INTRODUCTION
Alterations of the resting scapula position and dynamic scapular motion are frequently observed by sports physical therapists in patients with shoulder disorders from overuse injury in the overhead athlete.1–3 These alterations have been collectively classified by Kibler,4–7 three of which are thought to result in abnormal scapulohumeral rhythm and shoulder arthrokinematics and one that is considered normal scapular position.7 Abnormal scapulohumeral rhythm or dyskinesia can be considered either a cause or a result of shoulder disorders and adversely affect function.8 Evaluation of the Kibler classification can help in developing strategies to address shoulder dysfunction. During evaluation of the patient with shoulder dysfunction, scapular position should be examined statically and dynamically.9 The Kibler classification examination is a static scapular position test except for the last portion which involves observation of the position of the scapula in full shoulder flexion.
In terms of upper extremity performance, the Davies Closed Kinetic Chain Upper Extremity Stability test (CKCUEST) should be considered. The CKCUEST is a unique dynamic physical performance test because it assesses upper extremity function while most physical performance tests are related to the lower extremity.10–12 Most upper extremity sport activities involve closed kinetic chain activities. Closed kinetic chain upper extremity activities promote proprioception, joint stability, and high levels of activation of the scapular dynamic stabilizer muscles.13–17
The CKCUEST requires stability of the muscles that attach to the scapula, therefore, the CKCUEST may also be used as a scapular stability assessment. These scapular stabilizing muscles are active in both open and closed kinetic chain activities.17,18 The CKCUEST is a valid and reliable test that provides a measure of power and upper extremity stability.10,19 To perform the test, the participant is asked to assume a push-up position (men) or modified push-up position (females) and perform maximal speed alternating reaches to a tape target spaced 36 inches apart for 15 seconds. The number of touches to the tape is recorded for three 15-second trials. Three potential scoring outcome measures can be calculated from the CKCUEST: average number of touches, a normalized score, and a power score.20–22
The primary purpose of this study was to determine if a static scapular test, the Kibler scapula classification, in healthy participants affects the ability to perform a closed chain functional test that involves the use of the scapula and the upper extremity, the Davies CKCUEST. A secondary analysis was performed to evaluate the reliability of the student physical therapist and experienced physical therapist to identify scapular type by observation. The hypotheses were that those with a Type IV or normal Kibler scapula classification would perform better on the Davies CKCUEST and that students and experienced therapists would have a moderate (> 0.60) inter rater reliability of identifying scapular type by observation.
METHODS
Participants
Sixty-three healthy participants were recruited across two locations. Participants were recruited from two public university campuses by flyer and word of mouth from Wichita State University and Northern Arizona University. The local institutional review boards approved the study. All participants were informed of the benefits and risks of the study before signing an institutionally approved informed consent document to participate. Participants were required to be between 18 to 40 years old to participate and to be able to speak English. Exclusion criteria for the study included: currently pregnant, current bout of shoulder or upper body pain, diagnosis of any shoulder condition in the past year, diagnosed hypertension or respiratory distress. All participants were asked about each of these conditions to ensure appropriate ability to participate in this study.
INSTRUMENTATION
Kibler scapular classifications
Scapular classifications were described first by Kibler.7 Type I represents abnormal scapular control about a horizontal axis. Type II represents abnormal scapular control about a vertical axis. Type III represents excessive upward movement and abnormal control around a sagittal axis. Type IV is normal with bilaterally symmetric scapula. Multiple authors have investigated Kibler scapular classifications in the resting position that is with the participant standing in their normal posture with both arms at their sides therefore this was the case for this study.4,6,23,24 In the current study, Kibler scapular classifications were identified by visual observation.
Davies Closed Kinetic Chain Upper Extremity Stability Test
To perform the CKCUEST, the participant is asked to assume a push-up position and perform maximal speed alternating reaches to a tape target spaced 36 inches apart for 15 seconds. The number of touches to the tape is recorded for three 15-second trials.12 Some authors modify the push-up position for females by having the female in a kneeling position with knee support20,22,25 whereas others have concluded that the distance of the placement of the tape that is being reached to corresponds to anthropometric characteristics and maturational stages of the participant11,22 potentially putting a participant with a narrower build at a disadvantage. Authors have also modified the CKCUEST by performing only one trial11 or two trials26 as opposed to three trials.10,21,22 In the current study, female participants were offered a choice of the modified position or the standard push-up position and performed all three trials of the CKCST. Authors have suggested that CKCUEST scores can provide three potential scoring outcome measures from the CKCUEST: average number of touches, a normalized score, and a power score.20,22 The CKCUEST normalized score is obtained by dividing the number of touches by the height of the participant.20,22 The CKCUEST power score is obtained by multiplying the average touches by 68% of the participant’s body weight (kg) divided by 15.20,22
Procedures
Healthy participants aged 18 to 40 years old were recruited via flyers and advertising around the community. The order of procedures was the same for all participants. Each participant was weighed and height was measured followed by blood pressure and pulse rate being measured by a student physical therapist at both locations. Blood pressure was measured following the Frese et al27 guidelines and abnormal blood pressure or pulse rate excluded the participant from participation. A student physical therapist asked each participant to change into clothes to allow for visual observation of bilateral Kibler scapular positions with the participants limbs resting by the participant’s side and then the student physical therapist recorded the result. The student physical therapist then invited the faculty member into the room to evaluate bilateral Kibler scapular positions and record their results. One student and one experienced physical therapist evaluated Kibler position in each setting.
The student physical therapist then reviewed the Davies CKCUEST procedure with the participant. For all participants, female and male, two pieces of tape located 36 inches or 91.4 centimeters apart were placed on the floor. The participant was asked to assume a push up position and this became the starting position for the participant. Initially, the Davies CKCUEST starting position was performed with the hands spread apart to be touching the tape. Recently authors have suggested that placement of the hands in the starting position should correspond to the anthropometric characteristics of the participant.20,28 The participant was asked to move as quickly as possible alternating their reach to each piece of tape. A warmup trial was done to familiarize each participant before the three trials of the test. Between each trial, the participant was provided a 45-second rest as per protocol.20,22,25 The average of the three trials was used as the test score for each participant.
Statistical Methods
Sample size calculation was based on having 80% power for the primary outcome of scapular posture and performance on the Davies CKCUEST. Data were analyzed using SPSS v24 (IBM Inc, Armonk, NY). A p-value of less than .05 was considered statistically significant. A one-way analysis of variance (ANOVA) was used to examine the effect of Kibler scapular type to the CKCST and an analysis of co-variance (ANCOVA) using body mass index (BMI) as a control. All assumptions were met to run the ANCOVA to evaluate the covariate. A prospective design was used to evaluate the reliability via Pearson Correlation Coefficients between student physical therapists and experienced physical therapists in identifying Kibler scapular type as correct or incorrect assessment.
RESULTS
The demographic characteristics of the 61 participants who completed testing (33 males, 28 females; mean age 24.19±2.61) are provided in Table 1. The most common Kibler scapular type was that of a type IV normal scapular position seen in 30 (49%) participants, followed by Type I seen in 20 (33%) of the participants. Two participants were excluded from participation in the study secondary to unidentified high blood pressure that did not resolve after resting five minutes.
Kibler scapular classification and the CKCUEST
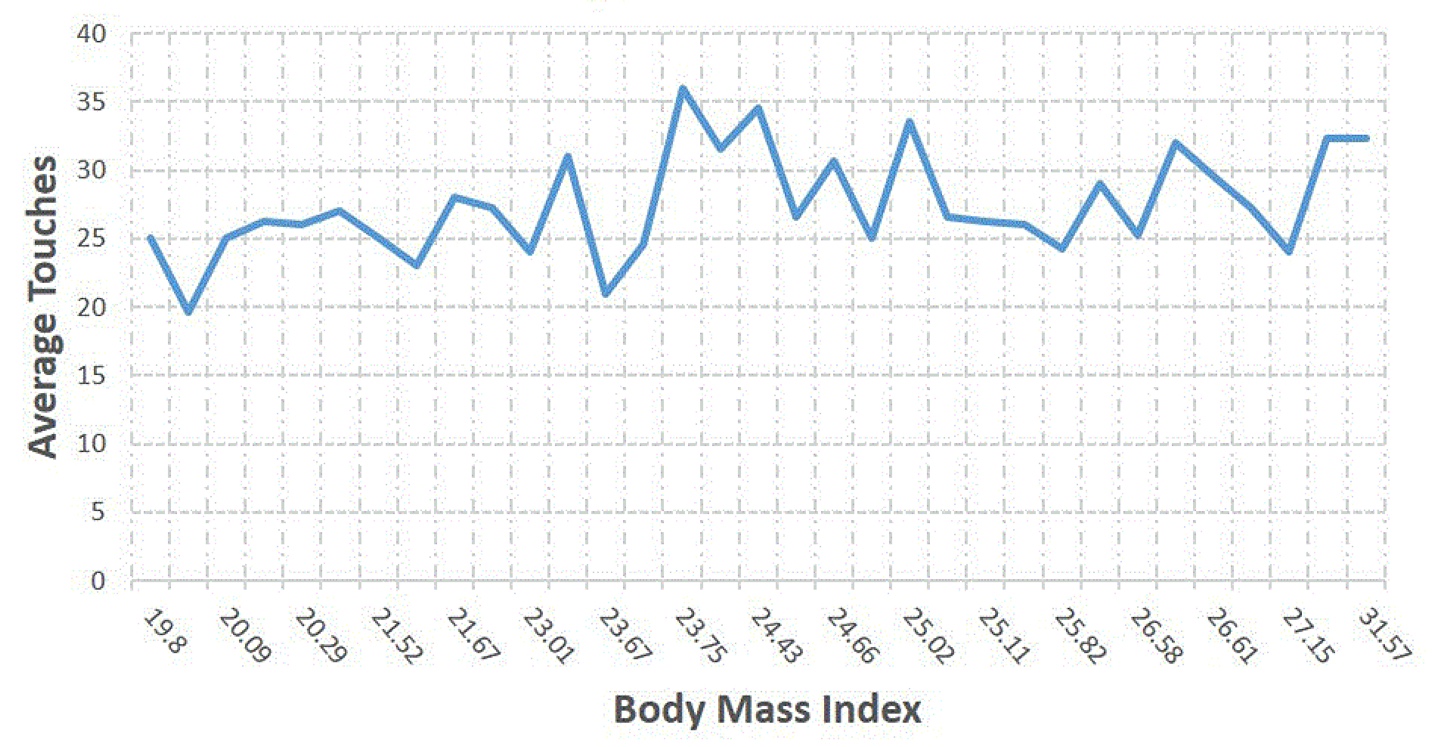
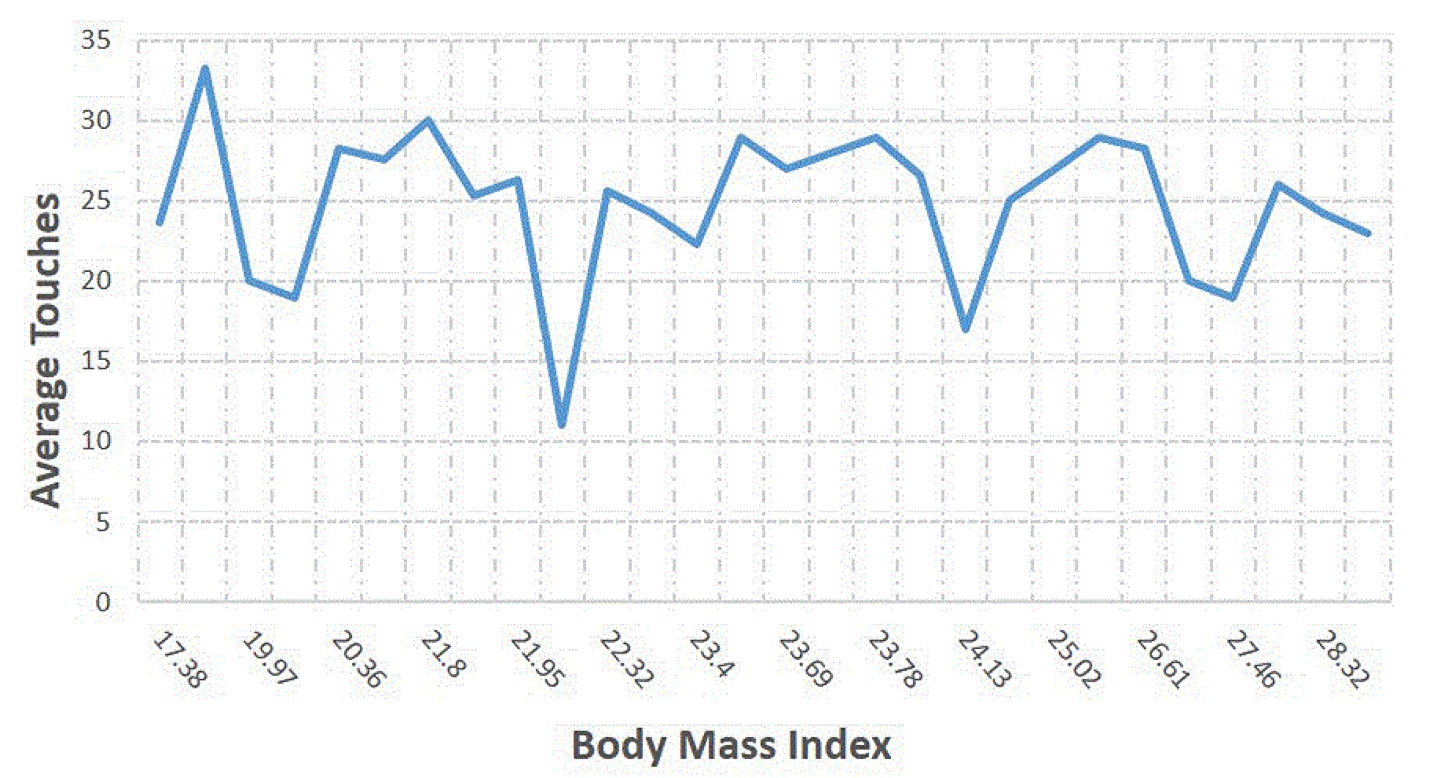
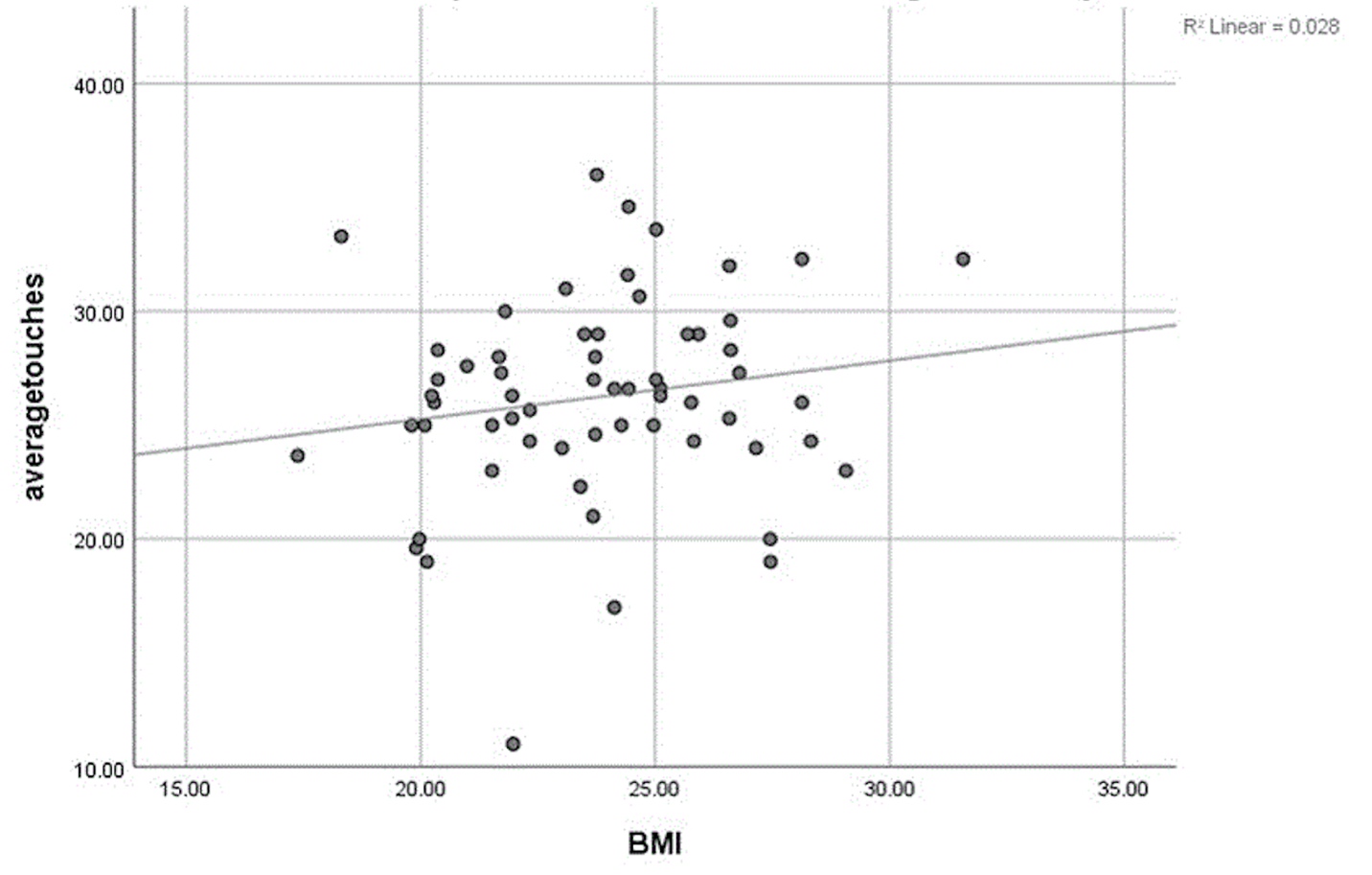
Table 2 provides the means and 95% confidence intervals (CIs) for the average number of touches, normalized and power score for the CKCUEST for all participants. Results of the one way ANOVA showed statistically significant differences between participants with Type I and Type IV Kibler scapular classification for the CKCUEST power score but no differences for the average number of touches or the normalized scores. Results of the ANCOVA, when controlled for the body mass index revealed no significant differences between participants with differing Kibler scapular classifications and the CKCUEST power score (Figures 1, 2, 3). Of note, females that chose the modified push-up position for the CKCUEST accounted for 5% of participants.



Reliability of Scapular classification between the student physical therapist and the experienced physical therapist
Pearson Correlation Coefficients between the student physical therapist and the experienced physical therapist at both locations are presented in Table 3. The inter rater reliability of student physical therapists and experienced physical therapist from both locations was excellent in evaluating the Kibler scapular classification (ICC=.96; 95% CI, 0.92, 0.99).
DISCUSSION
The purpose of this study was to determine if the Kibler scapular classification affects the ability to perform the CKCUEST in healthy participants. The first hypothesis that those with a normal Kibler scapula classification would perform better on the Davies CKCUEST was rejected. The results from the current study show that Kibler scapula position does not affect the ability to perform the CKCUEST in healthy young adults. Identifying Kibler scapular position(s) has been clinically useful to describe static scapular positions but may not reflect functional scapular abilities. Deng et al23 investigated four different positions (at rest and end range of elevation in the sagittal, scapular and coronal planes) and found that 90.8% of patients with shoulder complaints had an abnormal resting scapular position when the patients’ arms were by their side and at rest. Deng et al23 described this as scapular dyskinesia, which the authors of the current study would suggest as incorrect because dyskinesia as a clinical description implies upper extremity motion and instead abnormal resting position was found in a static position, which is not the true resting position of the scapula. Forty-nine percent of healthy participants in the current study had normal or type IV Kibler scapula classifications. None of the healthy participants with type I or type II had any symptoms.
Differences were only identified between those with Type I and Type IV Kibler scapular classification for the CKCUEST power score. Additionally, when controlled for body mass index no significant differences were present between participants with varied Kibler scapular classification types and the CKCUEST power score. Perhaps the lack of association is because it is a comparison of a visual observation of a static scapula position being compared to a dynamic stabilization test of the scapula stabilizers. Another potential reason may be that those with Kibler Type I scapular dyskinesis may represent a “normal asymmetry” in a healthy population. Future studies should include a larger sample size that includes subjects with a variety of Kibler scapular positions.
The interrater reliability of a second year student physical therapist at two separate locations to identify Kibler scapula types was excellent when compared to the experienced physical therapist. This is in contrast to authors who have noted low interrater reliability (k=0.084) in evaluating Kibler scapula classifications of uninjured professional baseball players.6 McClure et al29 investigated 142 uninjured athletes and found satisfactory reliability (k=0.48 to 0.68) with percent agreement ranging between 75% to 82% but they evaluated both a static limbs position and asked participants to go through flexion and coronal plane abduction using a 3 to 5 lb barbell. The current study approach did not include barbells to influence visual observation of Kibler classification. In terms of side-to side comparison, authors have found low interrater reliability for classifying the Kibler scapular position (k=0.264 for left, k=0.157 for right).6,30 The ability of a first year or novice student and an experienced physical therapist to reliably agree on the scapular posture by observation examination is presently unknown. Authors have also reported a limitation of interpretation of scapular position with video analysis.6,30 McClure et al also used video analysis for interpretation and reported coefficients ranging between 0.48 and 0.61 with percentage agreement ranging from 75% to 82% between examiners.29 Tate et al tried to validate the McClure et al study by using 66 of the same 142 participants used in the McClure et al study.31 Tate et al31 used three-dimensional electromagnetic kinematic testing and noted less scapular upward rotation or Type III scapula in the participants that McClure et al29 investigated and classified. Thus, visual observation of scapular position overestimated the three-dimensional electromagnetic kinematic testing or more simply stated what they saw did not correspond to precise measurements of scapular motion. Uhl et al32 categorized symptomatic and asymptomatic athletes into a yes/no method in which those with abnormal scapular dyskinesia were labeled as having dyskinesia and were not specifically categorized by scapular type. They found a sensitivity of 76% and positive predictive value of 74% using the yes/no method.32 Interestingly, they also noted that testing symptomatic patients showed a higher frequency of multiple-plane scapular asymmetries.32 Deng et al23 investigated the Kibler classification system in four different positions but concluded that the resting position of the scapula was the best position to assess in patients with shoulder dysfunction. In the current study, this static resting position of the scapula was reliable between student and experienced clinician but was not associated with CKCUEST performance.
Authors investigating the CKCUEST have suggested that the test has excellent reliability for adolescents,22 for physically active adults,21 sedentary adults, and sedentary adults diagnosed with shoulder impingement syndrome,21 for Division I college athletes,11,26 collegiate basketball athletes,33 for handball athletes,34 and collegiate baseball athletes.10 The majority of these studies have examined test-retest reliability and three of these studies investigated and reported the average number of touches, normalized score, and power score.20,22,28
Use of the power score and normalized score requires further investigation. Goldbeck and Davies12 first described the power score using 68% of the participant’s weight in kilograms based on Dempster’s work.35 The power score considers the weight of the participant by multiplying the average number of touches by 68% of the participant’s weight in kilograms. Tucci et al20,21 used the power score and report that 68% of the participant’s body weight in kilograms corresponds to the weight of the arms, head and trunk. Dempster35 is often cited as the classic paper for considering the mass of body segments but used adult male cadavers between 52 to 83 years of age to derive the 68%. Recently, authors have suggested that using older male cadavers do not correspond to younger adults or appreciate sex differences.36,37 Authors have separated body segment mass by sex and suggest that the mass of the head, trunk, upper arms, forearms, and hands equal 60.28% for males and 58.23% for females of the total mass of the body.37,38 Virmavirta et al36 concluded that inter-individual differences among athlete groups may be large and that the selection of segment body mass for analysis is not clear. Virmavirta et al36 suggest using a precise body segment model specifically for athletes. For example, gymnasts have different segmental body mass compared to throwers or hockey players. Considering that the use of the power score may not be specific enough for athletes, the authors of the current study controlled for BMI for the average number of touches of the CKCUEST and for the power and normalized score and found no statistically significant relationship to Kibler scapular position (Figure 3). The authors of the current study suggest that the use of a power score of 68% should not be used for athletes or for females based on the variability found in the literature on segmental body mass for younger athletes. Instead, a power score of 60.28% should be used for males and 58.23% for females to be precise. This approach should be adopted until sport specific normative data for body segment mass are gathered in a large population of athletes.
The normalized score considers the height of the participant by dividing the number of touches by the height of the participant and has also been questioned. Authors have suggested that the height of the participant, the maturational stage, or anthropometric measurements such as shoulder width place for those with a narrower build creates a performance disadvantage for the CKCUEST.11,28 Callaway et al28 suggest that the original CKCUEST starting position of placement of the hands 36 inches apart is not justified.12 Callaway et al28 suggest that using 36 inches as the starting position is inappropriate for both sexes as taller participants will have a greater advantage over shorter participants which leads them to suggest a different starting position appropriate to the height of the participant.28 Callaway et al28 investigated four different starting positions (36 inches, shoulder breadth, acromial distance, and 50% of the participant’s height) and reported that the starting position at 50% of the participant’s height resulted in the smallest standard error of measurement and minimal detectable change of all three positions. Callaway et al28 only investigated males in their study so it is unknown if performance improves in females using this starting position. Taylor et al11 used shoulder width as the starting position for male and female collegiate athletes as an attempt to adjust for body-size heterogeneity of the athlete. In the current study, the authors offered the participant the choice of starting position to correspond to the shoulder width of the participant. Regarding the normalized score, the authors of the current study suggest more evidence is needed on the use of the normalized score. Specifically, it is important to have normative data on how height affects the starting position and performance of the CKCUEST across all types of athletes. The authors of the current study suggest that since the original paper on the CKCUEST investigated this test as an upper extremity performance test of endurance, three trials of the test should be performed and performance of fewer than three trials alters the purpose of the original test. Maintaining a standardized approach of three trials should be used in the clinic as the original intent of the CKCUEST is related to endurance.
The authors of the current study did exclude two participants secondary to unidentified high blood pressure that precluded them from participation in exercise. The authors of the current study suggest that future studies investigating the CKCUEST should take blood pressure measurements on all participants especially since upper extremity exercise increases systolic blood pressure much more so than lower extremity exercise.39,40 As a precaution, any patient that is unknown to a clinician that performs upper extremity exercise should have their blood pressure measured by their therapist. For example, a per diem physical therapist that is covering a holiday that does not know any of the patients should consider taking blood pressure measurements on unfamiliar patients due to the increase in systolic blood pressure during upper extremity specific exercise.
The authors of the current study identify that experimental studies have limitations. One limitation was that the order of testing was standardized (visual observation of Kibler classification followed by three trials of the CKCUEST) and therefore may not mimic the clinical setting. Another limitation is that the study was done at two separate locations involving healthy participants that self-reported if they had a shoulder injury over the past year or current shoulder pain. As the current study used only healthy participants, findings should be extrapolated with caution to those following rehabilitation for upper extremity injury. It is unknown if the participants had any actual previous shoulder injuries or other musculoskeletal conditions that were not identified.
CONCLUSIONS
Sports physical therapists commonly evaluate patients with upper extremity injury or conditions and observe abnormal scapular position in the affected extremity. In the current study, resting Kibler scapular position did not affect the ability to perform the Davies CKCUEST in healthy young adults. However, the ability to identify Kibler scapular positions was reliable between second year students and experienced physical therapists. The authors suggest future studies should investigate varied starting positions and the use of the power and normalized scores for the CKCUEST.
Conflicts of interest
The authors do not have any conflict of interest to report.