


INTRODUCTION
Dancers often suffer from decreased ability to perform relevé, plié, and jumping due to deficits at the ankle joint.1,2 Calf pain from overuse, prevalent among professional ballet dancers, creates these limitations, which prevents the dancer from performing at their full potential.3–5 Research suggests dry needling (DN) may be effective for immediately decreasing musculoskeletal pain,6–17 but the acute results of DN on range of motion (ROM) have been mixed.7,8,10,12,14,16,18,19 Currently, evidence regarding the immediate results of DN on gastrocnemius and soleus function is limited.14 Additionally, only a small number of studies have demonstrated the instant effects of DN on force production.7,20–22 There are no studies on DN and surface temperature of the specific muscle treated.
Myofascial pain occurs in patients with MTrPs, defined as a point within a taut skeletal muscle exhibiting an increased response to a stimulus.23 One hypothesis for the cause of MTrPs is that acetylcholine (ACh) is released excessively at the neuromuscular junction, creating an area of tautness within the muscle.23 This may cause unremitting stimulation of the sarcomere and may lead to hypoxia.23–25 DN involves the insertion of a thin, filiform needle into MTrPs that elicit a local twitch response affecting the ACh at the neuromuscular junction.23 DN is also thought to impact blood flow by causing the release of vasoactive substances, which promote vasodilation and increase oxygenation similar to deep tissue massage.23,26,27
Even though researchers have documented increases in blood flow and oxygen saturation to the tissue after DN, the question remains if DN affects the surface temperature at the tissue being treated.23,26,28,29 One study demonstrated an increased temperature reading at an acupuncture point after the needle was in this point for 10 minutes.30 Recent research has shown that DN provokes intense vasodilation and temperature increases in measured referral points to the muscle treated.31 However, there are no studies that assess the pre- and post-surface temperature of the specific muscle being treated with DN.
Meta-analyses conducted on pain scores indicate that there is a statistically significant improvement in pain ratings immediately after DN.9,32 DN has also been shown to reduce pain faster than analgesics following total knee arthroplasty.15 Instant improvement on pain pressure threshold in the masseter muscle compared to placebo, decreased pain sensitivity in 57 shoulder patients, and a decrease in cervical muscular pain have been demonstrated after DN.6,8,12,13 Patients with myofascial pain syndrome demonstrated improvements on the Visual Analog Scale (VAS) after DN vs. sham needles immediately and at four weeks post treatment.17
Other authors have explored the effects of DN on pain in athletes such as rugby and volleyball.10,14,16,18 Mason, Tansey and Westrick reported decreased knee pain after DN in a case report on a dancer with posterior knee pain.14 These results on athletes might indicate DN as an effective means to treat ballet dancers’ calf pain immediately, but DN’s impact on performance ability remains unclear.
Amongst dancers, the effect of DN on ROM is especially important. Since one-fourth of injuries in ballet dancers involve the ankle joint, improving dorsiflexion ROM is key to prevention and treatment of acute and overuse injuries.4 Adequate triceps surae flexibility has demonstrated increased dorsiflexion ROM, increased force production by improving the ability to generate elastic energy, and decreased excessive pronation upon weight acceptance.4,33 In addition, increased dorsiflexion when landing jumps has been suggested to increase ankle plantar flexor pre-stretch, which may improve the utilization of elastic energy and enhance jump function.34 Therefore, improving dorsiflexion ROM of the triceps surae may be important in injury prevention and dancer performance.
Fernandez-De-Las-Penas describes trigger points as taut bands which limit joint mobility.35 Grieve et al36,37 performed studies on manual trigger point release to the triceps surae musculature and reported positive results in regards to ROM after intervention. Eftekharsadat, Babaei-Ghazani, and Zeinolabedinzadeh38 performed DN in patients with heel pain and demonstrated no effect in ankle ROM. However, the methodology of this study was different because it pre-determined points in the calf, did not manipulate the needle, and the measurements were taken at 4 weeks post-intervention.38 Additional authors have found immediate increases in shoulder ROM,16,39 cervical ROM,7,12,18,40 and jaw opening8 after DN.
Due to the possibility of increased ROM, DN may impact force and torque production immediately after treatment. Behm and Chaouachi1 have shown that increased ROM is associated with decreased force production acutely.1 Prolonged static stretching, which also increases ROM, has been shown to decrease voluntary peak torque and electromyographic amplitude when subjects perform isometric maximal voluntary contractions.41 Static stretching causes decreased strength production by affecting the length-tension relationship of the muscle secondary to changes in compliance.1 If DN could have the same lengthening effects as stretching, it may also have a similar potentially detrimental effect on torque production.
However, Ge21 found that latent trigger points decrease force production, so it is vital to research the effect DN would have on force production. Dar and Hicks found20 that DN in multifidus increases muscle function immediately. Cerezo-Telléz et al demonstrated an immediate cervical muscle strength in all directions of flexion, extension, rotation, and side bending after cervical DN.7 DN has improved muscle endurance of the knee extensors immediately and at four weeks in soccer players.22
DN might not result in improved outcomes immediately. Huguenin et al10 found that pain improved with DN, but passive straight leg raise and hip internal rotation remained unchanged in both therapeutic dry needling and placebo groups. However, Huguenin et al10 also concluded that they did not chose the appropriate ROM assessment. One RCT of DN demonstrated no improvement in hamstring ROM or knee pain immediately when compared to sham DN.42 One meta-analysis states that DN is less effective in treating pain conditions, but may be better at increasing ROM.19 DN has been demonstrated as less effective than acupuncture for motion-related chronic neck pain.43
The purpose of this study was to assess the immediate effects of DN on myofascial trigger points in terms of skin surface temperature, pain, active and passive range of motion, and plantar flexion torque production in the triceps surae of ballet dancers. Based on the literature review, it was hypothesized that DN would have a significantly greater effect than sham DN on decreasing pain, increasing skin temperature, increasing ankle ROM, in addition to a decreasing in plantar flexion torque immediately following treatment.
METHODS
Subjects
Eleven healthy, full time (25 hours of dance per week) ballet dancers were recruited from a professional ballet company by word of mouth. These dancers were included in the study if they presented with MTrPs in the calf through palpation. Dancers were excluded if they had significant health problems or bleeding disorders, were pregnant, feared needles, or had taken anticoagulant or pain relieving medications within the past 24 hours. Participation in this study was also denied if an individual had undergone DN or acupuncture in the prior four weeks. Prior to testing, the participants read and signed a specific Northwestern University and Andrews University IRB approved consent form. This included a health history form asking about recent injuries and general medical health.
Subjects were randomly assigned into two groups through computerized random number generation by the physical therapist performing the intervention so the assessors were blinded. The experimental group received bilateral DN to the calf, plus passive calf stretching of two repetitions of thirty seconds on a slant board in both knees bent and straight positioning, while the control group received bilateral sham DN (SHAM) in addition to the same slant board calf stretching protocol. All subjects had the intervention performed in a lab room at Northwestern University’s Physical Therapy department. A physical therapist provided the intervention, while physical therapy students, blinded to group assignment, obtained pre/post measurements after they had practiced and demonstrated competency in their measurement areas.
Materials
DN was performed using Seirin J-Type 30x30 needles. The 10cm VAS (Visual Analog Scale) was used to assess overall calf pain pre- and post- intervention as reported by participant, and temperature was measured with The Exergen TAT-2000 Series Professional Model Temporal Scanner (Exergen Corporation, Watertown, MA). A goniometer was used to measure the ankle dorsiflexion PROM in CKC (closed kinetic chain) and AROM in OKC (open kinetic chain). An isokinetic dynamometer, the Biodex System 3 Pro (Biodex Medical Systems, Shirley, New York), was used to measure calf force.
Procedure
Individuals meeting inclusion criteria were randomly blinded and placed into either the experimental or control group. The subjects were barefoot and wore athletic clothing. Each dancer followed a five-minute, standardized dance-specific warm up video prior to testing.
Initially, baseline skin temperature was measured at three standard points (SP) with a surface thermometer placed on marked spots 10cm below the popliteal fold, 10cm above the calcaneal tuberosity, and at a point in between. A blinded assessor performed and averaged the three measurements to discern an overall calf temperature pre-intervention. Then, a physical therapist certified in DN and having >10-years’ experience palpating dancers’ calf musculature located five trigger point (TP) spots using palpation. The trigger points were circled with a marker (Figure 1)
.jpeg)
After trigger point palpation, another blinded assessor administered a 10cm Visual Analog Scale (VAS) for the overall pain score of the five TP pre-intervention. The same blinded assessor measured all of the subjective calf pain for both the DN and SHAM groups pre- and post-intervention. The blinded assessor used the same script for each subject. The VAS has established test-retest reliability and sensitivity, and change in pain intensity can be easily obtained.44 A 50% pain reduction measured by the VAS was determined as statistically significant.44 As demonstrated in previous research, participants had access to their pre-test VAS at the time of the post-test VAS to reduce error.44
Next, the original temperature assessor measured surface temperature one more time to the nearest degree (Fahrenheit) at the marked TP and SP locations. The five TP measurements were averaged and the three SP measurements were averaged. This set of surface temperature measures was performed post-palpation, but pre-intervention, to confirm that the physical therapist’s palpation did not affect surface temperature. This second round of SP surface temperature measurements was conducted to confirm that the calf palpation did not change baseline temperature.
Ankle dorsiflexion AROM was measured bilaterally by a single blinded assessor using a standard 6-inch goniometer with the subjects in an open-kinetic chain seated position and for PROM in the closed-kinetic chain (CKC) weight-bearing lunge position. In OKC, the subjects sat over the edge of a plinth with their knees bent approximately 45-60° in order to prevent passive insufficiency of the gastrocnemius.45 The subtalar joint was placed in neutral position with the transcondylar axis of the knee in the frontal plane.46 Ankle dorsiflexion active range of motion (AROM) was measured in open chain first, using the standard text version.47 The neutral position was 0° and ankle motion was recorded to the nearest degree from that position in the dorsal direction.45 Subjects were asked to perform maximal active ankle dorsiflexion bilaterally three times and the angle was measured to the nearest degree. All measurements were recorded and the mean of the three was used for analysis.46 Only AROM was measured in this position because it is more functional and applicable to ballet while passive ROM could be influenced by human error due to the inconsistency with overpressure.
Dickson et al48 found that functional ankle dorsiflexion in modern dancers is best quantified in the weight-bearing lunge position, which has also been previously assessed for intra-rater (ICC=0.97-0.98) and inter-rater (ICC= 0.97-0.99) reliability.2 Subjects were asked to stand facing a wall in a lunge position with one knee touching the wall and the foot on the same lower extremity sliding backward to the point of maximum tolerance while the knee remains in contact with the wall and the heel with the floor. Researchers verified that each subject’s knee and heel remained in contact with the appropriate surface, and that the knee was aligned over the second toe prior to taking any measurements.48 The same bony landmarks were used to align the goniometer as in OKC ankle dorsiflexion AROM. Measurements were recorded three times bilaterally and the mean of the three was used for analysis. (Figure 2)
.jpeg)
Maximum muscular torque of the triceps surae was measured bilaterally using a Biodex prior to and after the DN or SHAM intervention. Two assessors blinded to group assignment performed all of these measurements. The participants were barefoot, seated and secured using a double chest strap, quadriceps strap, and two additional support straps fastened over the dorsum of the foot. The hip was placed at 90° flexion, the knee at 30° flexion, and the ankle at an angle of comfort for the participant. The axis of rotation of the Biodex ankle attachment was aligned with the lateral malleolus of the ankle being tested. Prior to testing, the participants warmed up by submaximally plantar- and dorsi-flexing each ankle ten times on the Biodex with no resistance. The subject then performed four maximal concentric contractions plantar flexion at angular velocities of 60°, 90°, and 120°/sec with a two-minute rest period between tests to minimize fatigue. The order of velocities was randomized. The first measurement was eliminated, and the remaining three were averaged for analysis using standard Biodex software in Newton.meters (NM).32,46,49 (Figure 3).

After all the pre-tests, the DN was administered to participants in the experimental group, while the control group received SHAM dry needling while lying prone on a plinth. The assessors were not present during the DN or sham DN. The DN was performed in the five previously palpated and circled trigger point locations on each calf using a clean technique with sterile needles. Needles were inserted into the triceps surae and repeatedly moved up and down in order to elicit a twitch response. All DN participants had twitch responses during the DN intervention.
The sham needles were prepared following the method adopted by Cotchett et al,50 which was originally found to be valid by Tough and colleagues.51 Prior to treatment, the needle tips were removed with wire cutters.52 The end of the needle was filed down to create a blunt surface that when tapped would not pierce the skin.50 The sham needle was placed back into its tube and repackaged. To begin each treatment, the skin was disinfected and a prepared sham needle was removed from packaging to stimulate a removal of a real needle.52 The sham needle was manipulated using the same technique as real dry needling. First, the applicator was placed on the skin and the dry needling administrator tapped the needle without piercing the skin. The applicator was removed while the administrator held the sham needle in place on the skin’s surface and mimicked needle rotation for five seconds, then removed the needle. The sham needle was disposed of in a sharps container to simulate the noise and effects associated with sharps disposal.50
Following the intervention, both groups were instructed to stretch on a 20° incline slant-board with straight and bent knees twice for 30 seconds. The choice to stretch after DN or SHAM as part of an intervention was to mimic the common tendency of ballet dancers to stretch after clinical treatment. Immediately following stretching, pain, temperature, ROM and torque were re-measured on both sides.

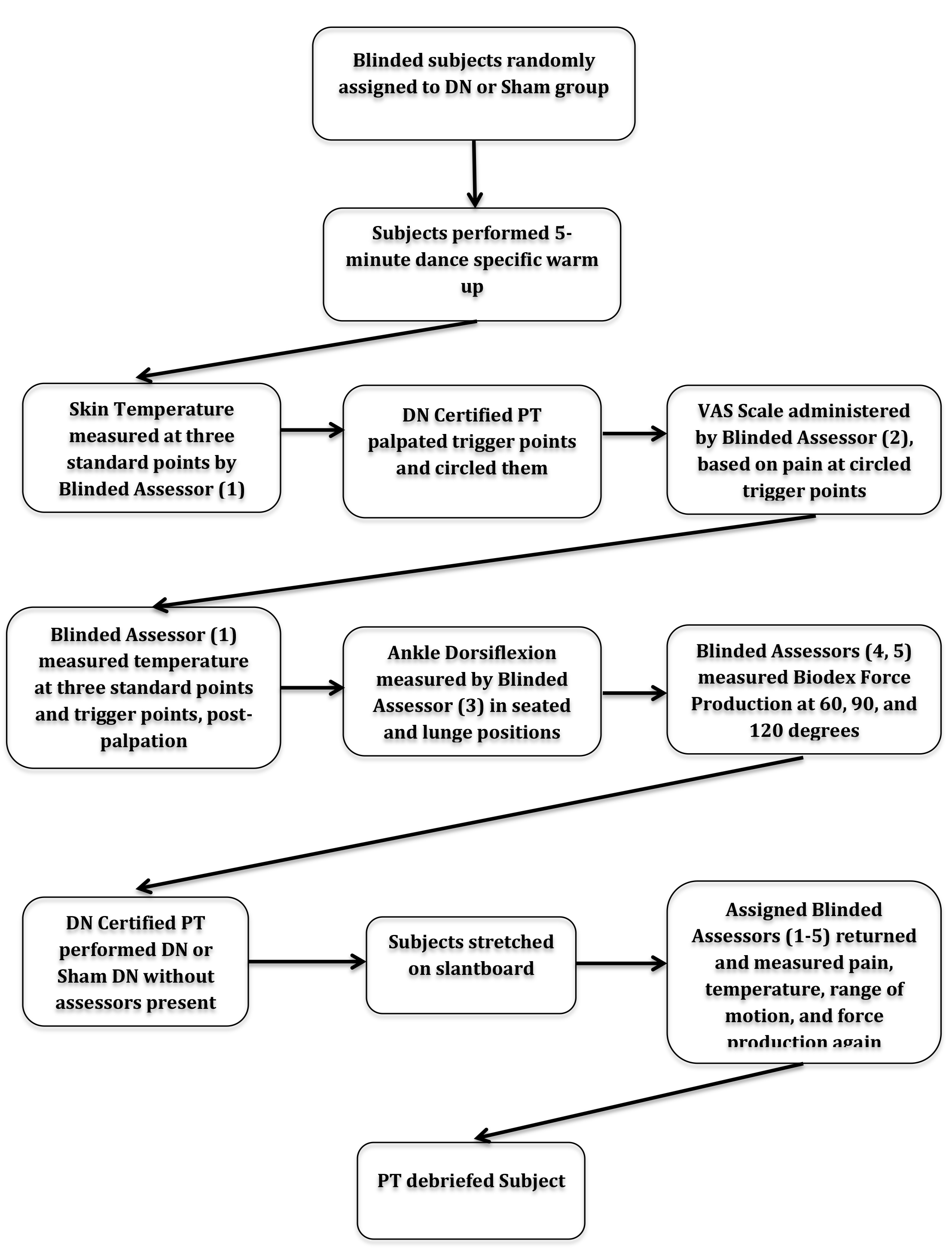
At the end of the procedures, the participants were debriefed on their treatment and given a contact number to call if they had any further questions or report adverse effects. No adverse effects were reported. Participants in the control group were given the opportunity to receive dry needling once they had completed the experiment but all declined. A summary of the methodology can be found in Figure 4.
Data Analysis
The raw data collected was used to calculate the independent and dependent variables. SPSS Version 10.0 (SPSS Inc, Chicago, IL) was used to analyze this data. A paired t-test was performed to compare pre- and post-intervention, as well as independent t-test to compare between the two test groups using a 95% confidence interval. Additionally, non-parametric statistics were run and the outcomes where statistically significant differences were found were the same between nonparametric and parametric analyses. Because of the specific homogenous population, parametric statistics were chosen. A histogram analysis looking for equally distributed variables was also performed. Statistical differences were assessed using the value p<0.05.
RESULTS
Six male and five female professional ballet dancers from the same professional ballet company fit the inclusion/exclusion criteria. The average number of years dancing professionally was 9.6. Six out of eleven of the dancers had used DN prior to the study. This was a uniform sample, as the subjects were similar in age and from the same professional ballet company. Males and females were similarly represented in both groups. (Table 1)
The mean measurements of pain, temperature, ROM and torque were calculated for all subjects prior to intervention. There were no significant differences for any mean measurement comparing right and left calves in temperature, pain, ROM, or force prior to the intervention. (Table 2)
Temperature
Prior to intervention, the mean surface temperature of the TP measurements was higher than the SP measurements when performing an independent t-test. This statistical significance happened in both the right and left calves (right: p= .014; left: p= .031). (Table 3) Using a paired t-test, the mean temperature for both the right and left calves in the SHAM group (right: p= .008; left: p= .008) and only the right calf in the DN group (right: p= .048) showed significance in temperature decrease from pre- to post- intervention. (Table 4)
VAS
There were no significant differences in mean VAS reported pain scores for either the SHAM or DN groups pre- to post-intervention. (Table 5)
ROM
In the seated AROM dorsiflexion measurement, the SHAM group had a statistically significant larger change in mean values in only the left calf (left: p= .005) when compared to the DN group. However, when a paired t-test compared the pre- and post- intervention measurements of the seated AROM dorsiflexion measurement in the SHAM group on the left calf, there was no statistical significance. (Table 6)
There was no significant difference in the lunge CKC measurement of dorsiflexion between the DN to the SHAM group. (Table 7)
Biodex Torque
There was a statistically significant (p= .027) increase in the torque of the plantar flexors at the 60-degree angular velocity (Table 8) in the DN group left side only when pre- and post- intervention was compared with a paired t-test. In the 90 and 120-degree angular velocity (Table 9 and 10), there was a statistically significant difference at 90 degrees (p= .014) and 120 degrees (p= .001) noted for mean change in torque, when comparing DN and SHAM on the right side only. The SHAM group had a larger mean change than the DN group. This change in the SHAM group was an increase in torque, but it was not statistically significant when comparing pre/post intervention measurements for the 90 and 120-degree angular velocity using a paired t-test.
DISCUSSION
Baseline measurements of surface temperature, pain, ROM, and torque demonstrated no significant difference between the right and left sides prior to intervention. (Table 2) This is interesting because dancers often have a lateral preference when performing, but this was not seen in the current measurements.11 This is relevant to future studies in dry needling because it demonstrates that perhaps only one side is needed for measurements and intervention.
Surface temperature measurements pre-intervention showed significantly lower SP mean temperature as compared to the TP mean temperature for the right and left sides (p=.014 right, p= .013 left). After intervention, both the right and left calves in the SHAM group, and right calf in the DN group showed a significant difference in mean temperature. The only other study that measured surface temperature with trigger points and dry needling was Skorupska et al,31 and they noticed an increase in surface temperature in muscles distal to the muscle being treated along the same nerve distribution after DN. A larger sample size would continue to investigate temperature responses after dry needling, since current research remains inconclusive in the direction of temperature change.30,31 The surface temperature findings are important in that it invites new research because demonstrates a potential nature of trigger point changes that may occur to MTrPs after DN. The baseline surface temperature is also important knowledge for the researchers that are trying to further understand trigger point physiology.
There were no significant findings for changes in pain which differs from the results of other investigations who demonstrated decreased pain after DN.6–17 Perhaps, specific population interprets pain differently, despite having used the uniform script to describe pain. Tajet-Foxell and Rose53 found that dancers had a higher pain threshold in regards to duration of pain but not intensity on a cold pain tolerance test. Due to this, dancers might tolerate the palpation of the trigger points but might rank the post DN palpation of the tender points as higher on a VAS, delineating the results differently than a typical population. Additionally, the examiner asked the subjects to average the pain between all five trigger points. A suggestion for future research would be to have the subjects rank each spot individually for pain, and then calculate a mean measurement. Lastly, immediate post-needling muscle soreness may have contributed to VAS outcomes, as Ziaeifar et al54 suggested that their subjects had improved pain intensity after two days instead of immediately after DN of the upper trapezius muscle.
The results of current research varies with trends in increases or decreases in ROM after immediate DN.7,8,10,12,14,16,18 For seated AROM, the SHAM group had a statistically larger change in AROM pre/post intervention on the left side (p= .005) as compared to the DN group. The lunge PROM measurements had no statistical difference between the DN and SHAM groups. Since this measure was performed in self-controlled lunging, some of dancers in the DN group might have been sore from the intervention and therefore self-limited their passive motion. Further research with a larger sample size needs to be performed as this study was underpowered, because our power analysis for ROM measurements required a sample size of 48 subjects.
In the 60-degree angular velocity Biodex force, the DN group on the left side only showed a statistically significant increase in torque production. In both the 90 and 120-degree angular velocity tests, the SHAM group had a statistically significant change as compared to the DN group on the right side only, but this was not significant when comparing pre/post intervention measures. To date, there are no known studies that compare DN using measurements of plantar flexion torque immediately after intervention. Since these findings are limited by the size of the study, caution should be used when performing DN prior to dance performance. Further research into the immediate effects on plantar flexion torque should be conducted.
There are several limiting factors in this study. As previously mentioned, this study was underpowered, which may have resulted in Type II errors. In part, this was due to coordinating multiple assessors in addition to the research process requiring 90 minutes per subject. Additionally, some subjects had previous experience with DN and were familiar with the twitch response. This potentially allowed them the ability to guess which treatment group they were assigned to, therefore limiting the subject-related blinding. Two subjects requested to not be dry needled due to concerns of being sore for dance rehearsal, so the SHAM group had two non-blinded subjects, further impacting the validity of the blinded subjects’ results.
This pilot study builds the framework for future DN studies, but further research is needed to determine the appropriate instruments to measure the effects of DN in the dance population. The unique methodology used in this study is important to consider when exploring further DN research. The assessors were blinded, reducing rater bias. All assessors were trained physical therapy students, and the same assessor took all measurements. Additionally, this pilot studied used a sham intervention to further blind the subjects.
CONCLUSION
The results of this research were inconclusive for changes in surface temperature, pain, ROM, and torque immediately after dry needling to the triceps surae musculature. However, this is the first blinded and randomized controlled study assessing the acute effects of DN in professional ballet dancers with a novel methodology for conducting further research. This study also presents potential information on the surface temperature of trigger points as compared to baseline temperature measurements. Further research is needed with larger sample sizes in order to fully understand the immediate effects of dry needling in the dance population prior to performance.
Statement of Institutional Board
Northwestern University, Chicago, IL STU00096692
Conflicts of Interest
The authors report no conflicts of interest.