
INTRODUCTION
The repetitive pattern of muscle use can cause specific muscular adaptations and bilateral strength deficiency, or muscular strength imbalance between antagonistic muscles of the joint, mainly in asymmetric sports.1 The muscular isokinetic strength profiles of athletes may help in understanding these specific muscular adaptations for each sport.2,3
Muscular strength balance between agonist and antagonist muscles is of fundamental importance for joint stability, ensuring a dynamic centering of the humeral head,3 mainly while an athlete is playing sports.2 Therefore, the strength balance ratio is of fundamental importance, independently of the athlete’s sex. Traditionally, isokinetic strength testing has been considered an important tool for monitoring training adaptations and for objectively quantifying the strength balance ratio between agonist and antagonist muscles.4–6 Regarding the shoulder joint, rotator cuff shoulder muscles exhibit an important action that ensures dynamic centering of the humeral head to the glenoid.3 Edouard et al.7 showed that the relative injury risk of the shoulder joint was 2.57 if athletes had an imbalanced muscular strength profile. For this reason, it is important to have appropriate balance between shoulder internal (IR) and external (ER) rotator muscles.2,8,9
Many studies have grouped different sports together and, in many cases, have evaluated isokinetic strength and the effect of exercise programs in a broad category of “overhead athletes”.6,10–12 However, it is unknown whether shoulder muscular balance ratios are similar between overhead sports. If the balance ratios are different between sports, analyzing the balance ratios together may be erroneous. To the best of the authors’ knowledge, there are no data that suggest that muscle adaptations due to overhead sports are similar to justify grouping overhead sports. Several studies have evaluated adaptive changes in the shoulder in athletes of several different sports, such as judo,13 handball,7,9,14,15 tennis,9,10,16,17 baseball,18,19 badminton,20 volleyball,9,10 and swimming,21 but no studies have compared the strength balance between overhead sports.
Overhead movements are the main gesture in sports such as volleyball, handball, tennis, swimming, and baseball, but there are several distinctions between these sports. They have different movement executions and muscular actions, and they use different implements, such as different types of balls or rackets.9 Thus, it is important to know if these differences produce unique adaptations in shoulder strength balance. Knowledge about differences between the overhead sports in terms of muscle adaptation could help design tailored prevention and rehabilitation programs for athletes. Thus, the aim of this study was to compare the strength balance ratios between overhead athletes from the different sports. It was hypothesized that strength balance ratios would be different between overhead athletes in different sports, supporting the notion that these athletes should be investigated based on their specific sport rather than categorized as general overhead athletes.
METHODS
Participants
Athletes were recruited from competitive teams (regional level) in São Paulo (Brazil) through direct contact from January to September 2017. To this end, the research coordinators visited the teams and invited the coaches and athletes to participate in the study. Data were collected from February to October 2017. Volunteers were from eight different sports: volleyball, handball, swimming, judo, baseball (for men) and softball (for women), functional movements performed at high-intensity interval training, tennis, and soccer. Soccer athletes served as a control group, since there is minimal upper limb involvement in this sport (goalkeepers were excluded from the sample).
To be included, athletes had to have trained at least two hours per day, five times per week during at least the last two years. Exclusion criteria included activity or resting shoulder pain (greater than 3 out of 10 on the visual analogic scale),22 upper limb swelling, inability to perform physical exercises, systemic diseases, surgery in the last year, orthopedic injuries, interrupted physical training because of shoulder pain in the last six months, and/or other dysfunctions that limit the ability to complete the testing protocol.
The participants and/or their parents/guardians (for those under 18 years old) were informed about the aim of the study and gave their written consent to participate in the protocol. In addition, athletes under 18 years old gave their written consent before participation. All experimental procedures were approved by the Research Ethics Committee of the Universidade Federal de São Paulo and conformed to the principles outlined in the Declaration of Helsinki.
Isokinetic strength test
Before each test, the dynamometer was calibrated according to the manufacturer’s specifications. Athletes assumed a seated position, and standard stabilization strapping was placed across their chest and hips (Figure 1). The ER and IR rotator muscles from the dominant shoulder were assessed with the athletes’ upper limbs abducted at 90 degrees (deg) in the frontal plane and the elbow flexed at 90 deg, which is the same position adopted for shoulder muscle isokinetic evaluation in previous studies.23–25 This position has been recommended for evaluations because it approximates the throwing position.23,26,27 The range of motion was set to 50 deg of IR rotation and 70 deg of ER rotation to replicate an overhead serving motion27 and to be the same angles used in previous studies.5,24,28,29 Before the isokinetic test, athletes performed a five-minute warm-up exercise protocol,30 followed by low-intensity dynamic stretching exercises for lower limbs, to avoid stretching influence in strength values.31 Following the warm-up period, athletes randomly completed concentric and eccentric isokinetic shoulder strength tests with the dominant limb using an isokinetic dynamometer (System 4 Biodex Medical Systems Inc., Shirley, NY, USA). Before the test, the athletes performed three trial movements with submaximal performance to familiarize themselves with the equipment, angular speeds, and concentric and eccentric actions.

The concentric test consisted of five maximal repetitions of shoulder IR and ER at 60 and 240 deg/sec, respectively.29,32,33 The angular speed of 60 deg/sec was chosen as the lowest angular speed to avoid high joint pressure while producing the highest torque values.34,35 Additionally, 240 deg/sec was chosen as the highest speed, once it is close to the functional movements speed without increasing the risk of injury associated to eccentric action.36 Other studies have also used the same isokinetic test speeds for isokinetic strength evaluation.28,29,32,33 The eccentric test consisted of five maximal repetitions at 240 deg/sec. Between sets, participants had 60 seconds of rest time.14 All athletes were tested by a single evaluator who was trained and experienced in the use of isokinetic devices. During the test, athletes were given the same verbal encouragement. Visual feedback from the computer screen was not permitted. The variables evaluated were the shoulder ER and IR peak torque in concentric action at 60 and 240 deg/sec, respectively, and ER rotator peak torque in eccentric action at 240 deg/sec. With this information, conventional (CR) and functional balance ratios (FR) were calculated. The CR was calculated as concentric ER peak torque at 60 deg/sec to concentric IR peak torque at 60 deg/sec (ERconcentric:IRconcentric). The FR was calculated as eccentric ER peak torque at 240 deg/sec to concentric IR peak torque at 240 deg/sec (EReccentric:IRconcentric).
Statistical analysis
The normal distribution of each variable was analyzed and confirmed by the Kolmogorov–Smirnov test. The homogeneity of the variance was verified by Levene’s test. All variables were shown as the mean and standard deviation (SD). To compare sports, one-way ANOVA was used. ANOVA was complemented by the Tukey post-hoc test when the threshold of significance was reached. Statistica software (version 12.0, USA) was used to process the analyses. The level of significance was set at p < 0.05 and the power level at 0.80.
RESULTS
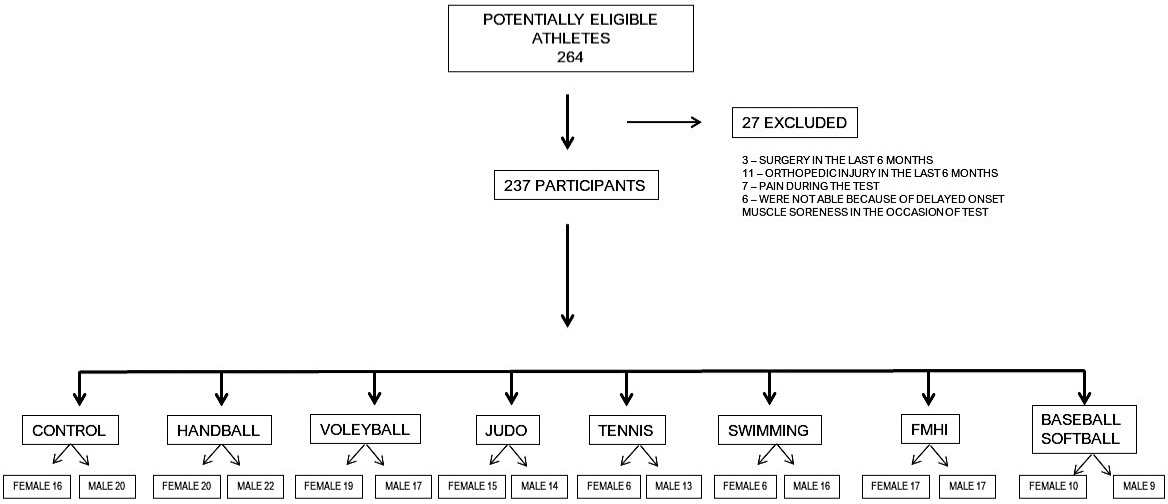
Two hundred and sixty-four athletes were screened for participation, and of these, 27 were excluded, so 237 athletes comprised the sample. The 27 athletes excluded from the initial sample were as follows: 3 had upper limb surgery, 11 suffered an orthopedic injury in the last six months, and 13 fell pain during the test. Figure 2 shows the participants’ flow through the study.

The characteristics of the athletes are described in Table 1. One-way ANOVA revealed a statistically significant difference between ages of the female groups (F[7,101]=12.32, p<.001, observed power 1.0) and of the male groups (F[7,120]=15.81, p<.001, observed power 1.0). There was also a significant difference between body mass of the female groups (F[7,101]=10.53, p<.001, observed power 1.0) and of the male groups (F[7,120]=7.37, p<.001, observed power .99). Regarding height, there was also a significant difference between female groups (F[7,101]=22.99, p<.001, observed power 1.0) and male groups (F[7,120]=6.93, p<.001, observed power .99).
The values of CR and FR of male and female athletes from different sports are shown in Table 2. One-way ANOVA revealed a statistically significant effect of sport on CR in the female group (F[7,101]=3.55, p=.002, observed power .96) and in the male group (F[7,120]=2.29, p=.031, observed power .82). There was also a significant effect of sport on FR in the female group (F[7,101]=7.10, p<.001, observed power .99) and in the male group (F[1,120]=9.65, p<.001, observed power .99).
The significant p-values for the differences between sports are shown in Table 3. Male athletes had no CR differences between sports. Moreover, the overhead athlete groups were not different from the control group. Conversely, female athletes had significantly higher CR values in the softball group than in the judo (p <.01), volleyball (p=.04), and swimming groups (p=.04) (Tables 2 and 3).
For the FR in the male athlete groups, the judo athletes had lower FR than the controls (p<.01), volleyball athletes (p<.01), swimmers (p<.01), functional movements performed at high-intensity interval training athletes (p<.01), and baseball athletes (p=.01). Tennis and handball athletes also had lower FR values than controls and volleyball athletes (p<.01). Moreover, tennis athletes also had lower FR than swimmers (p=.04) (see Tables 2 and 3). The female judo athletes had lower FR compared to the control group (p<.01), volleyball (p<.01), functional movements performed at high-intensity interval training (p<.01), and softball (p<.01) athletes. Female handball athletes showed lower FR values than the control group (p=.02) and softball athletes (p<.01).
DISCUSSION
The aim of the current study was to compare the CR and FR between overhead sports (volleyball, handball, swimming, judo, tennis, functional movements performed at high-intensity interval training, and baseball/softball) with a control group composed of soccer athletes. The main findings were that the CR was not significantly different between all male overhead sports and between the overhead sports and the control group. Only female softball athletes had a higher CR than female judo, volleyball, and swimming athletes. Conversely, the FR was significantly different between the sports evaluated. In the female group, the judo and handball athletes had lower FR values, and for male athletes, judo, handball, and tennis athletes had lower FR values.
Softball athletes had the highest CR. High values for this variable indicate weakness of the shoulder IR rotator muscles relative to the strength of the ER rotator muscles. The specificity of the throwing movement of this sport may contribute to this finding. Indeed, a softball throw is substantially different from other sports. At the moment a softball is thrown, the shoulder joint has less than 90 deg of flexion. Consequently, the shoulder’s IR action is not as clear as with other sports that involve an overhead throw, using more than 90 deg of shoulder flexion.37 Ellenbecker and Davies8 suggested that the CR should be between 66% and 75% in order to establish good joint stability and to avoid shoulder injuries. Therefore, besides the softball athletes presenting higher CR values (90.4 ± 13.6%) than the judo (67.3 ± 6.9%), volleyball (74.9 ± 15.9%), and swimming athletes (70.3 ± 8.7%), the softball group also had values that were higher than the recommended values in the literature. To the best of the authors’ knowledge, there are no previous studies about isokinetic shoulder strength balance in softball athletes. Therefore, these are the first data showing shoulder strength imbalance in these athletes. Given that there were no significant differences in the CR between the female control, handball, volleyball, judo, tennis, swimming, and functional movements performed at high-intensity interval training groups, it is reasonable to suggest that these sports could be analyzed together in future studies. CR for all the male groups evaluated in this study were all similar; therefore, it is also reasonable that the CR data for men from the overhead sports in this study can be grouped and analyzed together.
Male athletes from the functional movements performed at high-intensity interval training modality—besides presenting CRs that were not significantly different from the other sports —had a mean CR value lower (63.5 ± 8.8%) than the literature recommendation (66–75%),8 which is also lower than previous literature data for this sport.29 Athletes from the functional movements performed at high-intensity interval training modality characteristically applied a powerful sportive gesture, especially related to the shoulder IR muscle. In functional movements performed at high-intensity interval training, there are no throwing actions, which could limit the development of the shoulder ER muscles. This situation corroborates the presence of a low CR.13 Hadzic et al.38 evaluated volleyball athletes’ IR and ER muscles in the same angular speed and test position. The authors found CR of 61% and 74% for male and female athletes, respectively. Female volleyball athletes from the current study had very similar results (75%), but male volleyball athletes had a higher CR (81%). Comparing handball athletes from the current study with previously published data from the same test angular speed and position, similar values were observed for the CR. Andrade et al.14 found a CR of 79% for female handball athletes, and Andrade et al.15 found the CR to be 72% for male handball athletes, while the current study found it to be 76% for female and 67% for male handball athletes.
For the female group, judo athletes had the lowest FR values, which were significantly lower than the values in the control, volleyball, functional movements performed at high-intensity interval training, and softball groups. The second lowest FR values were in handball athletes, which were lower than in the control and handball groups. The FR is characterized by the ER peak torque in eccentric action divided by the IR peak torque in concentric action; therefore, lower values indicate a low eccentric strength of ER muscles. Noffal36 hypothesized that eccentric ER torque should be greater than concentric IR torque to be able to overcome and to decelerate the shoulder movement generated by the concentric action of IR muscles. The results in female judo and handball athletes were not only lower than those of the other studied groups, but their mean values were also lower than those reported for shoulder stability (FR > 1.0).36 Regarding female handball athletes, the data reported in the literature14 were higher than those observed in the current study. These authors found a FR of 1.21 ± 0.28 for the dominant upper limb; however, these authors evaluated the isokinetic strength at 300 deg/sec, and the higher speed used in their study could be responsible for the higher FR values. Along these lines, Edouard et al.7 found lower FR values (0.75 ± 0.15) for a population with the same characteristics; however, they assessed the isokinetic strength at 60 deg/sec. In the present study, a higher angular speed test (240 deg/sec) was chosen because it was closer to the functional throwing action than the lower speed (60 deg/sec) selected by Edouard et al.7 Conversely, an angular test speed higher than 240 deg/sec was not employed because it is hard for athletes to perform eccentric action at angular speeds that are too high (commonly they cannot reach very high eccentric speeds). Therefore, it is difficult to compare study results because the angular speeds tested were different.
Similar to the female group, the male judo and handball athletes, in addition to the tennis athletes, also had low FR values. The judo athletes had lower FR than the control, volleyball, swimming, baseball, and functional movements performed at high-intensity interval training athletes. Likewise, handball and tennis athletes had lower FR values than the control and volleyball groups, and tennis athletes also had lower FR than swimmers. Andrade et al.5 evaluated handball athletes and assessed muscular isokinetic strength at 90 (concentric mode) and 300 deg/sec (eccentric mode) and also found mean FR values lower than 1.0. Additionally, Saccol et al.16 observed FR lower than 1.0 for tennis athletes.
Strength evaluations at different isokinetic angular speeds were not performed, which could be considered a study limitation; it could be helpful to compare the results with previously published data. Therefore, future studies should be performed at different speeds. Another recommendation for future studies is to include other sports commonly grouped in overhead classification, such as badminton, water polo, or lacrosse.
Conclusions
CR for male overhead athletes may be analyzed together because there were no significant differences between them. However, for females, CR for softball athletes should be analyzed individually because they had higher values. As the FR for the male group had several differences across overhead sports, grouping all the evaluated sports, in order to evaluate these variables, should be done carefully. The sports that can be grouped together based on the FR analysis are volleyball, swimming, functional movements performed at high-intensity interval training, and baseball, or in a different group handball, judo, and tennis. For analyzing FR in a female group, overhead athletes (volleyball, swimming, softball, functional movements performed at high-intensity interval training, tennis) may be grouped and analyzed together, as there were no differences between them; only female judo and handball athletes should be excluded from the group. In general, these results could have important implications for the design of training programs and injury prevention, as well as rehabilitation programs associated with the shoulder joint and “overhead athletes.”
Conflicts of Interest
The authors declare no conflicts of interest.