvic drop, one would expect a compensatory increase in trunk lean. It is important to establish the relationship between kinematics observed in a clinical test, and kinematics observed during pitching to identify pitchers that have underlying movement deficits without the need of advanced motion capture systems.
There are several limitations of this study to be considered when interpreting the results. A dynamic task that relates to throwing was measured, but throwing was not directly observed. While the SLSD is a dynamic and reliable clinical assessment, it may not load the hip abductors enough to demonstrate more widespread joint deficits seen in throwing. Strength is not the only reason for altered kinematics; motor control has a major role in the coordination of athletic tasks. The significant, but relatively low correlation values between movement deficits and hip abductor strength suggests other physical factors need to be assessed. This study is the first step in understanding the relationship between muscle capacity (strength) and movement deficits in pitchers. To fully understand the relationship of trunk or lower extremity motion deficits, future research should aim to compare the effects of weakness in multiple lower extremity muscles and the trunk during throwing. Another limitation is that a subgroup analysis was not performed for position players due to low sample sizes for certain positions. Future research should also aim to examine the ability of the SLSD and other clinical screening tests, such as a lateral step down or single-leg balance test, to identify deficits that may increase risk of injury for position players and pitchers.
CONCLUSIONS
The SLSD can be used as a screening tool to allow clinicians to identify movement deficits related to hip abduction weakness. The results of the current study indicate that pitchers with decreased hip abduction strength had increased knee valgus and pelvic drop during performance of a SLSD. Increased knee valgus and pelvic drop may be related to poor lumbopelvic control. Previous studies have reported that professional pitchers with poor lumbopelvic control have decreased performance and greater time lost from participation.3,14 Identifying pitchers with deficits in lumbopelvic control through the use of screening tests that do not require the use of three-dimensional motion analysis is valuable for clinicians who work with baseball players. The SLSD can be used to identify movement deficits and allow for the use of preventative training programs that target these deficits. If movement deficits can be addressed, then pitchers may improve pitching performance and have a decreased risk of injury.
Conflicts of Interest
The authors affirm that they have no financial affiliation that has direct financial interest in any matter included in this manuscript, except as cited in the manuscript. The authors affirm they have no other conflicts of interest.
Funding
This research was funded by The Major League Baseball research grant: risk factors associated with upper extremity injuries in baseball.