BACKGROUND AND PURPOSE
Netball is a predominantly female team sport with millions of players across 117 countries.1 Netball evolved from women’s basketball in the 1890s, was first played in England in 1895, and later became popular across the British Commonwealth.2 In England in 2017, there were 180,200 adult netball players3 which increased to 321,200 players by 2019.4 In 2018, there were 486,618 registered netball players in Australia5 and 145,000 registered players in New Zealand.6 In the United States (US), netball is a relatively new sport which gained popularity in the 1980s.7 Recently, Miami hosted the World University Netball Championships in 20168 and the US Open Netball Championships attracted over 100,000 viewers in 2017.7 Now, Netball America has members in 33 states7 and a new high-performance development pathway exists following the success of the US University Netball Team.9 Community-level netball participation in America is expected to grow following netball’s countrywide introduction to schools and community centers and tournaments at venues such as Madison Square Garden.7 With increased sport participation comes an increase in injury frequency.10–1212 Because of growing participation in netball in America, it is prudent for sports physical therapists to become familiar with the nature of the game and to consider primary injury control interventions with community-level players.
Netball is a court-based team game played over 15-minute quarters.13 Netball is played on indoor and outdoor courts and requires rapid acceleration, deceleration, and change-of-direction running along with jumping, leaping, and ball throwing/catching when attempting to score a goal in the opponent’s territory.13–15 A unique characteristic of netball is the ‘footwork rule’ which restricts players to a one-step landing after catching the ball.13 In other words, after touching down with one foot, players can only take one more step with the other foot to decelerate the body; after this, players may pivot on the touchdown foot before passing the ball to a teammate.13 The requirement to obey the footwork rule and stop suddenly with one step results in frequent single-leg landing (SLL) with vertical ground reaction force (VGRF) ranging from 3.516 to 5.717 times bodyweight (BW). The VGRF is of interest because it contributes to shear, compression, and rotation forces experienced by the lower-limb joints18,19 and because SLL and double-leg landing (DLL) are involved in 27.1-73.8% of injury events.20–23
Knee injuries account for substantial proportions of netball lower-limb injuries.21,22,24,25 Across studies, the majority of netball knee injuries are of a noncontact nature20,21,23,26,27 (Table 1). Trauma accounts for 26% of knee injuries referred to the emergency room26 and approximately one-third of netball-related hospitalizations.28 Anterior cruciate ligament (ACL) and meniscus tears occur in netball with a respective frequency of 17.2-22.4% and 4.5-32.7%.24,26 When comparing netball to basketball, female ACL sprains and meniscus tears demonstrate higher proportions in netball (17.2%, 4.5%) than basketball (11.1%, 4.1%).24 Considering ACL-reconstruction (ACLR) incidence between sports, a higher rate of ACLR is also evident in netball (188/100,000 participants) than basketball (109/100,000 participants).29 Anterior cruciate ligament and meniscus injuries result in profound consequences such as physical disability,28,30 substantial healthcare costs,29–32 disrupted academic studies,33,34 premature retirement from netball,35 post-trauma osteoarthritis,36,37 and depression.38,39 Risk of suicide can also exist after sports injuries.40,41 Because of such consequences, interventions are needed to mitigate the burden of knee ligament injury for players, teams, and society, and prolong players’ safe netball participation across the lifespan.
The purpose of this clinical commentary is to demonstrate how theoretical principles, different types of research, and different levels of evidence underpin a rational clinical reasoning process for developing noncontact knee ligament injury prevention screening procedures in netball. An understanding of theoretical principles that support clinical practice is critical for designing evaluation and treatment interventions, deploying such interventions in the correct clinical context at the right time, and setting clinicians’ and athletes’ expectations appropriately relative to desired outcomes. This commentary will discuss how theoretical principles and different levels of evidence42 can be translated to and applied within sports physical therapy practice for primary prevention screening for noncontact knee ligament injury in community-level netball. Several paradigms will illustrate the implications of selected theoretical principles for such practice, including stages of injury control,43–45 sequence of prevention,46–49 principles of screening in injury prevention,50 multifactorial model of injury etiology,51 complex systems theory,52 and systems science.53,54 This commentary is original because no similar work exists in the netball literature. Sports physical therapists will find this commentary useful as an example for how to undertake clinical reasoning processes that justify the content of screening procedures contributing to noncontact knee ligament injury prevention in community-level netball.
DESCRIPTION OF THEORETICAL PRINCIPLES
Stages of Injury Control
Injury control refers to preventing or reducing the severity of injury43,45 and includes prevention, acute care, and rehabilitation phases of healthcare.44,45 Injury prevention refers to primary prevention of injury; that is, prevention of first-time injury to a bodypart.46,55 Injury prevention includes all countermeasures to eliminate or minimize the occurrence of injury.43,46 Injury prevention, therefore, does not refer to literal prevention of all injury cases but the prevention of as many cases as possible.43,46,55 Injury prevention seeks to reduce the probability of sustaining an injury rather than to achieve certainty that all cases can be averted.44,46,56 For the sports physical therapist, practice which recognizes prevention of all noncontact knee ligament injuries across time is not possible relative to probability theory (the likelihood that one event will occur given all possible outcomes)57,58 facilitates action from a place of scientifically-informed realistic intention and good conscience.59
Sequence of Prevention
Injury prevention includes evaluation and intervention procedures that combine to decrease the probability for and incidence of injury.44,46 The “sequence of prevention” refers to a process intended to culminate in such outcomes.49 The process includes four steps: 1. establish the incidence and severity of injury (epidemiology); 2. establish the factors contributing to and mechanisms of injury; 3. introduce prevention countermeasures (interventions); 4. assess intervention effectiveness by repeating step one.49 This process has been elaborated upon by other researchers,48 and correspond to long-standing public health disease prevention models.44,46 This commentary addressed step one (above) by establishing the frequency of ACL injury and ACLR in netball. This commentary addresses step two (below) by considering noncontact knee ligament injury mechanisms (i.e. mechanics of injury) and the factors associated with them (i.e. etiology of injury). The implication is that when a thorough undertaking of step two has occurred the sports physical therapist can consider appropriate evaluation (screening) procedures that, in turn, inform the content of step three and its interventions.44,46
Principles of Screening in Injury Prevention
In medicine, screening is a process to identify the presence or absence of disease.60 In sports medicine, the analogy is screening as a process to identify the presence or absence of injury.50 In injury prevention, the intent is to intervene before an injury occurs rather than diagnose an existing injury.50 Screening in injury prevention, therefore, is a process to identify characteristics (factors) that increase athletes’ probability of sustaining an injury.50 These characteristics are then termed ‘risk factors’.51,58 Risk factors are intrinsic (inside) and extrinsic (outside) to the player.46,49,61 In netball, examples of intrinsic and extrinsic risk factors for noncontact knee ligament injury appear in Table 2. Risk factors are also modifiable and nonmodifiable (Table 2).62 Modifiable risk factors (e.g. muscle strength) and nonmodifiable risk factors (e.g. age) can and cannot be altered with conservative interventions, respectively.62 For the sports physical therapist, the implication of intrinsic/extrinsic and modifiable/nonmodifiable risk factors is that the type and number of risk factors included in a screening test battery requires careful consideration. This consideration ensures the most clinically-amenable risk factors are evaluated and screening procedures are performed time-efficiently.
Multifactorial Model of Injury Etiology
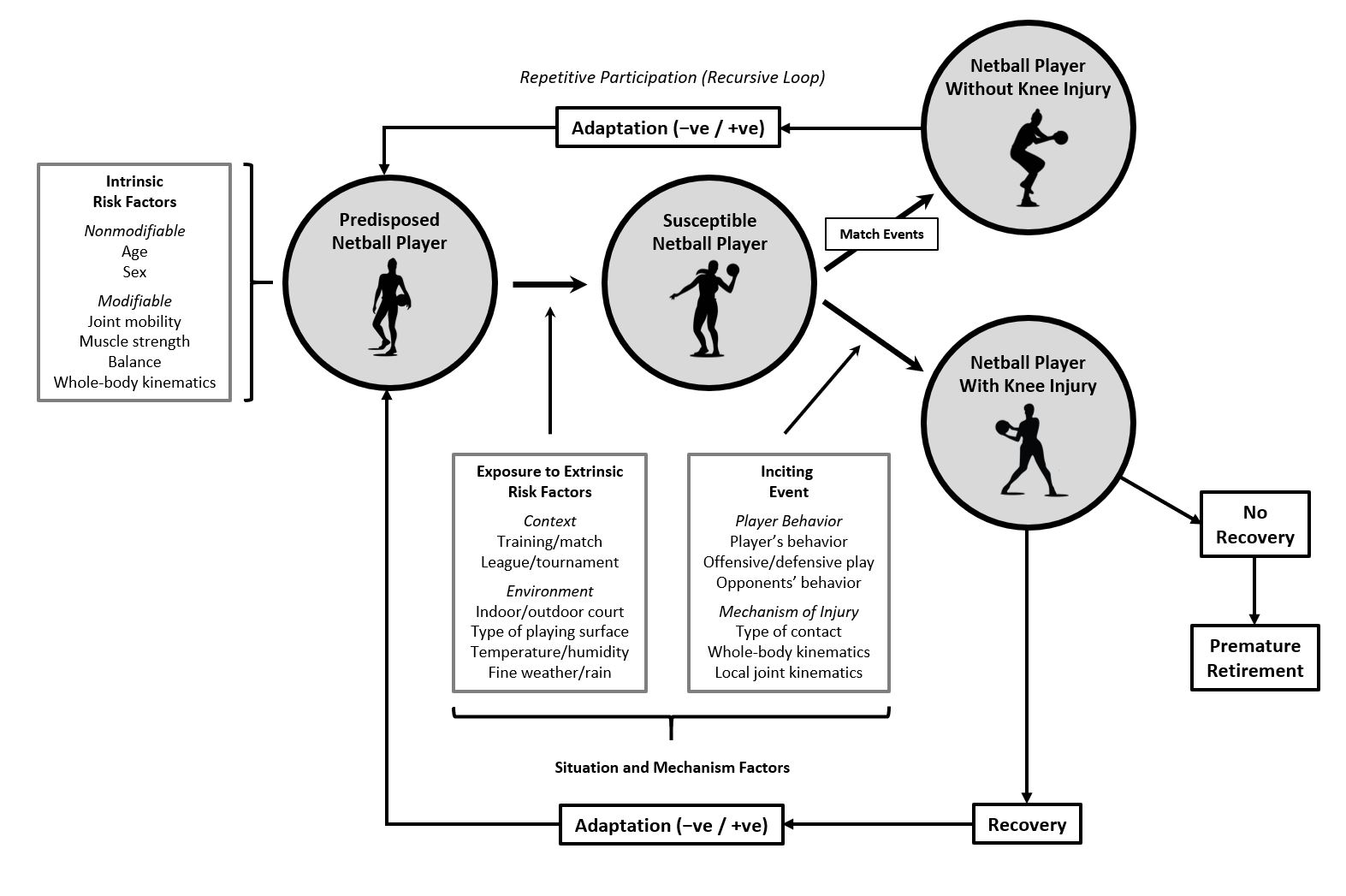
Because the probability of sustaining an injury is influenced by a combination of intrinsic and extrinsic risk factors, the etiology (cause) of injury is multifactorial.51,63 A combination of intrinsic (‘predisposing’) risk factors can sensitize a player to injury,51,64 while a combination of extrinsic (‘necessary’) risk factors must be present for an injury to occur.51,64 Therefore, the temporal relationship of risk factors is critical: some combination of intrinsic and extrinsic risk factors must exist before an injury event can happen (Figure 1).51,64 When a combination of factors produces an injury event within a specific situation, the factors are termed a “sufficient cause”.51,63,64 Screening to determine the presence/absence of intrinsic risk factors, therefore, relates to identifying an athlete predisposed to injury (“predisposed athlete”)51,65,66 (Figure 1). When a predisposed athlete enters a situation containing extrinsic risk factors, the athlete becomes susceptible to injury (“susceptible athlete”)51,65,66 (Figure 1). When the intrinsic and extrinsic risk factors interact within a specific situation as a sufficient cause, an injury event manifests (Figure 1).50,63,65,67 Therefore, for the sports physical therapist in netball, injury prevention screening is about identifying the predisposed player possessing intrinsic risk factors for noncontact knee ligament injury before entering a competitive environment (e.g. outdoor court), context (e.g. league match), or situation (e.g. offensive play).

Complex Systems Theory
A complex system is a collection of interacting components where the behavior of the whole system cannot be predicted with 100% accuracy from the behavior (status) of one component alone.52,68,69 Given the human body is composed of multiple systems (e.g. skeletal, muscular, nervous, etc.) where each system itself is composed of many parts, an athlete is, by definition, a complex system. A netball player’s physiological (e.g. hydration levels, glycogen levels), physical (e.g. joint range-of-motion [ROM], muscle strength), and psychoemotional (e.g. stress, anxiety) status can change between matches, across the season, and across the off-season. A netball match’s environment (e.g. outdoor vs. indoor court) and context (e.g. annual league vs. weekend tournament) can alter from week-to-week. A netball player, therefore, competes within repeating (recursive) loops that span different units of time (e.g. match-to-match, season duration, off-season duration) where sets of risk factors can alter/adapt within and between units of time (Figure 1).52,65 As such, multiple interacting risk factors form a complex “web of determinants” that shift the probability for injury up-and-down across time.46,51,52,65,70 Given probability theory57,58 and complex systems theory,52,68–71 injury prevention screening is not contextual to predicting which specific player will get injured.46,50 Injury prevention screening is instead contextual to identifying athletes with combinations (patterns) of risk factors that contribute to an increased probability for injury.46,50 For the sports physical therapist, noncontact knee ligament injury prevention screening should aim to identify patterns of modifiable intrinsic risk factors (multifactorial ‘risk profile’52) for one point-in-time. Screening is then repeated (serial screening) at appropriate timepoints across a season/year to reveal changes in a player’s risk profile.50
Systems Science
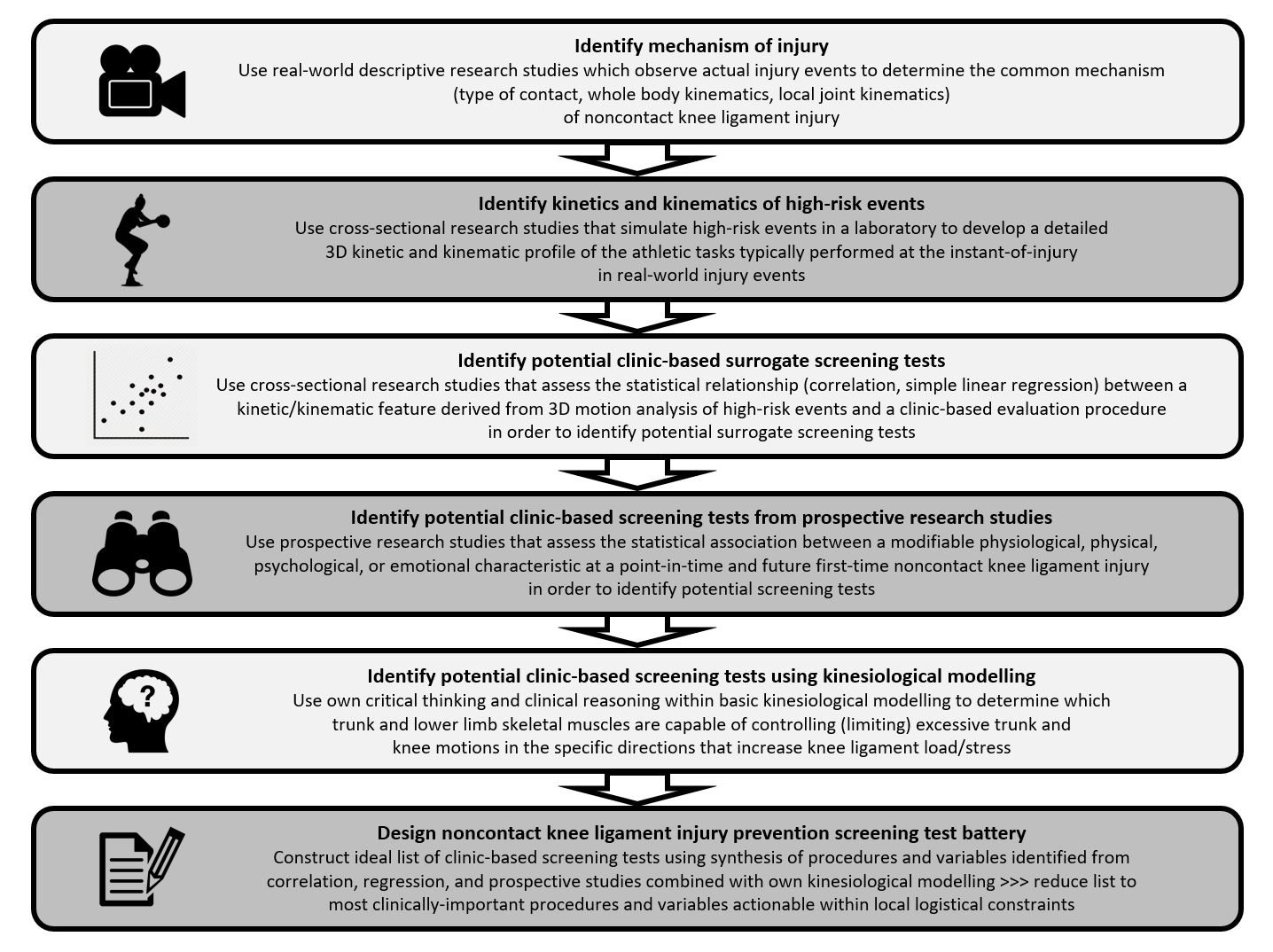
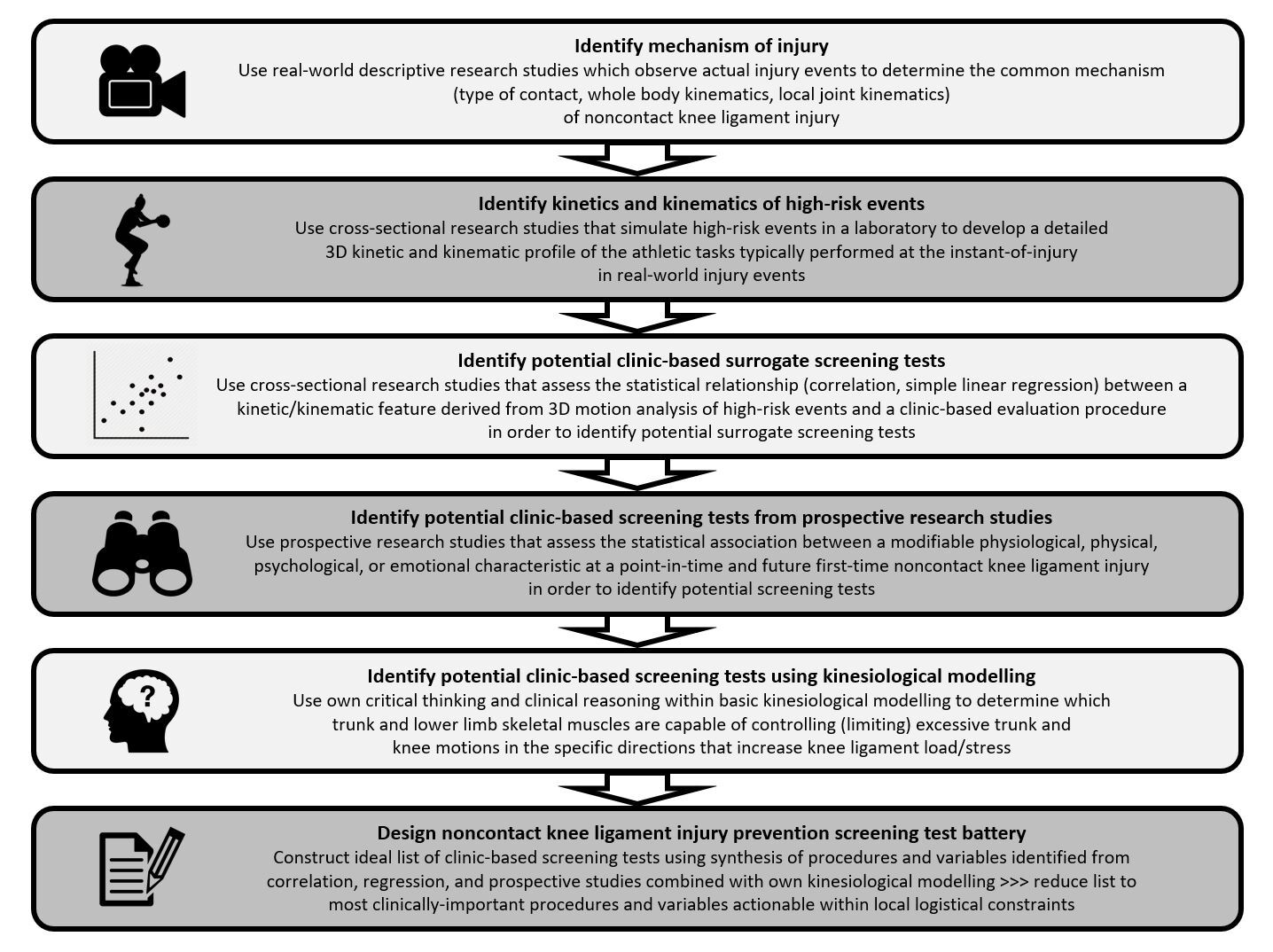
Systems science refers to viewing a clinical problem-space as a system of interconnected, interacting components.54,69,72 Systems science is a foundation for complex systems theory which, in turn, informs the design of complex clinical interventions.73 A fundamental principle in systems science is the use of different types of research to develop clinical interventions.54,69,72 In sports physical therapy, an example of a systems science approach to problem-solving is using different levels of evidence42 (e.g. prospective research + cross-sectional research + individual opinion) in clinical reasoning processes. The integration of different types of research in a clinician’s reasoning yields a richer understanding of a problem-space than when one kind of research is considered alone.54,69,72 In this commentary, descriptive58 (injury mechanisms) and analytic-observational58 (cross-sectional, prospective) in vivo and in vitro human research studies are combined with basic kinesiological modelling to develop rational screening procedures contributing to noncontact knee ligament injury prevention in netball (Figure 2).
Mechanism of Noncontact Knee Ligament Injury in Netball
Knowledge of the mechanism of knee injury gives insight into a player’s movement patterns at the instant-of-injury and the anatomical structures that are damaged. This knowledge contributes to step two of the sequence of prevention.49 Descriptive studies report small proportions (4.5-18.7%) of netball injuries occur during sudden stops when running or cutting to change direction21,25,27 with larger proportions (27.0-73.8%) occurring during landings.20,21,23,25 Other descriptive work reports 38-50% of knee injuries,25,26 81.3% of ACL injuries,27 and 100% of medial collateral ligament (MCL) injuries25 occurred during landings. Specifically, of all landing ACL injuries, 53.8% occurred during SLLs and 46.2% occurred during DLLs.27 Of all netball knee injuries, 24-29% followed contact with another player,20,21,23 although such injuries were not subdivided into direct or indirect contact74 (Table 1). One group performed detailed video analyses of netball ACL injuries and reported 50% followed indirect contact when airborne and contesting for the ball and 50% were noncontact when landing from receiving a mid-air pass.27 Together, descriptive studies indicate the majority of netball knee injuries are noncontact.20,21,23,25–27
Concerning whole-body kinematics when landing, support-leg trunk ipsilateral lateral flexion coupled with knee abduction was observed in 83.3% of netball noncontact ACL injuries.27 Frontal plane trunk motion relative to the knee is of interest because it can increase support-leg knee abduction forces.75 Because whole-body kinematics occur over a support-leg (i.e. weight-bearing leg), knee abduction motions are coupled with hip adduction and internal rotation (IR), knee flexion and IR, and foot pronation.27,76 The coupled trunk, hip, knee, and foot motions are termed a “valgus collapse”76 where knee valgus is synonymous with knee abduction. Concerning local knee joint kinematics, human cadaver (in vitro) research is useful for gaining insight into how joint kinematics influence ligament loads. Anterior tibial displacement (ATD), abduction, and IR generate ACL load/stress and elongation/strain.77–79 When such uniplanar motions are superimposed on each other to elicit a combined motion pattern of ATD + abduction + IR, ACL stress and strain increase exponentially.77–79 Because of the abduction component, the pattern also generates MCL stress and strain.79,80 Knee multiplanar combined motions such as those just described have been observed in 83.3% of netball noncontact knee injuries.27 When the mechanism of noncontact knee ligament injury is understood, the sports physical therapist can devise injury prevention screening procedures that identify which players may be predisposed to landings with kinematic patterns linked to injury-inducing events.
Biomechanics of Netball Landings and High-Risk Events
After knowledge of the mechanism of noncontact knee ligament injury is gained from descriptive studies, cross-sectional laboratory-based studies are employed to acquire a deeper understanding of the biomechanics of athletic tasks linked to the injury-inducing events (Figure 2). Specifically, laboratory-based studies are useful for developing a detailed kinetic and kinematic profile of athletic tasks associated with the mechanism of noncontact knee ligament injury. This profile then facilitates a deeper understanding of why such athletic tasks are ‘high-risk’ events that contain the potential for injury and further contributes to step two of the sequence of prevention.49 Because the majority of knee injuries occur during landings,25–27 focus will now be on the kinetics and kinematics of netball landings as high-risk events using variables popular in the netball literature.
The peak VGRF is of interest because it represents a foot-ground impact force that contributes to compression/shear/rotation forces experienced by the knee joint.18,19 For DLLs after catching a pass, VGRFs were 5.7BW.16 For SLLs with and without catching a pass, VGRFs were 3.5-5.7BW16,17 and 3.4BW,81 respectively. The time-to-peak VGRF (TTPVGRF) is of interest because short TTPVGRFs correspond to higher rate-of-loading of skeletal tissues82 and a significant challenge for the neuromuscular system relative to attenuating potentially harmful forces away from bone/cartilage/ligament tissue.82,83 In DLLs after catching a pass, TTPVGRFs were 48.8ms.16 In SLLs with and without catching a pass, TTPVGRFs were 30.6-42.1ms16,17 and 43.7ms, 81 respectively.
The peak braking force (BF) refers to horizontal ground reaction forces (HGRFs) which push players posteriorly when landing with anteriorly-directed momentum.84 The BF is of interest for the same reason as the VGRF and because it provides additional insight into potentially harmful tissue loading factors.17,82,85 For DLLs after catching a pass, BFs were 1.7BW.16 For SLLs after catching a pass, BFs were 1.4-3.3BW.16,17 The time-to-peak BF (TTPBF) is of interest for the same reason as the TTPVGRF. In DLLs after catching a pass, TTPBFs were 44.3ms.16 In SLLs after catching a pass, TTPBFs were 23.9-44.7ms.16,17
External and internal moments come from outside (e.g. VGRF) and inside (e.g. muscles) the body, respectively, and tend to cause joint rotation.18,19 Peak external moments are of interest because they estimate the tensile forces experienced by ligaments.19,86 In biomechanical modelling, external and internal moments balance each other and are equal and opposite in direction.18,19 Studies which only report knee internal moments of a specific size can, therefore, assume the knee experienced external moments of the same magnitude. For DLLs without catching a pass, knee internal adduction moments (opposing knee external abduction moments) were 0.38Nm/kg.87 For SLLs after catching a pass, knee internal adduction moments (opposing knee external abduction moments) were near 0.40Nm/kg.85
Frontal plane peak knee abduction angles are of interest because higher angles result in higher ACL and MCL stress/strain.77–80 As ligament strain increases with higher abduction angles, the point of ligament damage gets closer.88 For DLLs with and without catching a pass, knee abduction angles were 8.6°89 and 12.1°,87 respectively. For SLLs after catching a pass, knee abduction angles were 5.2°.89
Sagittal plane lower-limb joint displacement is of interest because small displacements are linked to ‘stiff’ landings and large displacements are linked to ‘soft’ landings.90–92 As for short TTPVGRFs, stiff landings are associated with higher tissue peak loads and rate-of-loading than soft landings.90,91,93 In DLLs without catching a pass, knee flexion at initial contact (IC) was 21.1° and at peak flexion was 85.2°, giving a mean displacement of 64.1°.87 In SLLs after catching a pass, knee flexion at IC was near 15° and at 50% of stance phase was near 60°.85 In other SLLs after catching a pass, knee flexion at IC was 16.3° and at peak flexion was 60.3°, giving a mean displacement of 44.1°.89
When the kinetic and kinematic profile of netball landings is familiar, ‘high-risk’ events that contain the potential for excessive loading of knee ligaments and injury can be better identified and understood. Decreased lower-limb flexion displacement during landing is related to increased VGRFs,94–96 increased knee abduction moments,94,96 and increased ACL tensile loads.93 Increased VGRFs are related to increased knee anterior shear forces.97,98 Increased knee external abduction moments are related to increased ACL and MCL loads.77–79 Higher rates-of-loading of the knee ligaments are more likely to cause tissue failure than lower rates-of-loading.99,100 Thus, netball DLLs and SLLs contain high-risk biomechanical features that contain the potential for noncontact ACL and MCL injury.
Developing Noncontact Knee Ligament Injury Prevention Screening Procedures
Having combined real-world observation of noncontact knee injury mechanisms (descriptive research) with laboratory-based study of landing tasks that simulate high-risk events (cross-sectional research), specific screening procedures can be considered relative to selected biomechanical features that contain the potential for noncontact knee ligament injury (Figure 2). The injury-inducing events and high-risk tasks discussed above require sophisticated equipment (e.g. 3D motion analysis) to determine kinetic/kinematic features (e.g. external abduction moment). Because such equipment is not typically available to community-based sports physical therapists, clinic-based ‘surrogate’ procedures related to 3D kinetic/kinematic features are required. Surrogate procedures are chosen using cross-sectional studies employing correlation or simple linear regression designs (Figure 2). Prospective studies reporting associations between intrinsic risk factors and future injury are also used to identify potential screening procedures (Figure 2). Alongside cross-sectional and prospective research, clinicians’ opinions (i.e. critical thinking101 + clinical reasoning102) derived using basic kinesiological modelling103,104 (e.g. identifying which muscles control joint motions in specific directions) can be additionally employed (Figure 2). Integrating different types of research (descriptive + cross-sectional + prospective + opinion) results in rich overall decision-making.54,69,72 Because little netball correlation, simple linear regression, or prospective research has been performed, the design of netball-specific knee ligament injury prevention screening draws from other related studies.
The Beighton score includes joint assessments to identify individuals with general joint hypermobility (GJH),105,106 which is prevalent in child107 and adult108,109 netball players. No published work has examined relationships between Beighton scores and knee biomechanical characteristics derived from 3D motion analysis of DLL/SLL tasks. In contrast, GJH is prospectively linked to an increased risk of all knee injuries110 and noncontact ACL injuries111 in athletic females. General joint hypermobility assessment using the Beighton score procedures may be useful for identifying players predisposed to increased risk for noncontact knee ligament injury.
The ankle is an important component in the lower-limb kinetic chain.112 In DLLs, decreased straight-knee ankle dorsiflexion (DF) ROM measured with a goniometer was related to increased VGRFs, knee external abduction moments, and knee abduction displacements.113,114 In DLLs, decreased bent-knee ankle dorsiflexion ROM measured with the weight-bearing lunge test (WBLT) was related to decreased knee flexion displacements.115 No prospective work has reported an association between ankle dorsiflexion ROM and noncontact knee ligament injury. Screening ankle DF ROM with a goniometer or the WBLT may provide data for identifying players predisposed to sub-optimal landing biomechanics.
The lateral trunk muscles influence pelvis position and motion104,116 and pelvis position and motion influence knee biomechanics.104,117 In SLLs, decreased trunk rotation strength measured with an isokinetic dynamometer (IKD) was related to increased knee abduction displacement.118 In a single-leg squat (SLS), decreased isometric side-bridge strength measured with a handheld dynamometer (HHD)119 and decreased strength-endurance measured via holding-time120 were related to increased knee abduction angles. In prospective work, large trunk lateral flexion displacements following laterally-directed perturbations were linked to higher odds for experiencing noncontact ACL injury.121 Screening lateral trunk muscle performance with a HHD or isometric holding-times may have utility for identifying players predisposed to sub-optimal landing biomechanics and risk for noncontact knee ligament injury.
Lower-limb muscles generate internal moments that absorb foot-ground impact forces19 and stress-shield skeletal tissues from excessive loads.122 Outside 3D motion analysis, lower-limb internal moment generating ability is inferred using strength tests.123 For SLLs, decreased isometric hip abduction strength measured with a HHD was related to increased knee abduction angles.124 For SLLs, decreased isometric hip external rotation (ER) strength measured with a HHD was related to increased VGRFs, knee external abduction moments, knee abduction angles, and knee anterior shear forces,86,124 and decreased isometric knee ER strength measured with an IKD was related to increased knee IR angles.125 For SLLs, decreased SLS strength measured with a barbell and decreased isometric knee flexion strength measured with an IKD were related to increased knee abduction and IR angles.126 In prospective research, decreased lower-limb strength estimated with one-repetition-maximum (1RM) barbell back-squats was associated with increased odds for traumatic knee injuries.127 In other prospective and case-control work, decreased isometric hip abduction and ER strength estimated with a HHD128 and decreased knee flexion strength estimated with an IKD129 were associated with noncontact ACL injuries. Screening hip and knee muscle strength with double- and single-leg strength tests may be useful for identifying players predisposed to sub-optimal landing biomechanics and risk for noncontact knee ligament injury. Considering kinesiological modelling, given that the quadriceps and gastrocnemius/soleus control knee flexion and ankle DF, respectively,103,104 and the dissipation of landing impact forces,92 screening of knee extensor130 and ankle plantarflexor131,132 muscle strength is wise. Isokinetic dynamometers and HHDs can be expensive and not easily available to community-based practitioners.130 Alternatively, leg press, knee flexion, and knee extension resistance machines can be more readily accessible.130 Single-leg 1RM strength tests can be performed with netball players in local communities and contribute to knee injury prevention procedures.130,133 Combining free-weight and resistance machine procedures for double-/single-leg strength testing may be the most thorough approach.66
Balance is the process of maintaining the body’s center-of-mass and center-of-pressure within its base-of-support via internal moments countering external moments that act to destabilize the body and its joints.134 Balance is a sensorimotor process involving proprioceptive, visual, and vestibular sensory information used by the central nervous system to adjust motor output and maintain postural equilibrium.134 For SLLs, increased single-leg stance center-of-pressure excursion (worse balance) was related to increased knee external abduction moments.135 In prospective studies, reduced dynamic balance defined by three (anterior/posteromedial/posterolateral) of the six directions in the Star Excursion Balance Test (SEBT) was associated with increased odds of lower-limb injuries including knee sprains.136 The SEBT has since been modified to use just the anterior, posteromedial, and posterolateral directions in the form of the Y-Balance Test (YBT).137 Reduced YBT performance defined by a reduced anterior/posteromedial/posterolateral composite score138 and a reduced anterior score alone139 have been prospectively linked to lower-limb noncontact injuries. Reduced static balance defined by a computer-force plate system has been associated with increased ACL injury frequency.140 Screening single-leg balance (SLB) with procedures such as the SEBT, YBT, and timed eyes-open/eyes-closed balance may provide data for identifying players predisposed to sub-optimal landing biomechanics and risk for noncontact knee ligament injury. Timed eyes-closed SLB tests have been used in preseason screening for community-level netball players.25,141
Neurocognitive performance refers to cerebral neural functions contributing to cognition and includes processes such as visual attention, visual memory, verbal memory, processing speed, reaction time, and dual-tasking.142,143 Neurocognitive performance is integrated with sensorimotor functions (proprioception, neuromuscular control) to activate skeletal muscle and maintain joint stability during athletic tasks.142 No published work has examined relationships between measures of neurocognitive performance and knee biomechanical characteristics derived from 3D motion analysis of DLL/SLL tasks. One study, however, reported that decreased neurocognitive performance (decreased visual memory) was associated with increased knee abduction angles during sidestep cutting.144 Preseason neurocognitive assessment using the Immediate Post-Concussion Assessment and Cognitive Testing (ImPACT) procedures145–147 was linked to in-season lower-limb sprains148 and noncontact ACL injuries.149 Screening neurocognitive performance with the ImPACT procedures or other computerized systems may have utility for identifying players predisposed to sub-optimal knee biomechanics and risk for noncontact knee ligament injury.
Movement screening is the process of assessing athletes’ kinematic patterns relative to the biomechanics of injury mechanisms and high-risk events that contain the potential for noncontact knee ligament injury. Because 3D motion analysis equipment is not easily accessible to community-based practitioners, 2D motion analysis procedures have been developed using commonly available high-definition video cameras. During landings, 2D measurements of frontal plane knee kinematics (e.g. knee abduction angle) are not related to 3D measurements.150–152 During a SLS, however, 2D measurements of frontal plane knee kinematics are related to 3D measurements.150,153,154 Therefore, 2D motion analysis is not advocated for assessing DLL/SLL frontal plane knee kinematics.150–152 Conversely, use of a SLS in netball knee injury prevention screening is advocated because its knee biomechanical characteristics are related to those in netball-specific leap-landings.155 If high-definition video cameras are not accessible, generic observational DLL (e.g. Landing Error Scoring System [LESS]-Real Time [LESS-RT],156 Tuck Jump Assessment [TJA]157), SLL (e.g. Qualitative Analysis of Single-Leg Loading158), and SLS158,159 movement screens have been developed where the observer visually scores the athlete’s hip-knee-ankle kinematics according to pre-defined criteria. Generic DLL movement screens such as the LESS and TJA are not related to the biomechanics of netball-specific SLLs.160 One group reported the reliability of the ‘Netball Movement Screening Tool’ (NMST) which contains 10 tasks deemed relevant to assessing netball knee injury risk.161 The NMST has not been used further beyond another group who employed the NMST to evaluate outcomes from a performance training program.162 For prospective work, increased trunk ipsilateral lateral flexion and knee abduction measured with 2D motion analysis during a SLL were associated with increased frequency of noncontact knee soft tissue injury.163 Increased “dynamic knee valgus” measured with 2D motion analysis during a SLL was evident in female athletes who later experienced a noncontact ACL injury compared to those who did not.164 Poor (higher) LESS scores have been prospectively associated with increased frequency of noncontact ACL injury.165 Screening whole-body and knee kinematics patterns with procedures such as 2D motion analysis and observational movement screens may be useful for identifying netball players predisposed to sub-optimal landing biomechanics and risk for noncontact knee ligament injury.
The lower-limb functional performance test (FPT) includes hop, leap, jump, linear-sprint, change-of-direction, and agility tasks.166 In knee injury prevention, single-leg FPTs are recommended to isolate each lower-limb and expose unilateral deficits that can remain hidden in double-leg tasks.166 In netball, SLL versus DLL occurs on 58.5-67.1% of occasions14,167 and, therefore, single-leg FPTs are important components of netball-specific knee injury prevention screening. Single-leg FPTs (e.g. hop, leap) recreate the joint compression/shear/torsion/rotation forces encountered in sport-specific activity166,168,169 and are measured using performance-related variables such as distance (centimeters) or time (seconds).166,170,171 No study has examined the association between single-leg FPT performance-related variables and knee biomechanical characteristics derived from 3D motion analysis of DLL/SLL tasks. For prospective research, athletes with a single-hop-for-distance mean distance of ≤64% of height for either limb were at increased risk of thigh and knee injuries172 and athletes with a side-to-side difference (asymmetry) of >10% for the single-hop-for-distance experienced more frequent noncontact ankle and foot trauma.173 Screening single-leg FPTs may provide data for identifying netball players predisposed to increased risk of noncontact knee ligament injury. Further considerations include that some FPTs may be more suited to assessing lower-limb force production (e.g. vertical-hop) versus force absorption (e.g. horizontal-hop) ability.166,174 The shared variance between vertical-hop and horizontal-hop performance in netball players is low and, therefore, such tests capture different aspects of lower-limb motor-performance.174 Unidirectional (e.g. triple-hop-for-distance)171 and multidirectional (e.g. zig-zag hop)170,171 repeated hop single-leg FPTs may also be useful for adding greater repeated impact and frontal and transverse plane challenges to the knee joint.166,170 Recently, screening of a community-level adult netball team using single-leg FPTs revealed that side-to-side asymmetries of >10% for the triple-hop-for-distance, single-hop-for-distance, and vertical-hop existed for 8.7%, 8.7%, and 52.2% of players, respectively.141 Given such considerations, netball knee injury prevention screening may require a selection of different single-leg hop FPTs.
DISCUSSION: CLINICAL INTEGRATION AND APPLICATION
Based on the different types of research cited in the previous section, suggested noncontact knee ligament injury intrinsic risk factor screening procedures appear in Table 3. In terms of integrating and applying such procedures in sports physical therapy practice in netball, it may not be necessary to perform all tests in Table 3. Clinicians can decide for themselves which procedures are viable based on their local logistical constraints (e.g. equipment/personnel/finance/time availability).66 When a battery of procedures has been assembled, and given the recursive nature of netball training and competition, serial screening should occur at appropriate timepoints across a season/year to reveal changes in a player’s risk profile.50,52,65,66
The majority of screening procedures in Table 3 are for modifiable intrinsic risk factors for which conservative interventions are applicable. One intrinsic risk factor, the Beighton score for GJH,105,106 is nonmodifiable. The value of including such a nonmodifiable risk factor is that further supplementary sensorimotor control interventions for enhancing knee functional joint stability can be considered for those classed as having GJH.175
When a battery of screening procedures has been administered, the sports physical therapist should design a targeted intervention program to address intrinsic risk factors that are of specific concern (e.g. hip abductor muscle strength, balance, reaction time).50,141,176–179 These interventions then contribute to stage three of the sequence of prevention.49 During stage three and across the competitive season, noncontact knee ligament injury incidence requires monitoring. At the end of the season, noncontact knee ligament injury incidence is compared to that of previous seasons; this represents stage four of the sequence of prevention49 and is a critical evaluative step in any primary prevention strategy for injury.44–46,48,49 Future research should endeavour to identify modifiable intrinsic risk factors for noncontact knee ligament injury specifically in netball. Research should be performed for all levels of the game and all competitive age groups.
SUMMARY
Netball is a team court-sport played worldwide and becoming more popular in the US. Noncontact knee ligament injuries are common due to a knee abduction collapse during landing. High-risk landing events that contain the biomechanical potential for noncontact knee ligament injury are common in netball. Cross-sectional research, prospective research, and kinesiological modelling provide insight into modifiable intrinsic risk factors linked to high-risk landing biomechanics and actual noncontact knee ligament injury incidence. This clinical commentary has described how theoretical principles (injury control, sequence of prevention, principles of screening in injury prevention, multifactorial model of injury etiology, complex systems theory, systems science), different types of research (descriptive, analytic-observational), and different levels of evidence (prospective, cross-sectional, clinician’s opinion) underpin a rational clinical reasoning process that develops screening procedures for community-level netball noncontact knee ligament injury prevention. An example of how such theories, research, and evidence can be applied by the sports physical therapist has been provided in the form of detailed explanations for suggested screening procedures (Figure 2, Table 3) and comments on the need for repeated screening at strategic timepoints across a season/year.
Conflict of Interest Statement
The author declares there are no conflicts of interest.