INTRODUCTION
Evidence has shown that dynamic balance is diminished in individuals with chronic low back pain (CLBP)1–3 and in individuals with a history of low back pain (LBP) who are pain-free at the time of testing as compared to asymptomatic controls.2 Individuals with LBP often stiffen their lower back, relying more on ankle movement and less on hip movement to perform dynamic tasks in an upright standing position.3 Once individuals with LBP lose their balance, they have more difficulty regaining it, and these deficits can persist even after an episode of LBP has subsided.2 In addition, individuals with LBP are apprehensive of performing dynamic tasks, primarily due to fear of additional pain and re-injury of their low back.2,4 Therefore, it is not surprising to find that the severity of a dynamic balance deficit is associated with chronicity of LBP.
Dynamic balance is essential for performing daily functional activities (e.g., leaning forward, navigating stairs, walking), work tasks, and recreational activities. Although balance has been evaluated in individuals with LBP using expensive laboratory-based equipment, this laboratory equipment is impractical in clinical settings.5,6 The Y-balance test (YBT) is a portable and inexpensive tool designed to measure dynamic balance. It was developed from the Star Excursion Balance Test (SEBT) to improve the repeatability of reach measurement and standardize performance of the test.7 The YBT evaluates single-leg-balance, dynamic neuromuscular control, proprioception, and strength while an individual reaches with the non-stance limb in three directions.5–7 The YBT has been a reliable measure of dynamic balance in healthy asymptomatic adults, with intraclass correlation coefficients (ICCs) ranging from 0.85 to 0.91 for intra-rater reliability and from 0.85 to 1.00 for inter-rater reliability.7,8 The YBT also has been used in various populations to predict general risk for musculoskeletal conditions and injury recurrence, typically in younger athletic populations.5,7,9 In addition, the YBT has been capable of detecting residual postural control deficits in asymptomatic individuals with a history of LBP.2 Therefore, the YBT may be a promising tool for measuring dynamic postural control of young adults with CLBP.
To date, there has been no consensus regarding the utilization of the YBT for assessing dynamic balance in individuals with LBP. However, two research studies used the YBT to compare dynamic balance performance between individuals with and without LBP.2,10 Hooper et al.2 found that reach distances of the dominant leg were reduced in all directions except the anterior (ANT) direction in adults with LBP and in adults with a history of LBP as compared to asymptomatic controls. Haag et al.10 found no significant differences in the three reach directions for lower extremities between two groups of adolescent female soccer players with and without LBP. However, Haag et al.10 did not consider limb dominance, and Hooper et al.2 assessed the reach distances of the dominant limb only. In both studies, the comparison of YBT performance did not consider the painful side of the participants with LBP.
Literature also has indicated that specific reach directions of the YBT correlate with specific impairments of the lower extremities.11 For example, poor performance in the posterolateral (PL) direction has been reported as a predictor of ankle sprain.11 In addition, composite YBT scores can assess an individual’s ability to perform a multiplanar motion.12 Scores of separate reach directions along with the composite score may be used as different indices of dynamic balance for patients involved in specific types of work or sports activities. To date, there is little evidence to demonstrate the reliability and validity of the YBT when used for assessing dynamic balance in young adults with CLBP. Therefore, this study determined the inter-rater reliability and validity of the YBT in young adults with CLBP. Specifically, the YBT scores of the young adults with CLBP were compared to those of asymptomatic young adults to establish the construct validity of the YBT for this population.
METHODS
Study Design
This study is a cross-sectional reliability and validity study approved by the Institutional Review Board of Texas Woman’s University.
Participants
The sample size was determined based on prior YBT studies,1,2 which showed a large effect size of 1.25 between individuals with LBP and asymptomatic individuals. Using a more conservative approach, an effect size of 1.0 was used to estimate the sample size for this study. A power analysis performed with G*Power version 3.1.9. indicated that at least 24 participants would be needed to ensure an adequate power level of 0.80 for an independent t-test at an alpha level of 0.05. To allow for attrition, 30 participants, 15 in each group, were planned for the study.
Thirty 18- to 40-year-old young adults, 15 individuals with CLBP and 15 age- and gender-matched asymptomatic participants, were recruited and completed the study. Age and gender were matched between groups to reduce the possible influence of these variables on dynamic balance. Asymptomatic participants were individuals who had not experienced LBP within a year before the testing and no known LBP-related injury in their lives. Participants in the CLBP group were individuals who had experienced repeated episodes of persistent or recurrent LBP of musculoskeletal origin for a duration of over 12 weeks and an average pain intensity score ≥ 2/10 on the Numeric Pain Rating Scale (NPRS) in the past week.
Participants were excluded from the study if they reported or demonstrated any of the following: (1) pregnancy, (2) systemic joint disease (e.g., neurological or rheumatologic disorders), (3) serious spinal conditions, such as tumor, infection, or fracture, (4) signs of nerve root compression, (5) a history of hip, knee, or ankle pain in the previous two years, (6) previous surgery to the lower extremity or lumbar spine, (7) a concussion within the previous three months, (8) vestibular or other balance disorders, (9) ongoing treatment for inner ear, sinus, or upper respiratory infection, and (10) a need for any form of walking aid, such as a cane or walker. In addition, participants were excluded were they receiving medical care from a physician or other practitioner at the time of the study. Each participant was informed of the study procedures, benefits, and possible risks and then signed a written informed consent form. Potential participants were screened with a neurological examination (e.g., strength, sensation, and reflexes) performed by one investigator to determine their eligibility for the study.
Instrumentation and outcome measures
The Y-Balance Test Kit (Functional Movement Systems, Inc. Chatham, VA) was utilized for evaluating dynamic balance. This kit consists of a single central stance platform which is connected to three plastic tubes with three moveable reach indicators arranged in the ANT, posteromedial (PM), and PL directions. Each tube is marked at intervals of one centimeter (cm).7,13 The outcome measures of interest were the reach distances of the three directions and the composite score of the YBT.
Examiners
Four investigators, all doctoral-level physical therapy (PT) students, administered the YBT test in this study. Before commencing the study, these four investigators completed three hours of training in the YBT protocol given by the principal investigator (YA), who had attended a YBT online course and was certified in performing the YBT. Each participant was assessed by two of the four investigators based on the availability of the investigators; however, the same two investigators took measurements from each participant for the testing sessions. To examine inter-rater reliability, the YBT scores for participants in the CLBP group were independently determined and recorded to the nearest cm by two investigators.
Procedures
Once a participant was determined to be eligible for the study, the participant was asked to complete an intake form, including questions asking their age, gender, limb dominance, level of physical activity (minutes per week), and past surgical and medical history. Participants with CLBP also were asked questions related to their pain location and duration. In addition, they were asked to rate their average pain levels in the past week using the NPRS, their disability level using the modified Oswestry LBP Disability Questionnaire (OSW), and their fear-avoidance level using the Fear-Avoidance Beliefs Questionnaire (FABQ). The NPRS, OSW, and FABQ have been reliable and valid tools for assessing LBP-related pain intensity, perceived disability, and fear-avoidance beliefs, respectively.14–18 Last, the height (cm), body weight (kg) and leg length (LL) were collected from all participants. Because LL has been shown to be a factor in affecting YBT performance, LL was used to normalize reach distances.19 The LL was measured from the inferior tip of the anterior-superior iliac spine to the distal border of the ipsilateral medial malleolus with the hips and ankles in a neutral position while the participant was in a supine position.7 LL was measured two times for each participant, and the average of the two measurements was used for data analysis.
Next, the participants were instructed in the proper performance of the YBT following the procedures described by Plisky et al.7 The lower limb being tested was defined as the stance limb, and the reaching direction was defined based on the orientation of the stance limb.9 For the asymptomatic group, the dominant leg was determined by the participant’s self-reported preferred leg used for kicking a ball.20 For participants with unilateral LBP, the painful side was designated as the involved side. For participants with bilateral LBP, the most painful side was designated as the involved side. If both sides were equally painful, the dominant leg was designated as the involved side.
Participants performed the YBT barefoot to eliminate potential effects of varying footwear.9 In addition, each participant performed six practice trials in each direction on each leg before taking measurements of reach distances. A break was given when the participant requested during the practice trials. These practice trials were performed to minimize the learning effect, as performance on the YBT has been shown to reach a plateau after six practice attempts.21 During the YBT, the participants were instructed to maintain single-leg stance on the center foot-plate with the foot behind the marked starting line. Next, the participants used the foot of their non-stance leg to slide the reach indicator along the designated tube as far as possible and then returned their foot to the starting position while maintaining their balance.
Participants could use their arms for balance or for safety, if necessary. After the practice trials, each participant performed three trials used for data analysis. However, the trial was discarded and retried if the participant did any of the following: (1) moved the foot of the stance leg from the platform or crossed the marked line, (2) pushed, kicked, or stepped on the reach indicator, (3) touched the floor with the foot of the non-stance leg, or (4) lost balance before returning the foot of the non-stance leg to the starting position. To reduce fatigue, participants were given a rest of at least 10 seconds between each trial, and at least 30 seconds between each reach direction.22 In addition, the testing order of the reaching directions and the testing order of the limbs were randomized.2 The successful reach distance was measured by reading the demarcated line at the proximal edge of the reach indicator closest to the participant to the nearest cm.
For each direction, the reach distances collected from the three trials were averaged and then normalized to leg length, using the following formula: (reach distance/LL) x 100%.7,23 The YBT scores were collected from the dominant leg of asymptomatic participants and the involved side of participants with CLBP. To determine the inter-rater reliability, two investigators, including the investigator who provided the instructions, took turns and independently recorded the participant’s reach distances. Considering that pain, aggravation, and fatigue could occur with repeated testing of the YBT on the participants with CLBP, only one session of the YBT was administered for inter-rater reliability.
Data Analysis
SPSS Statistics, Version 25 (IBM Corp., Armonk, NY, USA) was used to perform statistical analysis. Descriptive statistics, including means, standard deviations, frequencies, and percentages, were used to describe the demographics for both groups, as well as pain duration, the NPRS score, the OSW score, and the FABQ score for the CLBP group. In addition, independent t-tests or chi-square tests were performed to compare differences in the demographic data between groups, such as age, gender, body mass index (weight (kg) ÷ height2 (m)), and physical activity level.
Intraclass correlation coefficients (ICC2,k) were calculated to determine the inter-rater reliability of the composite score and the normalized reach distances of the three reach directions for the CLBP group. Next, paired t-tests were used to compare the differences in the three normalized reach distances and the composite score between limbs in asymptomatic participants. If there were no differences between limbs, the YBT scores of the dominant leg were used for between-group comparisons. To assess construct validity using the known-groups method, independent t-tests were performed to examine between-group differences in the three reach distances and the composite score of the YBT. The alpha was set at 0.05 for all statistical analyses. Lastly, effect sizes were calculated for the group comparisons using Cohen’s formula: 24
RESULTS
Fifteen asymptomatic controls and 15 participants with CLBP with similar age- and gender-matched (9 women and 6 men in each groups) completed the study. A summary of participants’ characteristics for both groups is presented in Table 1. Independent t-tests showed that there were no statistically significant differences between the CLBP group and the asymptomatic group in age (p = 0.943), BMI (p = 0.282), and physical activity levels (p = 0.165). The participants with CLBP had an average NPRS score of 4.5 and an average OSW score of 16.8, indicating that the CLBP group had relatively moderate pain levels and low disability levels. For inter-rater reliability, the results showed that the YBT had excellent inter-rater reliability for the ANT (ICC = 0.99; 95% CI: 0.99–1.0), PM (ICC = 1.0; 95% CI: 1.0), and PL (ICC = 1.0; 95% CI: 0.99–1.0) reaches and the composite score (ICC = 1.0; 95% CI: 1.0).
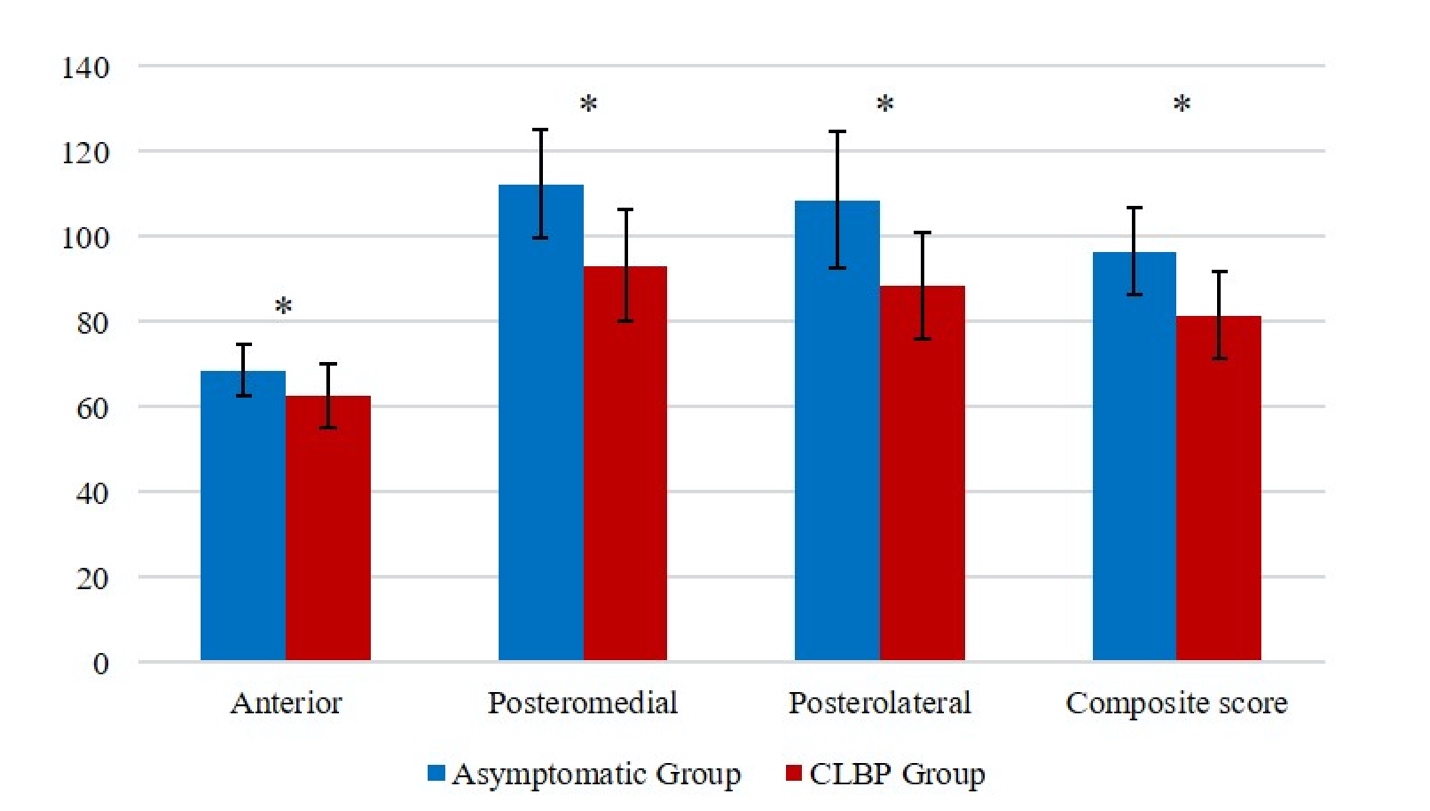
Table 2 displays the YBT scores for both groups. Because there were no significant differences in the YBT scores between the dominant and non-dominant limbs of the asymptomatic participants, the YBT scores of the dominant leg of asymptomatic participants were compared to those of the involved side with CLBP. The results of four independent t-tests showed that the CLBP group had a significantly lower composite score (p < 0.001) and shorter reach distances in the ANT direction (p = 0.023), PM (p < 0.001), and PL (p = 0.001) directions than the asymptomatic group (Figure 1, Table 3).
_for_the_asymptomatic_group_(.jpeg)
DISCUSSION
The results of our study showed excellent inter-rater reliability for the ANT, PM, and PL reaches and the composite score for the CLBP group, indicating that the YBT can be used by different testers to reliably assess dynamic balance in those with CLBP. Our reliability results follow reported work by Plisky et al.,7 who also demonstrated excellent reliability (ICC = 0.99-1.00) of the YBT for assessing dynamic balance in asymptomatic active young adults between 18 and 35 years old. Using two raters to observe each trial and score it independently may have contributed to the reliability shown in both studies. However, Plisky et al.7 used two experienced raters with at least seven years of clinical experience, whereas novice raters scored the YBT in this current study. Shaffer et al.8 also showed good inter-rater reliability (ICC = 0.85-0.93) when raters with limited experience used the YBT to assess dynamic balance in active duty service members. The slightly lower ICC values in the Shaffer et al. study could be in part due to the collection of their data by seven raters and on separate days.8 The YBT can reliably assess dynamic balance with both novice and experienced raters.
The results of our study also showed that the CLBP group demonstrated significantly lower YBT scores in all three reach distances and the composite scores, indicating that the YBT can be used to distinguish the CLBP groups from asymptomatic healthy controls. Similar to our study results, Ganesh et al.1 also found that individuals with CLBP had significantly reduced ANT, PM and PL reach distances of the SEBT as compared to healthy controls. The results of Ganesh et al.1 study and the present study may demonstrate an impairment in functional activities for those with CLBP. Therefore, restoring dynamic balance should be considered in the management of CLBP. Pain-related fear avoidance of movement could have contributed to the reduction of the YBT performance. However, CLBP group had a very low OSW and FABQ scores. Therefore, it is unlikely that fear avoidance of movement could have impacted the results.
Hooper et al.2 found significantly reduced PM and PL reach distances of the YBT in the CLBP group as compared to those of asymptomatic controls, but there was not a significant difference in the ANT reach distance. Hooper et al.2 speculated that the impairments of their participants could be less severe because their criteria for inclusion in the CLBP group was noticeably different from that of the Ganesh et al.1 study. The individuals with CLBP in the Hooper et al. 2 study were those with current LBP and a history of LBP over the previous 18 months, whereas the participants had LBP for more than 6 months in the Ganesh et al.1 study. Considering that the participants with CLBP in this current study had pain for an average of 57 months, they could have had more severe impairments (e.g., strength loss and deconditioning) than those in the Hooper et al.2 study, resulting in decreased ANT reach distance. In addition, hip extension range of motion (ROM) is required to perform the ANT reach. Therefore, decreased hip extension mobility could have affected the ANT reach distance, as hip extension was found to be reduced in the individuals with CLBP,25 but not in those without LBP.26 However, hip ROMs were not measured in this current study to confirm this hypothesis.
On the contrary, Haag et al.10 reported that the YBT reach distances for those with LBP were not different from healthy controls. The difference in findings of the two studies could be attributed to differences in the age of the participants. The participants in the Haag et al.10 study were adolescents (15.9 ± 0.9 years of age), who have been shown to have better YBT performance than adults.27 The adolescents with LBP may have a greater hip range of motion, thus allowing them to compensate for reduced low back mobility while performing the YBT.28 In addition, the pain in Haag et al.'s LBP group was less severe and less chronic, thus further contributing to the lack of difference in the YBT performance between the LBP group and health controls, as literature has shown that adolescents with higher intensity of LBP demonstrate reduced ability to perform a single-leg-stance balance task.29
Limitations
One limitation of this study is the use of convenience sampling. In addition, the participants in this current study were young adults only; therefore, these participants may not have been representative of the general population with regard to age. Furthermore, although efforts were made to control the potential influence of confounding factors that may affect YBT performance, factors such as hip, knee, and ankle strength and joint ROM were not measured. Future studies should examine the impact of these factors on the reduced YBT performance in patients with CLBP.
CONCLUSION
The results of this study indicate that the YBT demonstrated excellent inter-rater reliability, and that young adults with CLBP had impaired dynamic balance as compared to young asymptomatic adults. The YBT may be a useful tool for clinicians to assess dynamic balance deficits in patients with CLBP. Our study adds to the existing body of literature by showing that the involved side of participants with CLBP may influence YBT scores , as the participants with CLBP in this current study scored lower than the asymptomatic group on both the YBT reach distances and the composite score for the YBT. However, further investigation is warranted in order to ascertain the effect of the involved side on dynamic balance performance as related to functional daily activity or sport tasks of LBP populations.
Disclosure Statement
No conflicts of interest were present in this study.
Acknowledgements
The authors would like to thank Abby Smith, Emily Groff, Jessica Britain, and Michael Aqrabawi for their contribution to data collection.