Introduction
Nearly 30 million women play soccer worldwide1 while approximately 27,000 women play collegiate soccer in the United States.2 Collegiate female soccer players incur anterior cruciate ligament (ACL) injuries at more than double the rate of men.3–5 Of these injuries, most occur via a non-contact mechanism.3 Landing with the knee extended and in dynamic valgus during an abrupt or unexpected pivoting or cutting maneuver have been cited as frequent components of non-contact ACL injuries.6–9 Poor neuromuscular control, including dynamic knee valgus, is also believed to be a modifiable risk factor contributing to the increased incidence of non-contact ACL injuries in female soccer players.10
A variety of neuromuscular training programs have been designed to address strength and neuromuscular control deficiencies and reduce injury risk in female athletes.11–13 Common components of effective neuromuscular training programs include high intensity plyometrics, strength training, and an emphasis on exercise technique.12,14 A systematic review of the efficacy of neuromuscular training programs on the rate of ACL injuries by Sugimoto et al. reported a 73.4% relative risk reduction for non-contact ACL injuries in female athletes participating in neuromuscular training programs.13 The 11+ (previously known as the FIFA11+) is a program designed to be a comprehensive, time effective, warm-up program for soccer players that addresses key components of neuromuscular training including lower extremity strengthening and dynamic balance exercises.15 Furthermore, the 11+ emphasizes soft landings with plyometrics and maintaining proper lower extremity alignment throughout the program, but can be implemented by coaches with minimal training.15 The 11+ has also been established as an effective program for reducing ACL injuries in soccer players.16,17 An initial randomized control trial of the 11+ demonstrated a reduction of severe lower-extremity injury by 50% in female athletes, and additional studies have demonstrated a decrease in ACL injuries among male soccer players.16,17 Although the 11+ is effective in reducing non-contact ACL injury rates, the mechanism by which participation in the program reduces injury, and whether participation alters a player’s movement patterns on the field, is unclear.
Previous studies have sought to examine biomechanical changes following participation in the 11+ using a vertical drop jump. Collegiate female soccer players performing the 11+ for two consecutive seasons demonstrated greater knee flexion angle with drop jump landings compared to players completing a standard warm-up. However, players demonstrated no changes in kinematics related to lower extremity valgus.18 Pre-adolescent soccer players performing the 11+ for a single season demonstrated significant decreases in knee abduction moment during a double legged landing task when compared to control subjects completing a standard warm-up.19 Although bilateral tasks like the drop jump have been used in several studies as a biomechanical screening tool, it has also been suggested that a more sport-specific or challenging task may be needed to screen for ACL injury risk.20
Cutting is a movement pattern that soccer players frequently execute, and is the second most common mechanism of non-contact ACL injury among female soccer players.21 An epidemiological study of players in the German women’s national league reported that 22% of traumatic, noncontact injuries were the result of cutting. Furthermore, 7 of 11 total ACL injuries recorded in this epidemiological study were the result of a change in direction.22 Female soccer players who underwent ACL reconstruction (ACLR) have been shown to have significantly higher knee abduction angles and knee abduction moments than uninjured players while completing an anticipated cut to 45°.23 Although no normative values have been established for what constitutes a high knee abduction load during a cutting maneuver, it has been established that increased knee valgus may indicate increased risk for ACL injury and decreased neuromuscular control.24 It has also been determined that sharper cutting angles (>45°) result in greater knee abduction angles and moments than more shallow cutting angles.25 Therefore, the purpose of this study was to determine whether participation in the 11+ led to changes in hip and knee biomechanics during a soccer-specific 90° cut. Specifically, the aims were to determine whether participation led to changes in peak knee abduction moment, and the components of valgus collapse: hip adduction angle, hip internal rotation angle, and knee abduction angle. The authors’ hypotheses were that collegiate female soccer players participating in the 11+ for one season would demonstrate a greater decrease than control team players in peak hip adduction angles, hip internal rotation angles, knee abduction angles, knee abduction moments, and knee valgus collapse.
Materials and Methods
Procedures
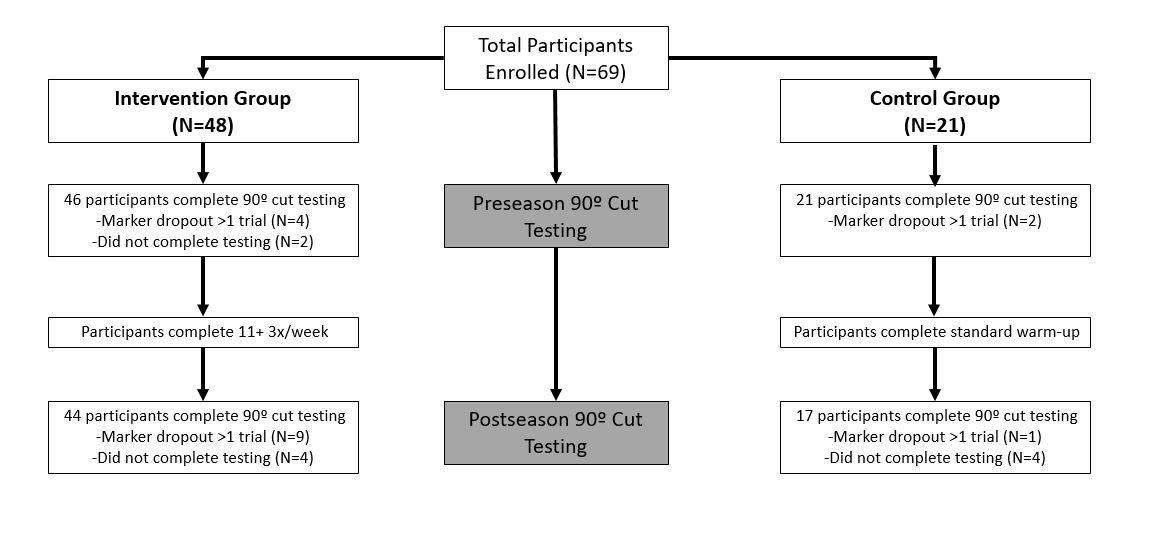
Sixty-nine athletes from three National Collegiate Athletic Association (NCAA) Division 1 and Division 2 women’s soccer teams participated in this study (Table 1). Teams were recruited based on proximity to the testing site and willingness to participate in motion analysis testing and the 11+ intervention. All participants signed informed consent documents prior to participation, and all study procedures were approved by the University of Delaware Institutional Review Board. Players were included, regardless of injury history, if they could complete a unilateral cutting task. Two teams completed the 11+ as a warm-up before team practices and games and served as the intervention cohort (Figure 1). Execution of the 11+ was supervised by the teams’ coach and athletic trainers. The coach from each intervention team completed a digital contract at the beginning of the season to acknowledge compliance to completing the 11+ throughout the 12 week season. Further description of the 11+ can be found on the FIFA Medical Network website.26 Compliance was also verified by a study investigator at the conclusion of the season. Intervention teams completed the 11+ at least three times a week for the duration of preseason and throughout the NCAA soccer season. The third team agreed to participate in preseason and postseason motion analysis testing, but was not willing to implement the 11+. Therefore, the third team served as a control team and continued to complete their standard warm-up before practices and games. The control team’s warm-up consisted of running, dynamic stretching, and passing the ball. Each team’s respective athletic trainer kept a log of all injuries sustained by players throughout the season, which was then sent to the study investigators.

Players completed pre and postseason motion analysis of a unilateral 90° cutting task (Figure 1). Kinematic and kinetic data were recorded simultaneously using an 8 camera motion system (VICON, Oxford Metrics Ltd, London, England) sampling at 240Hz and three embedded force plates sampling at 1080Hz (Bertec, Worthington, OH, USA). Twenty-two retroreflective markers were placed on bony landmarks by one investigator (AA) with excellent inter-rater and intra-rater reliability (ICC>0.95) (Appendix 1). A static calibration trial was then taken to create a model. For the 90° cut, participants planted their foot on the force plate and turned 90° to the contralateral side. Players were given a demonstration of the task and verbal instructions to, ‘Run forward, plant your foot forward, turn 90°, and keep running.’ Only trials with an entire foot strike on the force plate were accepted for data analysis. Foot angle at initial contact varied some between players. To ensure that players completed a 90° cut, trials were rejected if the foot was in greater than 45° of internal rotation. The mean number of trials rejected per participant for these errors was <1 trial. Approach velocity was not controlled for at the time of data collection. Instantaneous approach velocity was calculated in a retrospective manner by taking the first derivative of the position of the bottom pelvis marker at initial contact (defined as vertical ground reaction force >50N) on the closest of two preceding force plates; initial contact on the preceding force plates varied between individuals secondary to stride length. Three trials without errors were collected on both the right and left limbs, but only the second and third trials were analyzed secondary to higher reliability.27 Limb dominance was defined as the self-reported preferred kicking leg.
Data analysis
Markers for motion analysis data were labelled with Vicon Nexus (v 1.85 VICON, Oxford Metrics Ltd, London, England), and gaps in the markers were filled using Nexus’s spline based algorithm if gaps were less than five frames. Trials with gaps greater than five frames were excluded from the final statistical analysis. Inverse dynamics and rigid body analysis of motion analysis data was performed in Visual 3D using custom written scripts (C-Motion Inc., Germantown, MD, USA). Kinematic and kinetic data were low pass filtered at 6Hz and 40Hz respectively with a fourth order Butterworth filter.28,29 Peak hip adduction and internal rotation angles and peak knee abduction angles and external moments were analyzed. Moments were normalized to each participant’s body mass x height. Additionally, a composite measure was used to analyze changes in lower extremity valgus, which we termed “knee valgus collapse”. Since valgus collapse is a composite of hip adduction, hip internal rotation, and knee abduction, it was assessed at peak knee flexion angle as a global measure. The equation used for this was Knee Valgus Collapse=hip adduction angle + hip internal rotation angle + (knee abduction angle*-1), with (-) values indicating less knee valgus collapse and (+) values indicating more knee valgus collapse.18
Statistical analysis
Anthropometric differences between groups for: height, weight, age, and time between testing timepoints were assessed with independent t-tests. Differences between groups and timepoints for instantaneous approach velocity were assessed with a 2x2 (time x group) repeated measures ANOVA. Peak hip adduction angles, hip internal rotation angles, knee abduction angles and moments, and knee valgus collapse were also analyzed with 2x2 (time x group) repeated measures ANOVAs with planned least squares comparisons and analyzed separately for the dominant and non-dominant limbs. Changes in kinematic variables were compared to previously published smallest detectable change (SDC) and minimal important difference (MID) values for the 90° cut to determine whether they were clinically relevant.27 Changes exceeding statistical significance (p<0.05) will be referred to as ‘statistically significant’, and changes exceeding the MID will be referred to as ‘clinically meaningful’. An a priori power analysis using preseason data of 31 subjects was completed, and indicated that to detect a change in dominant limb peak knee abduction angle that exceeded the MID of 2.0º (standard deviation: 3.09º) with power=0.80, 30 subjects would be needed.
Results
Approach Velocity
Forty-six participants (15 control, 31 intervention) had complete motion analysis data at the pre and postseason time points after accounting for unusable data due to marker dropout >five frames and subject dropout due to injury (Figure 1). There were no significant differences between groups for demographic variables (Table 1). Forty-three participants (13 control, 30 intervention) had instantaneous approach velocity data and instantaneous approach velocity data was not present for three participants since they did not contact either preceding force plate. There were no significant interactions between group and time point for instantaneous approach velocity. There was a significant main effect of group for approach velocity of the dominant and non-dominant 90° cut; the control group was 0.3-0.4m/s slower than the intervention group at both time points (Table 2).
Hip Kinematics
There was a significant interaction effect for non-dominant hip adduction angle (p=0.03) (Table 3), but changes in non-dominant hip adduction angle did not exceed the SDC.27 There was a main effect of time for dominant hip internal rotation angle (p<0.01). Dominant hip internal rotation angle decreased from preseason to postseason, and this change exceeded the SDC in both groups. There was a main effect of time for non-dominant hip internal rotation angle (p<0.01). Non-dominant hip internal rotation angle decreased from preseason to postseason, and this change exceeded the SDC in both groups. There were no other significant interactions or main effects that exceeded the SDC or MID for hip frontal and transverse plane variables.27
Knee Kinematics and Kinetics
There was a time main effect (p<0.01) for dominant knee abduction angle. Dominant knee abduction angle increased from preseason to postseason, and this change exceeded the SDC in both groups. There were no other significant interactions or main effects that exceeded the SDC or MID for knee sagittal or frontal plane variables.27
Valgus Collapse
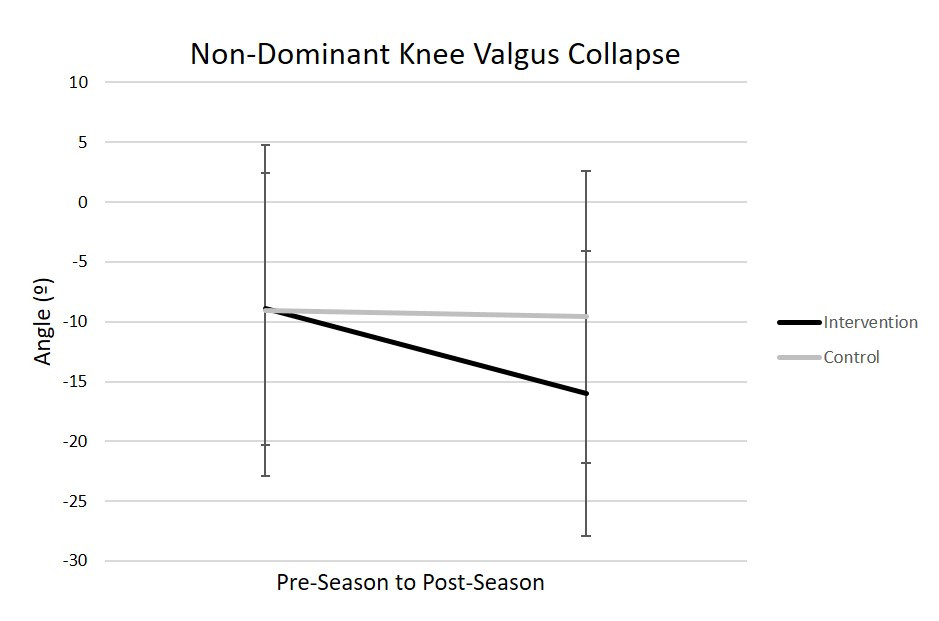
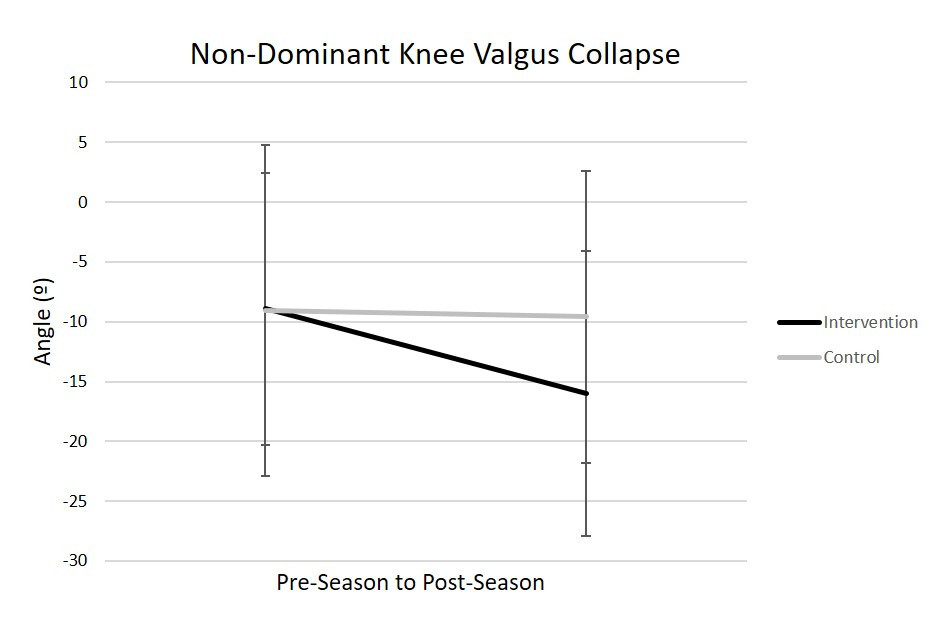
There was a main effect of time for dominant knee valgus collapse (p<0.01), but changes in dominant knee valgus collapse did not exceed the SDC for either group. There was a main effect of time for non-dominant knee valgus collapse (p=0.03). Non-dominant knee valgus collapse decreased from preseason to postseason, but only exceeded the SDC in the intervention group (Figure 2).
Discussion
The primary aim of this study was to determine whether the 11+ would reduce components of valgus collapse in female collegiate soccer players. The hypothesis was partly supported by the data. The intervention group demonstrated a statistically significant reduction in non-dominant hip adduction angle, a component of valgus collapse, and a clinically meaningful decrease in knee valgus on the non-dominant limb. Reductions in dominant and non-dominant hip internal rotation angle that exceeded the SDC were also observed. However, these changes were seen in both the intervention and control group participants so they cannot be attributed to participation in the 11+.
Knee valgus during a vertical drop jump has been cited as a risk factor for non-contact ACL injuries and has been used as a biomechanical measure of neuromuscular control.24 The soccer specific task of cutting has been used less frequently to identify whether biomechanical changes have taken place after implementation of an established injury prevention program.21,30,31 In this study, the intervention group demonstrated a 7.1° decrease in knee valgus collapse.27 Although this change did not reach statistical significance, it did exceed the SDC of 6.4°, indicating this is likely a true biomechanical change. So, this decrease in valgus collapse in the non-dominant limb may indicate a positive biomechanical effect of the 11+. This biomechanical change is especially interesting in the context of a sport-specific task like cutting. Video analysis of ACL injuries in male soccer players has demonstrated that players who tore their ACL while cutting were typically in knee valgus at the time of injury, suggesting that this is a hazardous posture for cutting maneuvers.32 Additionally, comparisons of the kinematics and kinetics of male and female athletes during a cutting task have indicated that female athletes tended to have greater knee valgus while cutting than male athletes.33,34 Previous literature has also demonstrated that sharper cutting angles lead to greater loads at the knee joint.25 So, a reduction in valgus collapse at a higher cutting angle, such as a 90° cut, may be especially advantageous for reducing ACL injuries. Further research is needed, however, to determine whether this change in biomechanics also corresponds with a reduced rate of ACL injury.
Despite these promising results, changes in valgus collapse exceeded the SDC but did not reach statistical significance and were only seen in the non-dominant limb. The lack of statistical change in valgus collapse may indicate the 11+ does not equally address movements in all planes of motion. Valgus collapse is a combination of frontal and transverse plane motions, but the majority of dynamic running exercises in the 11+ focus on sagittal plane motions. The balance and plyometric elements of the 11+ do address frontal plane knee control, however, these exercises may not represent typical injury scenarios. Minimal statistical changes in hip frontal and transverse plane biomechanics may indicate that players could benefit from additional dynamic neuromuscular training in the frontal and transverse planes of motion. Additionally, a low volume of unilateral exercises in the 11+ may be a shortcoming of the program and could help explain why biomechanical changes were not observed consistently in the dominant and non-dominant limbs. Since a 90° cut is a unilateral task with frontal and transverse plane biomechanical demands, there may not be a great enough volume of neuromuscular training specific to cutting in the 11+ to alter well-established playing biomechanics. Given the prevalence of cutting in a typical soccer match, it may also be valuable to implement cutting drills at a variety of angles with an emphasis on knee alignment during the cut.
High peak knee abduction moments have previously been identified as a risk for non-contact ACL injury.24 The intervention group participants in this study did not demonstrate significant changes in peak knee abduction moments despite demonstrating decreases in non-dominant knee valgus collapse. Intervention group participants also demonstrated a statistically significant decrease in non-dominant hip adduction angle during the 90º cut. Since hip adduction angle is a component of knee valgus collapse, this may indicate that biomechanical changes at the hip are driving changes in valgus collapse versus changes at the knee. Consequently, this may help explain why postseason changes in knee abduction moments were not observed in this study.
Although there is strong evidence that the 11+ is effective in reducing ACL injury rates, there has been low implementation of it.16,17,35 Time and adherence are two highly ranked barriers to long-term implementation of injury prevention programs such as the 11+.36–38 High player adherence has also been linked to a greater reduction in injuries.14,39 The coaches for the intervention teams in the current study completed a digital contract and agreed to complete the 11+ three times a week. However, individual player exposure and program progressions were not recorded, which is a limitation of this study. Access to individual player compliance information may have allowed for more detailed statistical analysis on how individual exposures to the 11+ affects player biomechanics. Future research should examine whether individual player exposure to an intervention like the 11+ effects magnitude of biomechanical changes, as previous research examining individual and team compliance to an intervention has demonstrated a greater reduction in knee injuries.40 However, monitoring individual player compliance and progressions can be difficult to implement, especially across multiple teams. Therefore, interpretation of the current results is limited by a lack of data to confirm a connection between adherence, biomechanical change, and ultimately reduction in ACL injuries. Establishing this connection may help improve the perceived time investment of an injury prevention program such as the 11+ and ultimately increase implementation.
A limitation of this study was not controlling for approach velocity of the 90° cut. Although there was a significant main effect of group, there was not a significant time x group interaction or main effect of time for instantaneous approach velocity. This suggests that biomechanical changes across the season were likely beyond noise of the signal and not the result of changes in cut velocity between time points. Analysis of a pre-planned cut may also be a limitation of this study as there is evidence that unanticipated cutting has been associated with higher loads on the knee joint than anticipated cutting.41 It is possible that the results of this study may also have been different in a younger age group. The mean age of the intervention group participants was 19.1 years due to inclusion of collegiate soccer teams. There is evidence that neuromuscular training programs are most effective in reducing injuries in females younger than 18 years-old.42 Regarding biomechanics, Thompson-Kolesar et al determined that pre-adolescent girls participating in the 11+ for eight weeks demonstrated greater improvements in biomechanical, especially in knee abduction angle, than adolescent girls.43 The slightly older age (college) of the participants may have limited the biomechanical changes observed across the season. However, it is unknown if age of the study’s participants impacted biomechanical change. Limited information about individual player exposure to and progression of the 11+ throughout the season, was an additional limitation. In future studies, the authors would collect individual player compliance information.
One of the strengths of this study was that it investigated the biomechanical effects of the 11+ on a sport-specific task. The results of this study indicate that the 11+ may have the potential to positively impact players’ movement strategies in the context of a task that is regularly performed on the field and carries a risk for ACL injury. Another strength of this study was the comparison of biomechanical changes to SDC and MID values. These values allowed for deeper understanding of the clinical impact biomechanical changes with this task may have.
Conclusion
The principal finding of this study was that participation in the 11+ led to a clinically meaningful, although not statistically significant, decrease in knee valgus collapse in the non-dominant limb. There is a preponderance of evidence supporting the implementation of a neuromuscular training program, such as the 11+, in female athletes.14,44 This study adds to the existing evidence that neuromuscular training programs are beneficial to female soccer players as it suggests that the 11+ may have the potential to reduce risky biomechanical patterns during the sport-specific task of cutting. Regardless, there is overwhelming evidence that female soccer players should be consistently participating in some form of neuromuscular training, that includes strength training and plyometric components, to reduce the risk of injury.14
Acknowledgements
Thank you to the University of Delaware, Temple University, and Wilmington University women’s soccer teams, coaches, and athletic training staff for their participation in this study. Thank you to Kelsey O’Donnell and Elise Krause for their assistance in data processing.
The work of Celeste Dix was supported by National Institutes of Health [T32 HD007490]. The work of Amelia Arundale was supported by the National Institutes of Health [R01 AR048212 and R44 HD068054] and a Foundation for Physical Therapy Promotion of Doctoral Studies I Scholarship. The work of Holly Silvers-Granelli was supported by the National Institutes of Health [R44 HD068054]. The work of Ryan Zarzycki was supported by the National Institutes of Health [R37 HD037985].
Conflict of interest
All authors declare no conflicts of interests.
Erratum
Biomechanical Changes During a 90º Cut in Collegiate Female Soccer Players With Participation in the 11+ Volume 16 , Number 3, June 2021, Pages 671-680. PMID: 34123519
This paper was originally published with a minor error in Table 3. The Non-Dominant Pre-Season abduction moment and ANOVA p-values are presented incorrectly. This error does not change any calculations or results in the paper, and the paper has had the Table corrected.
Sincerely,
Celeste Dix PT, DPT, PhD, SCS
The Editorial Staff at IJSPT