
INTRODUCTION
Analysis of how to improve the safety of all amateur sports participants is an area of interest for multiple groups including players, coaches, caregivers, and medical care providers. Protecting youth baseball players from preventable injuries is imperative considering there are over 200,000 youth baseball teams in the United States.1 Systems to reduce the incidence of overuse injuries include limiting pitch counts (during games, weeks, seasons), allowing for periods of time (months) without pitching, limiting participation in multiple leagues, regulating pitch type, and learning appropriate throwing mechanics.2–6 There are a number of sources that baseball players, caregivers, and coaches can use to learn about safe pitching practices, a majority of which can be found online (Table 1 and Table 2). Despite the accessibility of information regarding safe pitching practices, little league pitchers continue to experience overuse injuries.
A study performed by Fazarale et al. provided a questionnaire to youth baseball coaches in their region concerning the USA Baseball Medical and Safety Advisory Committee (USA BMSAC) pitching guidelines.3 Seventy-three percent of the coaches reported compliance with the recommendations, yet only 43% of the questions regarding pitch count and rest periods were answered correctly. The coaches surveyed believed that only 53% of other coaches in their league followed the guidelines. Furthermore, 19% of these coaches knew that at least one of their players pitched in a game with a sore or fatigued arm. This is of particular concern because many sports medicine experts see shoulder and elbow pain not as an innocent symptom, but rather a warning sign of an acute or developing overuse injury.1
Caregivers and youth baseball players often rely on coaches to enforce safe pitching practices, however previous data has demonstrated that this may not always be consistent.3,6 Petty et al. evaluated risk factors for ulnar collateral ligament (UCL) injury in high school pitchers. In their patient population only 13 of 25 pitchers (52%) believed their coaches were proactive about preventing throwing injuries. They also reported situations where they believed they were overthrowing, including pitching during playoff games, tournaments, and showcase tryouts.6 Additionally, youth pitchers themselves have demonstrated a substantial lack of comprehension of appropriate pitching practices, with as many as 85% reporting never having heard of USA BMSAC guidelines and 57% indicating that they would not seek medical help if they had throwing arm pain after a game.7
The failure of appropriate education can occur at many levels, including ignorance that guidelines exist, lack of awareness of where to learn about guidelines, inaccurate provision of information by coaches, and failure to understand the overall importance of guidelines. To date, no study has evaluated the knowledge that each child’s caregiver possesses. The primary purpose of this study was to evaluate how knowledgeable youth baseball caregivers were about safe pitching guidelines and secondarily determine pitching practices which may be associated with increased risk of player injury.
MATERIALS AND METHODS
This cross-sectional survey study was approved by the University of Florida Institutional Review Board. A twenty-two question survey was distributed to the caregivers of youth baseball pitchers between the ages of 7 and 18 years old across North Central Florida. Locations utilized for distribution included regional baseball fields during practices and games, the Orthopaedics and Sports Medicine Institute clinics, and affiliated physical therapy/rehabilitation centers in order to reduce bias. The survey was constructed to capture questions on caregiver demographic data, knowledge of throwing guidelines, athlete pitching background and throwing habits based on recommendations provided by the USA Baseball and Medical Safety Advisory Committee, Little League Baseball, and the American Sports Medicine Institute (Appendix 1). The caregivers of the youth pitchers were asked to complete and return the survey. The results of each survey were then placed into a deidentified database using the Research Electronic Data Capture (REDCap)8 application at the University of Florida. Chi-square analysis was used to evaluate the categorical variables with the level of significance set a-priori at p 0.05. As guidelines stratify recommendations based on specific age brackets, a separate subgroup analysis was performed between pitchers less than 13 years old and those 13 years or older to represent youth athletes and those in adolescence.9
RESULTS
Population Characteristics
The survey resulted in 102 responses, 98 of which were used for analysis. One survey was excluded because it pertained to a baseball player who was not a pitcher and three others were completed by someone who was not the child’s primary caregiver. Fifty-two percent (51/98) identified themselves as the child’s mother. Ninety-one percent (89/98) of the respondents were Caucasian, and forty percent (39/98) of respondents fell within the 41 to 50 year-old age group. Of those surveyed, thirty-eight percent (37/98) were the caregivers of a pitcher between the ages of 13 and 16. With regards to education, seventy-six percent (74/98) had an associate’s degree, bachelor’s degree, or advanced degree (Table 3).
Survey Results
Eighty-three percent (81/98) of those polled were unaware of the existence of safe pitching guidelines. Fifty-three percent (52/98) of the surveyed population did not actively participate in monitoring their child’s pitch count. Seventeen percent (17/98) of the caregivers were unaware of how many pitches their children throw in a typical game. In children 13 years and older, if their caregiver was aware of pitching guidelines, they were more likely to estimate their child threw less than 85 pitches per game (p < 0.05).
Forty-four percent (43/98) of the pitchers threw in more than one league at a time while eighteen percent (18/98) pitched at least nine months out of the year. Participation in extra showcase scenarios was reported by fifty-eight percent (57/98) of caregivers and twenty-eight percent (27/98) of the youth pitchers participated in four showcase camps or more annually (Table 4). When not pitching, eleven percent (11/98) of the population identified catcher, twenty-six percent (25/98) outfield, and sixty-one percent (60/98) infield as their child’s primary position.
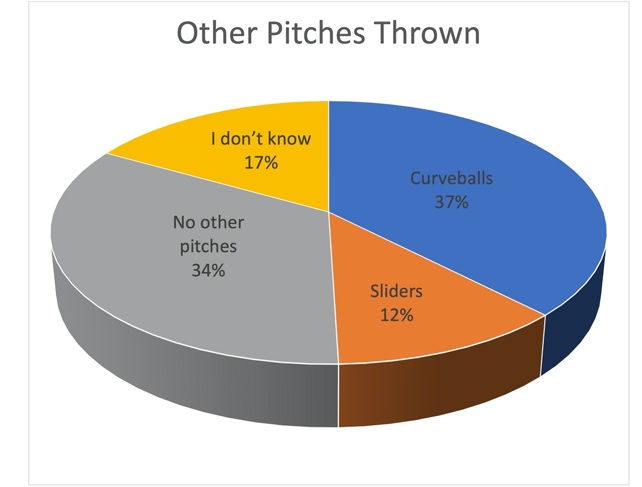
Seventeen percent (17/98) of the caregivers surveyed did not know what kinds of pitches their children throw. Thirty-four percent (34/98) only threw fastballs, change-ups and knuckle balls while fifty-one percent (50/98) also threw breaking pitches (Figure 1). Forty-two percent (41/98) of children were taught pitching technique by their coach, followed by twenty-seven percent (26/98) with a hired instructor, twenty-one percent (21/98) answering “other”, and twelve percent (12/98) taught by a caregiver (either the respondent or their spouse).

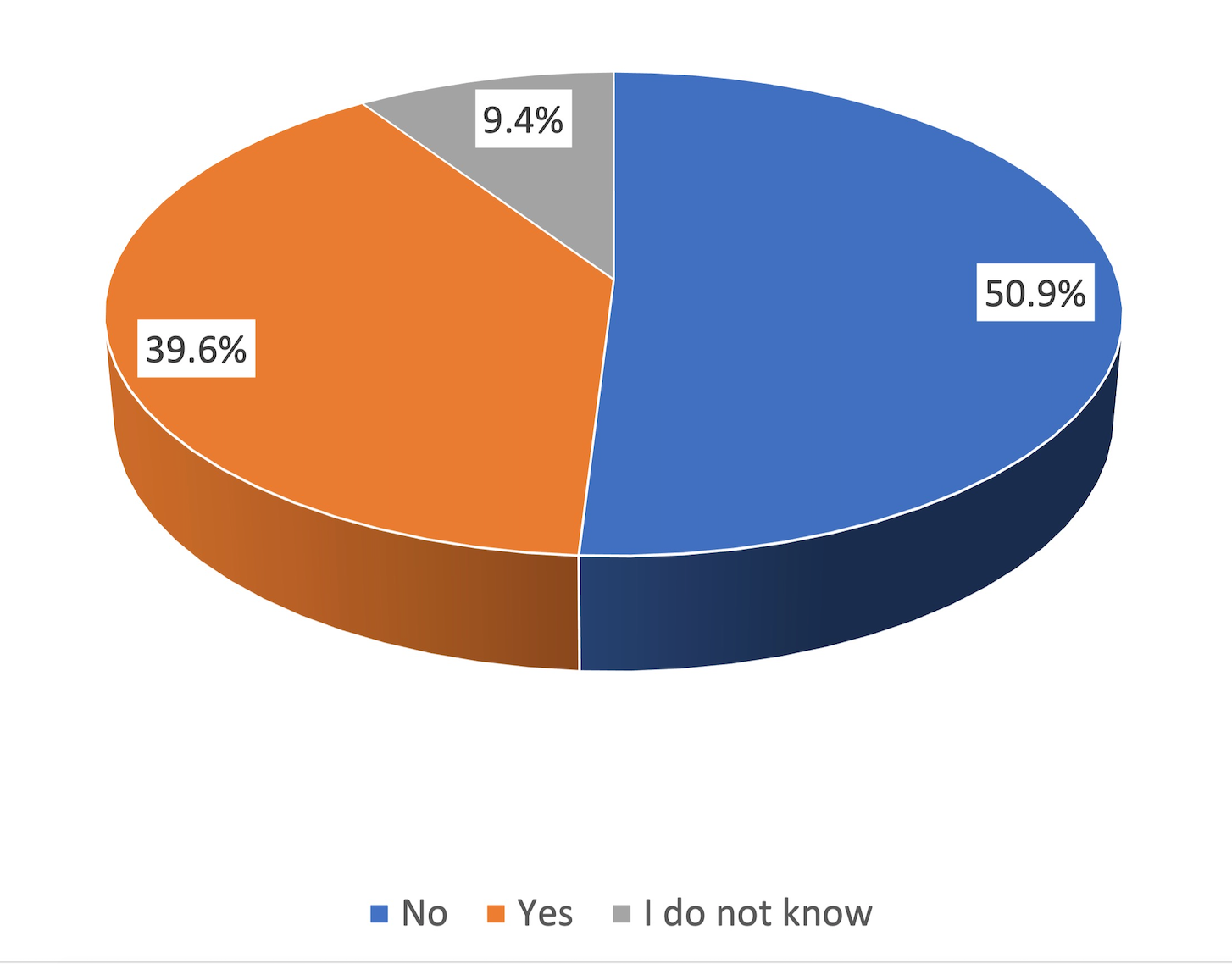
Fifty-two percent (51/98) of the caregivers recalled their child having upper extremity pain as a direct result of pitching, which was located twenty-three (45%) times in the shoulder and nine times in the elbow (18%) (Table 5).
Twenty-six percent (25/98) of the pitchers had to miss either a game or a pitching appearance because of their throwing arm pain, and twenty-seven percent (26/98) experienced pain concerning enough to be evaluated by a medical professional (Table 6).
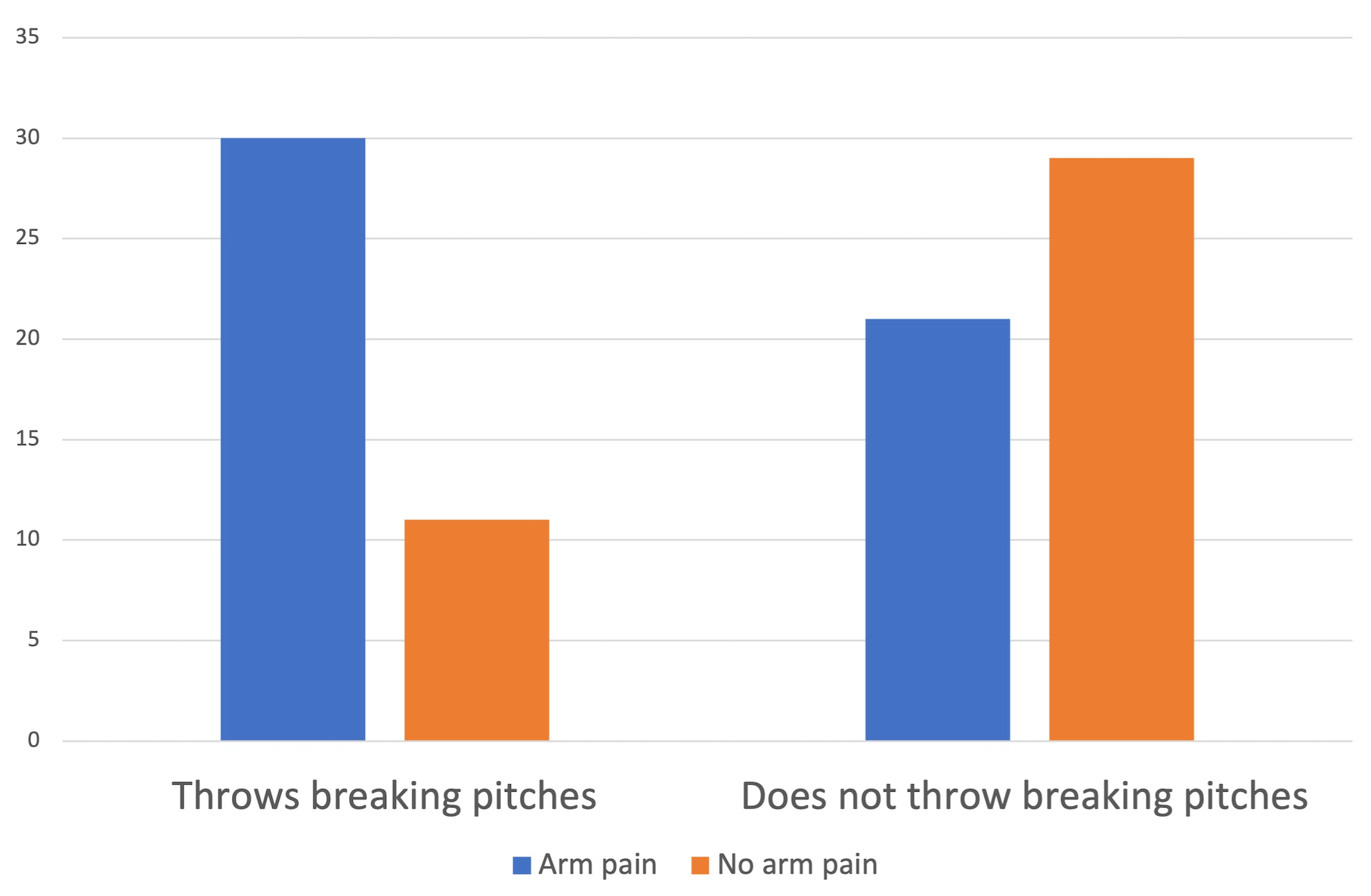
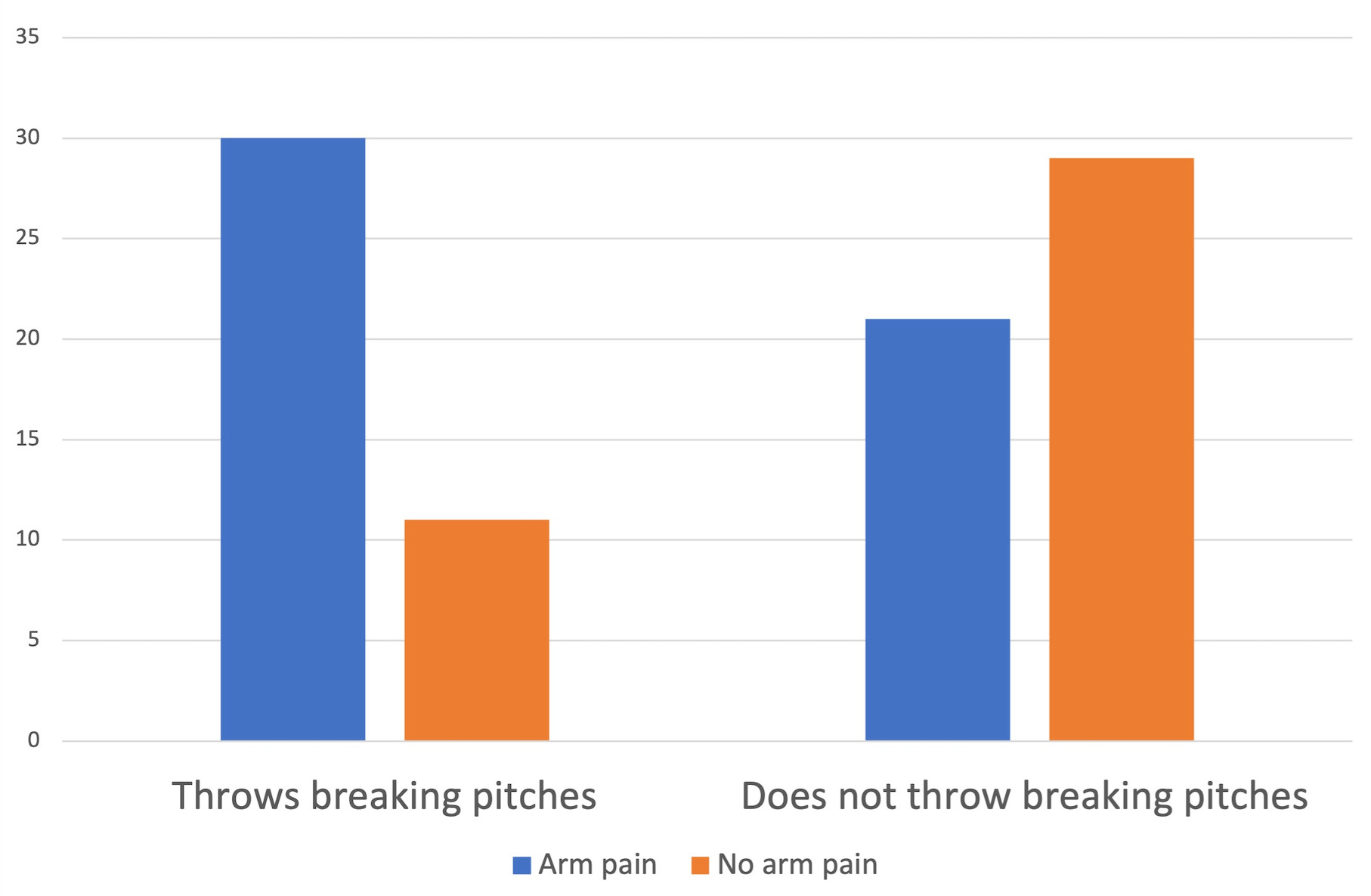
Those pitchers who threw breaking pitches or threw for more than six months out of the year were more likely to experience arm pain after a pitching performance (Figure 2a and Figure 2b, Figure 3; p < 0.05). There was also a general trend toward significance noted in regards to increasing number of months pitching out of the year and arm pain (p = 0.059).
Variable Correlations
Compared to pitchers younger than 13, players 13 years and older were more likely to throw curveballs (25% compared to 12%; p < 0.05). Additionally, children 13 years of age and older were more likely to miss games because of throwing arm pain (20% compared to 6%; p < 0.05).
Using the same age cutoff of 13 years, there was no statistically significance difference found between awareness of youth pitching guidelines, number of pitches typically thrown in a game, position when not pitching, and who keeps track of pitch count (p > 0.05).
DISCUSSION
Overhead throwing creates an environment of significant mechanical stress. During the pitching motion, the kinetic chain transfers energy from the lower extremity, through the trunk, and finally through the upper extremity. The shoulder and elbow are sensitive to biomechanical stress and prone to pathology because they are inherently less stable joints and near the end of the energy transfer. Individuals who are involved in repetitive events, like pitchers, can be disposed to anatomical and mechanical changes in the throwing arm commonly presenting as overuse injuries.1,10,11
Eighty-three percent of baseball caregivers were unaware of safe pitching guidelines. Given the potential catastrophic complications that can occur from overhead pitching at an early age, the medical community should continue to make data-driven recommendations to best prevent irreparable damage. Many researchers have recognized that prevention of acute and chronic injuries stems from a multidisciplinary approach that includes sports medicine providers, coaches, and caregivers.1,6,12 Limpisvasti et al. recommended that injury prevention in youth baseball begin as early as possible. This is particularly true for those who have the opportunity to play at higher levels, as many of the injuries sustained later in a players’ career are speculated to be the culmination of insults that began at a young age.1
The overall rate of baseball overuse injuries has been estimated at 5% in some studies, with an injury rate of 1.39 per 10,000 athlete-exposures (AEs) for the shoulder and 0.86 per 10,000 AEs for the elbow.13,14 In their patient population, Andrews et. al showed that pitchers sustain the majority of shoulder (39.6%) and elbow (56.9%) injuries which were most often caused by overuse. From this same study 10.8% of shoulder injuries and 3.6% of elbow injuries required surgery.14 In this population, 26% of the pitchers had to miss at least one game because of throwing arm pain, and 27% had pain severe enough to require an evaluation by a physician. This number remains unacceptably high and merits further investigation into the failure of preventative measures.
Olsen et al demonstrated that the amount of pitching is the strongest risk factor that correlates with shoulder and elbow pathology. They determined that throwing greater than 80 pitches per appearance and pitching competitively more than eight months per year increased the odds of an injury requiring surgery by 3.83 and 5.05, respectively.15 Despite no statistically significant difference between average number of pitches thrown during a game and throwing arm pain, these findings otherwise support this conclusion with players throwing for greater than six months associated with a significant increase of throwing arm pain. Promisingly, only eighteen percent of participants pitched during nine or more months out of the year. In addition, Zaremski and Farmer demonstrated a highly likelihood of UCL reconstruction in athletes playing in the Southeastern Conference (SEC) compared to more northern conferences. This parallels the playing environment of pitchers from this study as rosters in the SEC consisted of a greater number of players from southern states and were more likely to have grown-up playing baseball year-round.16


There are recommendations to limit the number of different leagues, teams, and showcases in which pitchers participate based on outcomes reported in previous retrospective reviews.17 Seventy-seven percent of players did not participate in other sports beside baseball during the season and only thirty-nine percent did play another sport outside of the baseball season. Although a growing trend and widely prevalent, early specialization in sports has been demonstrated to lead to higher rates of injury, increased psychological stress and loss of interest in playing.18 In this sample population forty-four percent of those surveyed reported that their child pitched in more than one league concurrently. Furthermore, while fifty-eight percent of pitchers participated in at least one showcase camp annually, twenty-eight percent participated in four or more. In many circumstances, pitchers have different coaches for each team or showcase. This leads to a lack of continuity in regulating pitch counts and appropriate time off. These situations demonstrate the importance of caregivers becoming both knowledgeable and compliant with safe pitching practices, yet the findings from this study demonstrate that at least fifty-three percent of youth pitchers will not have appropriate oversight.
Overuse injuries of the shoulder and elbow can be exacerbated by other repetitive overhead activities outside of pitching. Data published in 2001 demonstrated that a pitcher who also plays catcher is 2.7 times more likely to sustain a serious throwing arm injury.19 Additionally, Fleisig and Andrews noted that the shoulder and elbow microtrauma created during pitching may not have adequate time to resolve when pitchers also play catcher.13 These studies in part form the basis of the recommendation that a pitcher should not also play catcher for their team. Encouragingly, in the population of this survey only eleven percent of the baseball players identified playing catcher as their primary position when not pitching and although sixty-one percent reported playing in the infield secondarily, separate analysis did not find a significant association between alternate field position and throwing arm pain.
The appropriate age at which pitchers should begin to throw specific pitches has gained increasing interest in the sports medicine and baseball communities. Current recommendations from the American Academy of Orthopedic Surgeons (AAOS) are that pitchers should refrain from throwing breaking pitches (curveballs and sliders) until they are skeletally mature. This suggestion is more stringent than previous guidelines which recommended that pitchers not throw breaking pitches until 14 years of age.6 An article published in AJSM in 2002 investigated if there was a correlation between breaking pitches and injury by prospectively following 476 youth pitchers between the ages of 9 and 14 for a baseball season. They found that the curveball was associated with a 52% increase in shoulder pain while the slider increased elbow pain by 86%.10 Although questioned by more recent literature which has failed to find an increase in shoulder and elbow forces after breaking pitches compared to other types, in this population of pitchers analysis demonstrated a statistically significant relationship between those players who threw breaking pitches and throwing arm pain (p < 0.05).20,21 Nonetheless, 24% of pitchers under 13 years of age were reported to throw curveballs, and 10% in this same age group threw sliders. This result demonstrates that pitchers continue to participate in activities that are contrary to established guidelines. The reason for this may be unfamiliarity with the recommendations from coaches and caregivers or lack of knowledge regarding the association between types of pitches and throwing arm pain.
There are several limitations to this study which encompass the same confounding factors of other cross-sectional surveys. First, a majority of the surveys were administered to caregivers during athletic competition, while only a small amount were provided in a physician’s office or in physical therapy. This may lead to a selection and convenience sample bias, and may not be representative of the population at large. Similarly, this analysis illustrates only a specific geographical region (North Central Florida); therefore, the experiences in this location may not be characteristic of the rest of the country but are likely generalizable to other warm climate areas. More surveys were distributed than the total response of 102, and the nonresponse group may have answered differently which would have altered the results.
Several of the questions in the survey also ask specific details regarding pitch counts and days between performances – the nature of these questions is highly susceptible to recall bias. Although edited and tailored to focus on issues surrounding pitching, the questions may have unintentionally lead individuals or been misinterpreted. Additionally, private pitching lessons were not analyzed, which could have a dramatic effect on overall pitching volume.
Further directions based on the results of this study would include distributing either the same or a similar survey to multiple geographic locations so that all the data could be compiled into one data set for further review. These findings demonstrate a need for better education of youth baseball caregivers. One method of improving their knowledge of guidelines and access to resources would be for healthcare providers to participate in community outreach programs. The efficacy of these outreach programs could be evaluated by prospectively collecting data on shoulder and elbow injuries before and after their implementation.
CONCLUSION
No other study to date has sought to determine caregivers’ knowledge of safe pitching practices. Despite the implementation and accessibility of safe pitching guidelines, a large portion of those surveyed were unaware of or noncompliant with these established recommendations. These findings demonstrated an increase of throwing arm pain in youth baseball players pitching more than six months out of the year, suggesting that annual limitations on pitching performances be considered. Players 13 years and older were more likely to use breaking pitches and miss games due to throwing arm pain, supporting current guidelines from the AAOS that pitchers refrain from throwing breaking pitches until reaching skeletal maturity. Given the results of this study, further measures need to be taken to improve caregivers’ understanding of the guidelines to help increase compliance and protect youth pitchers. Injury prevention should be a multidisciplinary approach that includes educating coaches, caregivers, and youth pitchers. Future directions may include establishing outreach programs for the youth baseball community.
Support/Conflicts of Interest
No sources of support or conflicts of interest to disclose