



Introduction
Acute knee injuries, especially to the ACL, often result in functional instability.1 Consequently, ACL injury can have a number of negative consequences on both the short- and long-term functioning of the knee joint.2–4
ACL injuries occur three to seven times more frequently in athletes compared to non-athletes, and represents a substantial problem in ball sports such as team handball and football,5–8 which involve sudden stops and side-cutting maneuvers. In 80 % of the cases, the ACL injury happens in non-contact situations.9 Further, the incidence of non-contact ACL injury is reported to be three to six times higher for women than men.3,9–13 Proper neuromuscular control is imperative for stabilization of the knee joint during athletic movements with injury risk. Especially, adequate hamstring activation before or during the landing phase is considered important to control excessive rotations and protect e.g. the ACL.11,12,14
Compared to male athletes, female athletes exhibit greater quadriceps EMG activity during vertical stop-jump tasks14 and side-cutting maneuvers,15,16 while male athletes often display higher hamstring activation in these situations with high risk of ACL injury.14–22 Moreover, reduced strength and recruitment of the hamstring muscles are considered significant risk factors in relation to non-contact ACL-rupture.23–25 Introducing preventive training programs have shown positive effects on the muscle-strength relationship between quadriceps and the hamstrings,22,24 as well as on the neuromuscular activation pattern in selected landing and side-cutting situations.22 The medial hamstring muscle(s) seem particularly important in this context, as a reduced medial (semitendinosus) electromyographic (EMG) activity during side-cutting in combination with a high activity in the lateral quadriceps (vastus lateralis) have been shown to be related to an elevated risk of non-contact ACL injury.25 Previous research has identified dynamic valgus of the knee as a predisposing factor for ACL injury in female athletes.26 The balance between medial-lateral hamstring recruitment seems highly important for the control of dynamic valgus.27 Female athletes appear to have disproportionately greater EMG activity in their lateral biceps femoris muscle than male athletes when landing from a jump.28 Increased lateral hamstring recruitment potentially could lead to a more open medial joint space and thereby contributing to increased dynamic valgus, and hence contribute to increase the risk of non-contact ACL injury.28
Strengthening exercises for the hamstring muscles such as hip extension and isolated knee flexion (i.e. leg curl) typically show high levels of muscle activity in the lateral biceps femoris compared to the medial semitendinosus.29–33 From an ACL injury prevention perspective, it thus becomes relevant to examine the relative balance between semitendinosus and biceps femoris muscle activity during commonly used training exercises, in order to identify or develop exercises with high medial vs lateral hamstring muscle activity. Recent research has identified the Kettlebell swing and Romanian deadlift to be associated with a preferential activity in the semitendinosus vs. biceps femoris muscle,33,34 and as a common characteristic both exercises are performed with nearly straight knees and a forceful hip extension with the peak load at the most flexed hip joint angle. However, these exercises may vary in the technique, load and intensity of the movement, which may affect the activity of the muscles. Furthermore, progression in these exercises are frequently achieved by using a single stance leg, typically in a common belief that the preventive exercise effect is improved when the exercise involves an increased need for dynamic joint stabilization. However, the effect of this assumption on hamstring muscle activation levels has never been tested in controlled experimental settings.
The purpose of this study, therefore, was to investigate selected lower limb strengthening exercises performed either unilaterally or bilaterally to identify 1) which exercise elicited the highest hamstring activation, 2) which exercise elicited the highest ST activation, and 3) to examine if unilateral exercise execution altered the medio-lateral hamstring activation pattern. Furthermore, the kinematic characteristics of each specific exercise and execution modality were determined to reveal possible causes for differences in medio-lateral hamstring activation between the different exercise conditions.
Methods
Subjects
Female team handball players from the three highest Danish team handball divisions were invited to participate in the study. Twenty-three players (mean age: 20.7±2.9 year; mean height: 176.0±5.7 cm; mean weight: 73.1±7.3 kg; mean handball training frequency: 3.2±0.9 sessions/week; mean strength training frequency: 2.8±0.8 sessions/week) with no previous history of ACL injury or hamstring injury volunteered to participate in the study.
The study was approved by the local Ethics Committee (H-18063645). All participants received written information about the study and each participant confirmed their participation by signing a written declaration of consent. All participants were informed about the protection of subject rights.
Test procedures
A pretest familiarization session was carried out on a separate day prior to the first test day. In this session, all experimental exercises were demonstrated for the participant by an experienced test instructor. Afterwards the participant executed the exercises with guidance from the test instructor to ensure that the exercise was correctly executed. When correct technique and movement execution were achieved, the individual load for the testing day was established for each exercise. The kettlebell weight corresponded to a 20RM load, whereas an 8RM load was chosen for the bilateral Romanian deadlift and hip thrust exercises. During all unilateral exercise conditions, the exercise load/weight corresponded to half of the load used in the corresponding bilateral exercise condition.
On the day of testing, all participants performed a standardized warm-up program that involved five stretching exercises for the larger muscle groups (quadriceps, hamstrings, chest, shoulders, back) followed by a number of low-load strength training exercises (squats, lunges, hip bridge, back extensions, crunches, push-ups) performed in 3 sets of 10 repetitions for each exercise with 30-45 s rest between sets. After warm-up, participants performed three maximal voluntary isometric knee flexor contractions (MVC) of five seconds duration (30-s pause between successive MVC trials) were performed to determine maximal volitional EMG activity in the lateral and medial hamstring muscles (more details provided below). Finally, for familiarization ten repetitions were performed for each exercise using a 16RM load (40RM in kettlebell swing) altogether followed by three minutes of rest. Subsequently, five test repetitions using an 8RM load (20RM load in kettlebell swing) were performed and sampled for later off-line analysis. A total of six exercises were performed in a cluster randomized order using lottery notes with numbers from 1 to 6. The unilateral exercises were performed on both legs (and data averaged between the two limbs), in the order of dominant non-dominant leg. Approximately three minutes of rest were prescribed between exercises to avoid fatigue.
Exercise protocol
The exercise protocol involved three distinct lower limb strengthening exercises (kettlebell swing, Romanian deadlift and hip thrust). The exercises were selected based on their regular involvement in clinical practice and athlete physical conditioning, as well as being inspired by previous ACL injury prevention programs.29,35–41 As a common characteristic, all selected exercises involved a large degree of hip flexion and -extension.
Kettlebell swings (KS)
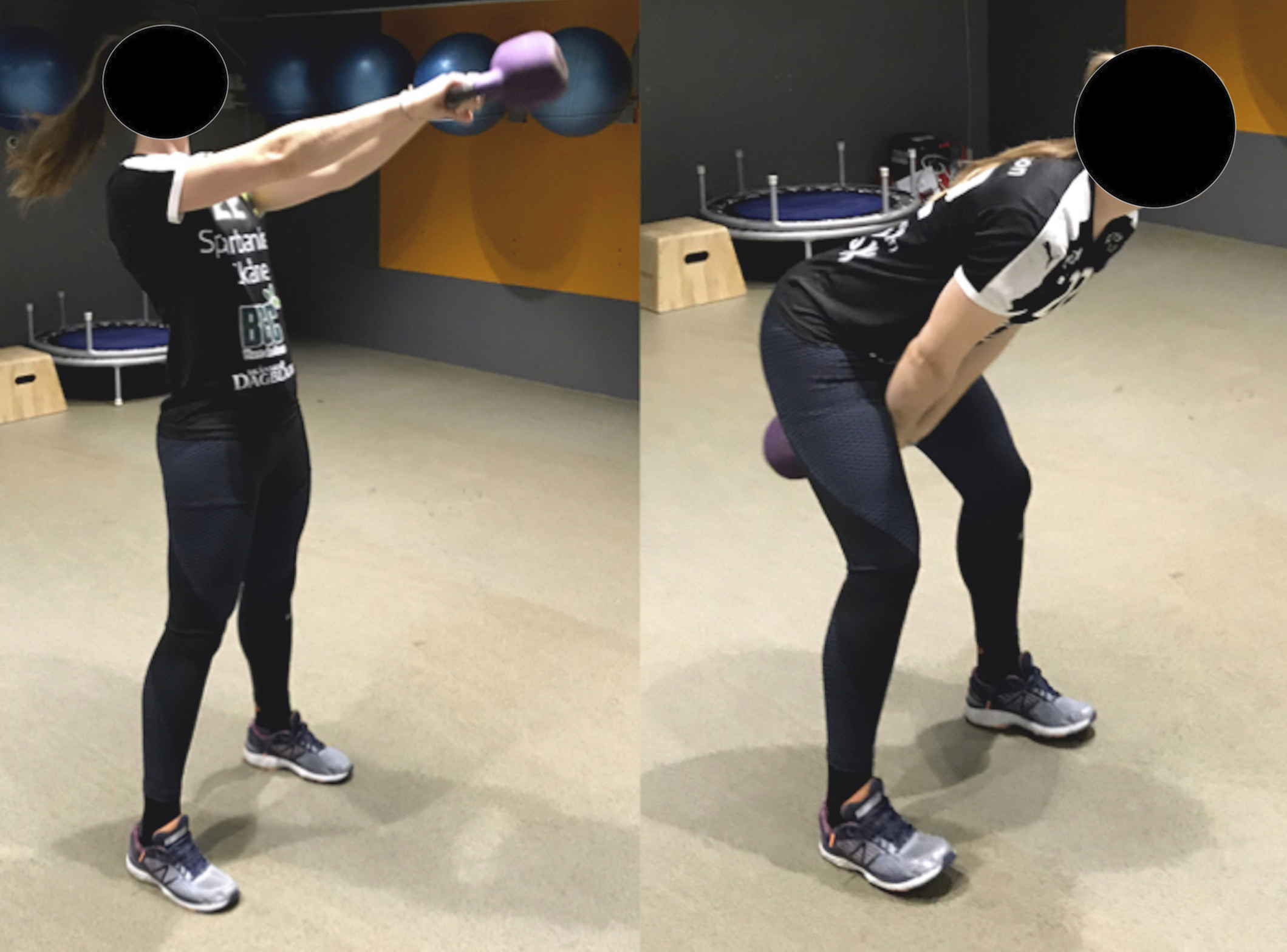
Participants were standing with their feet positioned in parallel (shoulder width distance between right and left foot). The exercise was always performed bilaterally (no unilateral variant) using an explosive (i.e. maximally accelerated) hip extension to swing the kettlebell up (chest level) using straight arms continuing into a down-ward swing between the legs, while in all swing phases maintaining a knee joint angle close to full extension (Figure 2A).
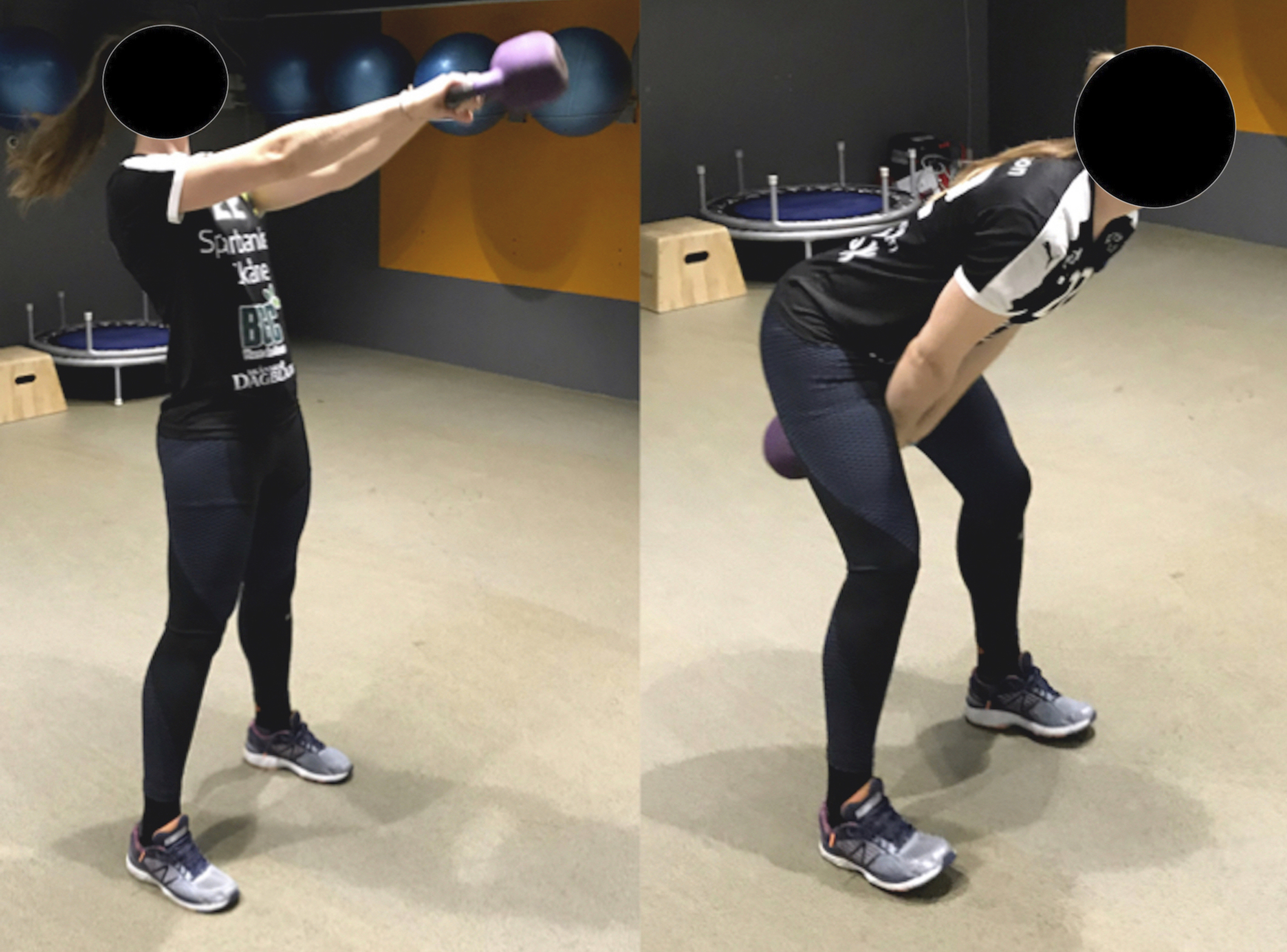
The kettlebell weight corresponded to a 20RM load i.e. the maximal weight the subject could swing 20 times without loss of correct technique. The subject performed a single set of ten swings using this load.
Romanian Deadlift (DL)
Bilateral DL: Participants lifted the barbell (load corresponding to 8RM) with the feet parallel and shoulder-width apart. The barbell was lifted from hanging right below the knees with an explosive extension of the hips until standing upright (Figure 2B). The knees were maintained at an angle near full extension.

Unilateral DL: Participants performed the exact same movement as described for the bilateral DL, except standing on one leg. The subject performed a single set of five repetitions with a load corresponding to half of the two-legs load (Figure 2C).

Hip thrusts (HT)
Bilateral HT: Participants were positioned supine with the upper part of the back supported on a bench and starting with flexed hips and knees. A barbell was placed on the upper part of the thigh (weight corresponding to 8RM) and was lifted as fast as possible by extending the hips. The exercise was performed using two different feet positions that resulted in different knee joint angles at full hip extension; first, a set of five repetitions with an ~90° knee angle (Figure 2D) and afterwards a set with ~110° knee angle (180° = full extension).

Unilateral HT: This exercise was performed as described above for bilateral HT testing, except using a single leg only. The subject performed a single set of five repetitions with a weight corresponding to half of the load used in the two-legs HT (Figure 2E). Unilateral HT was only performed as the 90° knee flexion end-position exercise.

Electromyography (EMG) recordings
The skin of the subject was shaved with a hand razor and carefully cleaned with ethanol before electrode placement on both legs. Bipolar surface EMG electrodes (2-cm inter electrode distance, Myon Aktos, prophysics SOL AB, Höör, Sweden) were placed at the BF and ST muscles according to standard recommendations.42 Raw EMG signals were pre-amplified, band-pass filtered (20-450 Hz) and sampled with a frequency of 1000 Hz. The EMG recordings were high-pass filtered using a 4th order Butterworth filter with a cut-off frequency of 10 Hz and subsequently smoothed by a symmetrical moving root-mean-square filter (RMS) with a window size of 30 ms and 29 ms running overlap.
Before exercise testing, the maximal EMG activity was obtained during maximal voluntary isometric hamstring muscle contraction (MVC), as described in detail elsewhere.41 Three maximal isometric MVC’s were performed for the knee flexors (hamstrings) of each leg separated by 30-s rest and the peak EMG amplitude of the three trials was used for later EMG normalization.41
All dynamic EMG data were normalized to the maximal EMG amplitude recorded during MVC testing.41 The peak EMG amplitude for each repetition was obtained, and the mean of five repetitions for DL and HT exercises,33,43 and ten repetitions in KS for each participant were used.33,41
Biomechanical analysis
All tests were performed in a biomechanical motion analysis laboratory with eight infrared cameras (Vicon T40 cameras, Vicon Motion Systems Ltd, Oxford, UK) with a frame capture frequency of 100Hz. Data were collected using inherent software, (Nexus 2, Vicon Motion Systems Ltd, Oxford, UK).
3D Biomechanical model
To obtain hip and knee joint kinematic data, a total of 22 reflective markers were placed over anatomical landmarks according to a modified Helen Hayes marker setup,44 except for the thigh markers, which were substituted by markers attached over the patella, to reduce the effect of wobbling masses.45
Statistical analysis
Shapiro-Wilk testing was performed to check for normality. Subsequently, a two-way analysis of variance (ANOVA) was performed in SPSS (Version 22, IBM SPSS Statistics) using a repeated measures procedure with Bonferroni corrections to determine whether differences existed in peak nEMG between exercise type and medial vs lateral hamstring muscles, respectively. Factors included in the model were muscles (ST and BF) and exercises (six exercises), as well as the interaction between these. Pearson correlation analysis was performed to examine the potential relationship between hip- and knee joint range of motion and muscle activity, respectively.
p-values of ≤0.05 were considered statistically significant.
A statistical power of 80 % to detect a difference of p=0.05 with a standard deviation of 20 in nEMG (expressed in % of peak EMG at MVC) and a between-exercise difference of 15 % points of peak nEMG was calculated to require a total of 16 participants.33
Results
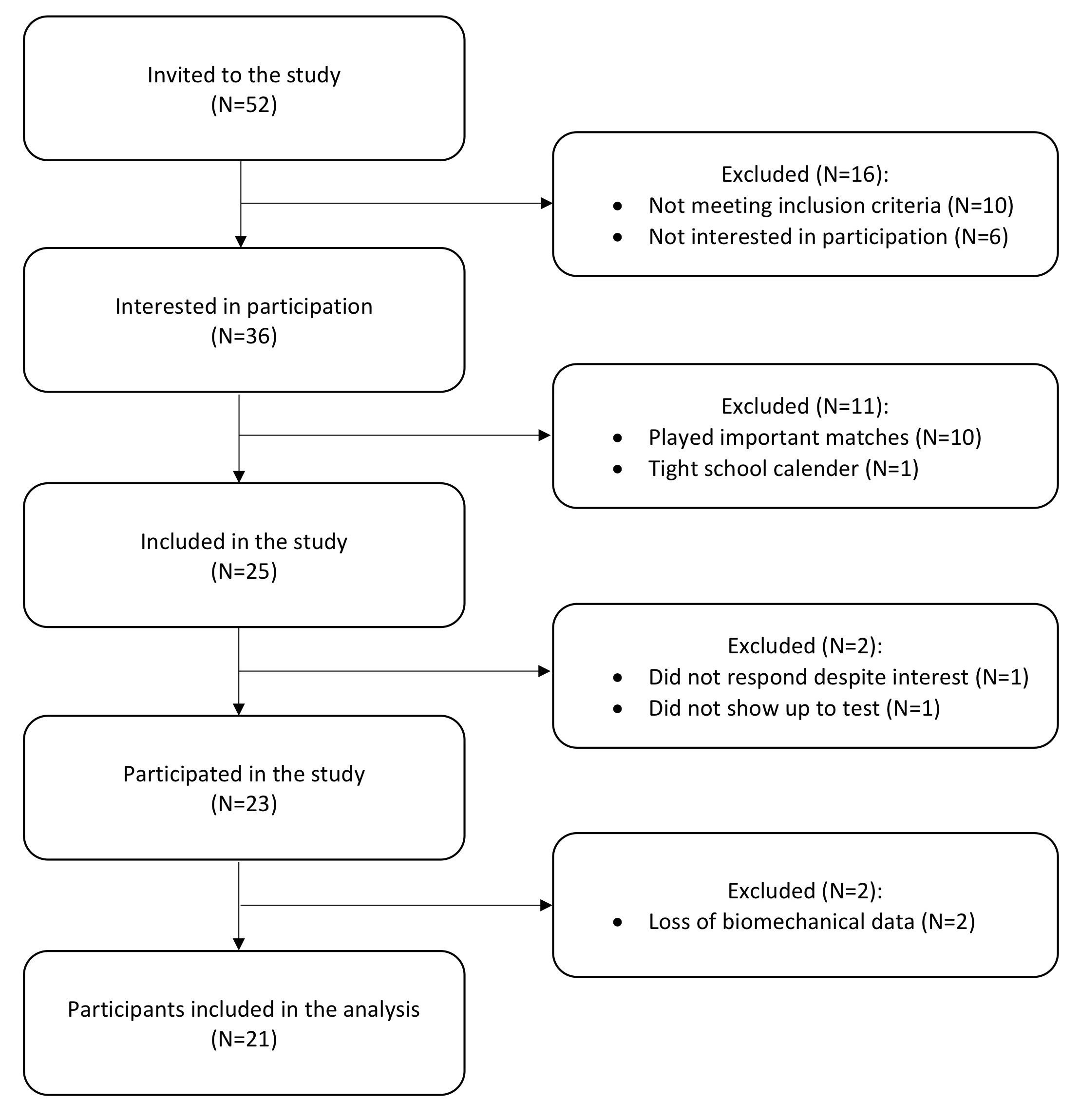
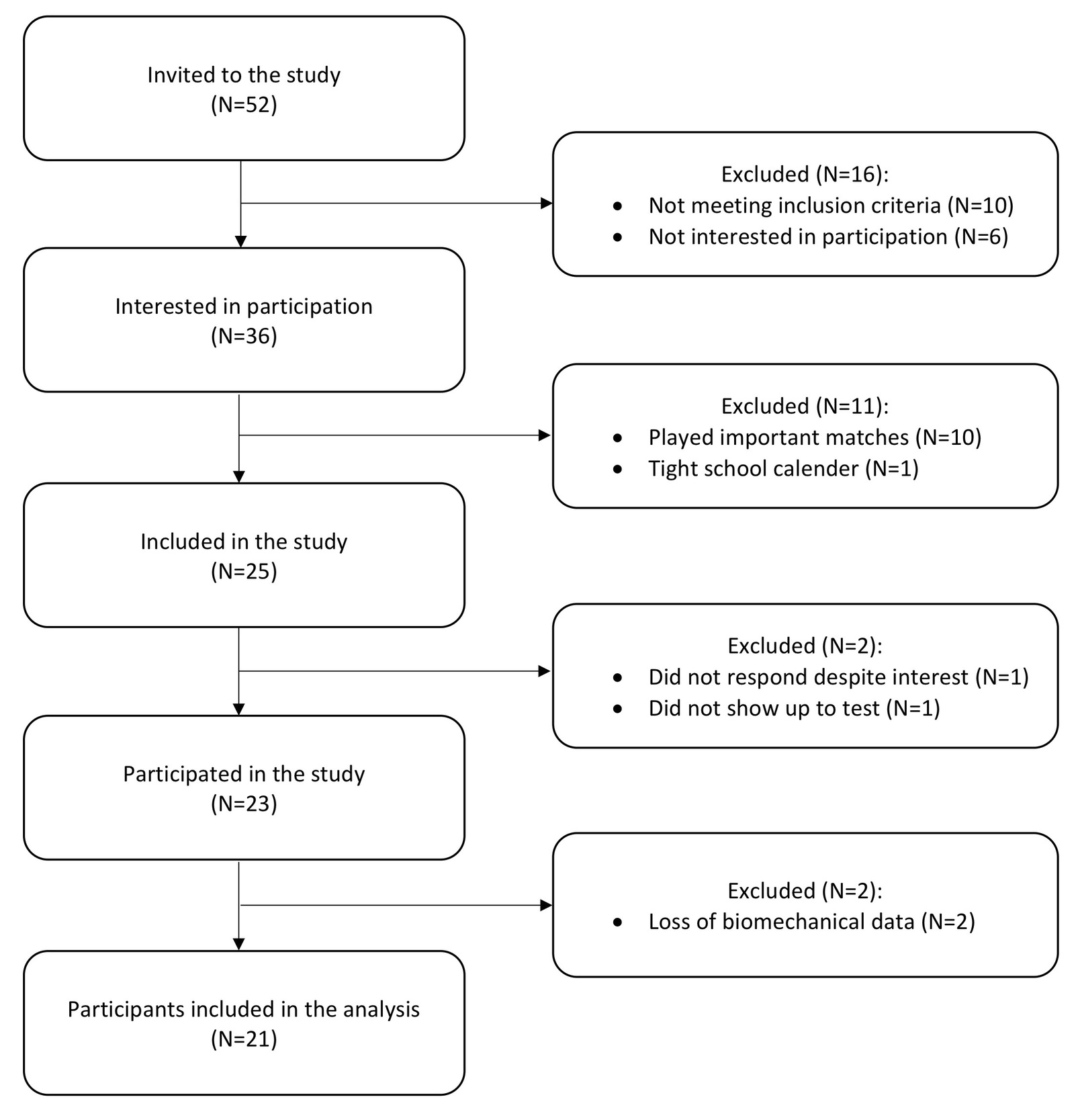
Data were excluded from two participants, due to undetected loss of markers during the test exercises. Thus, the present results contain data from 21 participants. Subject characteristics are presented in Table 1 with participant flow illustrated in Figure 1.
Hamstring muscle activation
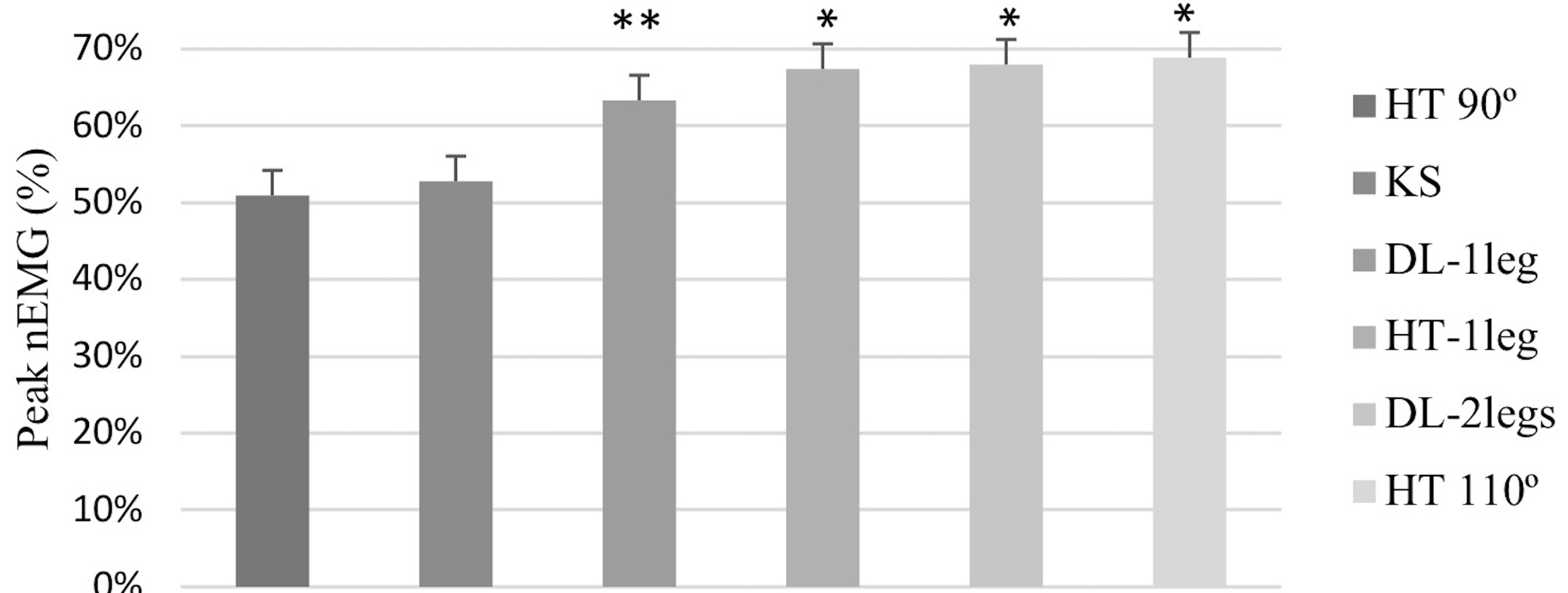
Total hamstring muscle activity (mean (ST+BF)) expressed as peak normalized EMG amplitude (nEMG) varied between the different test exercises (Figure 3). The HT exercise performed at 110° knee angle (HT 110°) showed the highest activity level of 68.9±16.6 % (mean ±SD). Hamstring activity levels for the other tested exercises were: Two-legs DL (DL-2legs) (68.0±18.8 %), Single-leg HT (HT-1leg) (67.4±18.3 %), Single-leg DL (DL-1leg) (63.6±16.7 %), KS (53.0±15.0 %), HT performed at 90° knee angle (HT 90°) (50.4±15.9 %).
_shown_as_group_mean___-_sem.jpeg)
Medial versus lateral hamstring activity
ST and BF muscle activity assessed in each exercise are presented in Table 2. ST showed greater muscle activity compared to BF, except for HT-1leg (69±18 % vs. 66±18 %) and HT 110° (71±18 % vs. 65±16 %). ST and BF activity levels for the other tested exercises were: DL-2legs (80±17 % vs. 57±20 %, p<0.0001), DL-1leg (74±16 % vs. 54±18 %, p<0.0001), KS (59±14 % vs. 47±16 %, p<0.0001), HT 90° (54±17 % vs. 47±15 %, p=0.038).
Medio-lateral activation balance
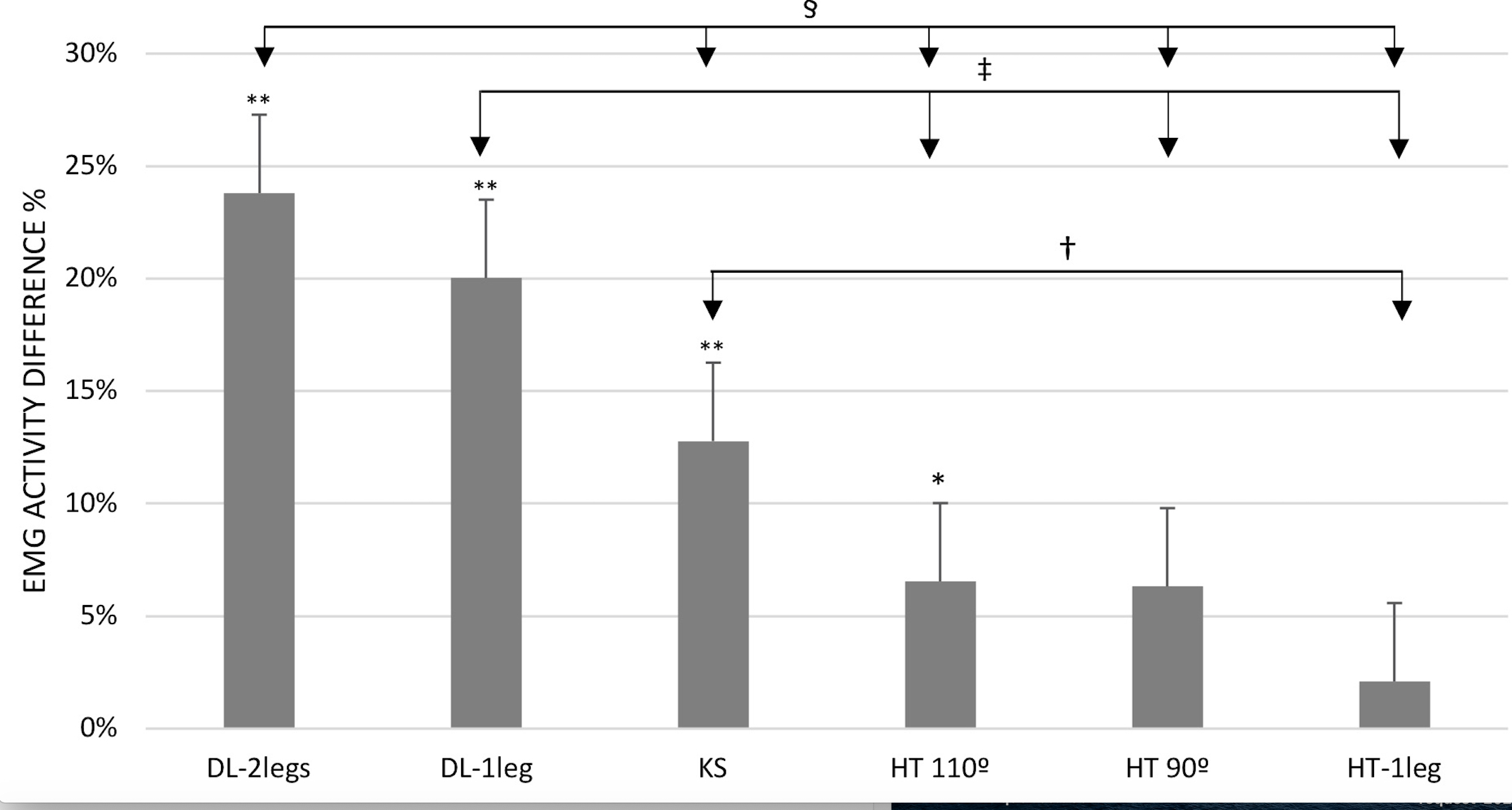
Within-exercise analysis of the medial-lateral hamstring activation balance (∆ = difference between ST and BF, ±SD) showed a preferential activation of ST over BF during DL-2legs (∆23.8±2.4 %, p<0.0001), DL-1leg (∆20.0±2.2 %, p<0.0001), KS (∆12.8±2.1 %, p<0.0001) and HT 110° (∆6.5±2.1 %, p<0.05), whereas no difference was found for HT 90° (∆6.3±2.3 %) and HT-1leg (∆2.1±1.0 %) (Figure 4, bar graphs).
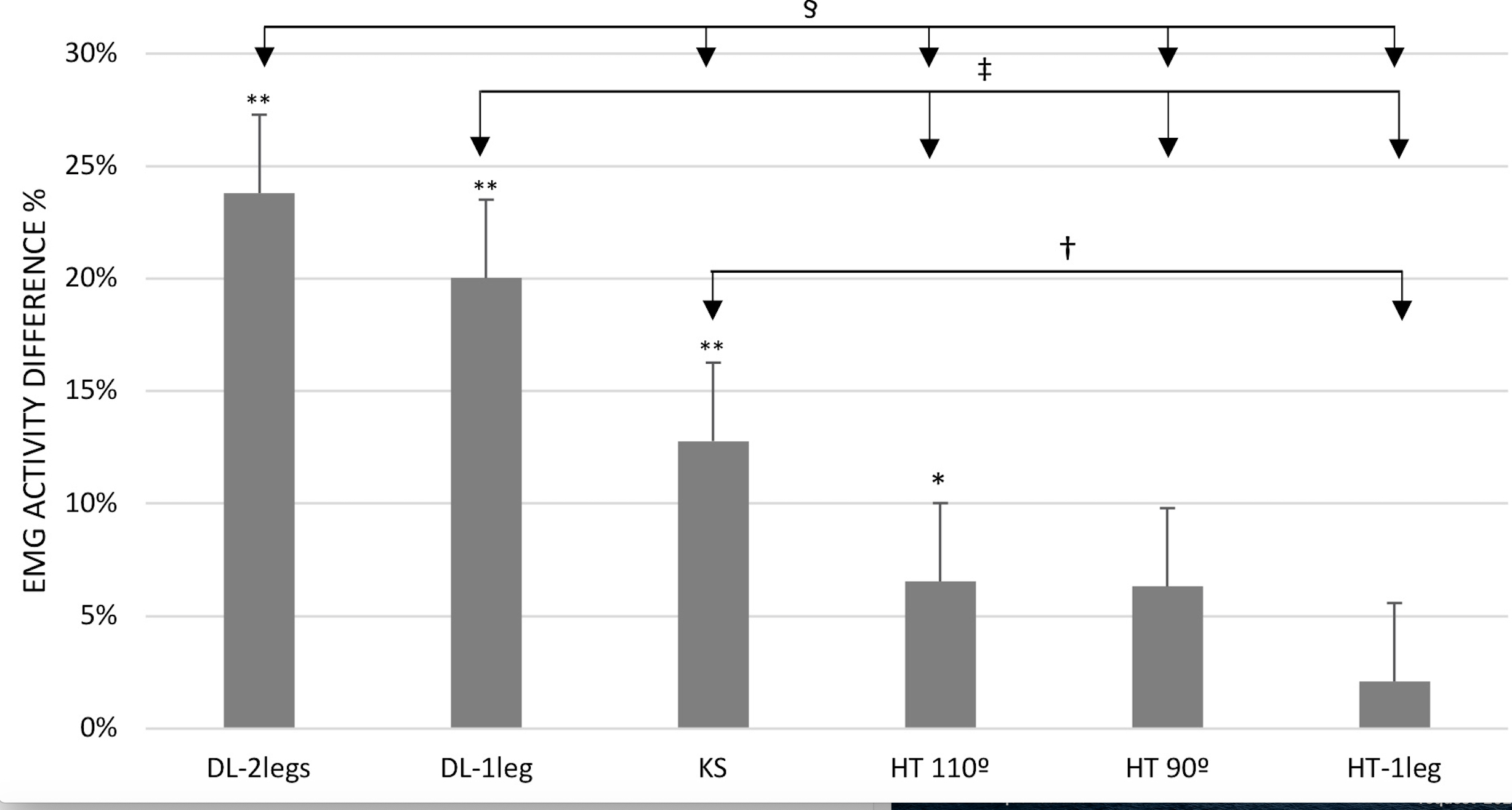
Between exercise analysis of the medial-lateral activation balance (Figure 4, arrows) revealed elevated muscle activity difference in favor of ST during DL-2legs compared to KS (∼∆11 %), HT 110° (∼∆17.3 %), HT 90° (∼∆17.5 %) and HT-1leg (∼∆21.7 %) (p<0.0001). Likewise, DL-1leg evoked greater ST-BF activity difference than HT 110° (∼∆13.5 %), HT 90° (∼∆13.7 %) and HT-1leg (∼∆17.9 %) (p<0.001). ST-BF muscle activity difference was also greater during the KS compared to HT-1leg (∼∆10.7 %) (p<0.01).
Relationships between hamstring muscle activity and knee joint ROM
For the HT exercises, HT 110° demonstrated a knee range of motion (ROM) between 79.9±9.2° and 56.8±9.7° flexion. HT 90° had a knee ROM between 102.2±9.9° and 76.1±10.2° flexion. A correlation analysis revealed a positive correlation (r=0.515, p<0.035) between more extended knee joint angles and increased ST and BF muscle activity.
The KS exercise was characterized by a hip ROM ranging from 2.4±8.2° to 96.5±8.0° of flexion whereas knee ROM was 9.5±5.5° to 48.2±11.5° flexion (0° = full extension). A positive correlation was revealed (r=0.436, p<0.024) between more extended knee joint angles and increased ST muscle activity during the ECC phase.
The DL exercises demonstrated a hip ROM between 9.7±5.9° and 100.2±7.5° flexion, and a knee ROM between 8.4±6.2° and 34.8±9.7° flexion. No correlation was observed between DL kinematics versus ST or BF muscle activity.
Relationship between hamstring muscle activity and hip extension angular velocity
The KS exercise demonstrated a mean hip extension angular velocity (HAV) of 312.2±58.1° s-1 and 204.2±40.2° s-1 in the CON- and ECC phase, respectively. A positive correlation was revealed (r=0.459, p<0.05) between increased HAV and elevated ST muscle activity.
The DL exercises performed on either two legs or a single leg demonstrated a mean HAV of 244.8±37.1° s-1 and 203.8±32.3° s-1, respectively, in the CON phase. Velocity in the ECC phase was 101.2±36.2° s-1 when performed on two legs and 71.6±21.9° s-1 on a single leg. No relationships were observed between HAV in both DL exercises and hamstring activity.
The HT exercises demonstrated a mean CON HAV of 222.7±54.8° s-1, 201.3±49.8° s-1 and 157.3±39.7° s-1 in HT 90°, HT 110° and HT-1leg, respectively. The ECC phase demonstrated a mean HAV of 93.2±39.0° s-1, 89.9±27.9° s-1 and 81.2±20.5° s-1 in HT 90°, HT 110° and HT-1leg, respectively. No relationships were observed between HAV in all HT exercises and hamstring activity.
A comparison analysis between exercises showed higher CON HAV in KS compared to both DL exercises and the three HT exercises (p<0.035). Likewise, DL-2legs showed higher HAV compared to DL-1leg, HT 110° and HT-1leg (p<0.023). Finally, DL-1leg, HT 90° and HT 110° showed higher HAV compared to HT-1leg (p<0.045). KS showed higher HAV compared to all the other exercises in the ECC phase (p<0.034).
Discussion
The main finding of the present study was that all examined lower limb exercises elicited a minimum of 50 % muscle activity in the hamstring muscles, which identified these exercises to be suitable for hamstring muscle strengthening. Further, the majority of the exercises were ST dominant, as evident by elevated ST compared to BF muscle activity. HT and KS displayed a positive correlation between more extended knee joint angles and elevated ST muscle activity. Likewise, KS revealed a positive correlation between increased HAV and an increase in ST muscle activity.
Hamstring muscle activation
All exercises involved high levels of muscle activity in the hamstring muscles, especially when knee joint angles were near full extension (180° = full extension). In the HT exercise, a positive correlation also was found between reaching more extended knee joint angles and elevated ST and BF activity. Similar observations have been reported by Collazo Garcia et al.,43 who tested four variations of the HT exercise, two of those similar to the HT 90° and HT 110° in the present study.43 Their study revealed high levels of ST and BF activity when HT exercise was performed with a more extended knee joint angle (ST: 70±17 % vs 71±18 % in the present study) compared to a 90° knee joint angle (ST: 32±8 % vs 54±17 % in the present study). The architecture of the ST muscle with long fiber lengths gives it excellent potential to contract at long muscle lengths.33 This could at least in part explain the lower muscle activation differences between ST and BF at more extended knee joint angles observed in both the Collazo Garcia and the present study.
Together with HT 90°, the KS exercise demonstrated the lowest levels of hamstring muscle activity. Previous studies have reported similar magnitudes of normalized muscle activity in the KS exercise.46–48 In contrast, a single previous study observed hamstring activity levels in KS reaching 90% of nEMG, which was recorded at 7±8° knee joint flexion.33 This is in contrast to the present study, which demonstrated a mean knee joint ROM between 10.7±4.1° and 48.2±11.2° flexion (mean for KS: 30.9±6.7°). Furthermore, the present study revealed a positive correlation between more extended knee joint angles and increased hamstring muscle activity in the KS exercise. Even though Zebis and coworkers used a similar setup and study population, the more extended knee joint angles in their study could possibly explain the high hamstring activity values observed in their study.30
ST-dominant exercises
The present study revealed that DL and KS exercises preferentially activated ST over BF, and at intensity levels sufficient to stimulate muscle strength gains. Likewise, Zebis and coworkers reported DL-2legs and KS to be highly ST dominant exercises.33 During KS and DL, the hamstring muscles are extensively stretched with the highest load at the greatest hip flexion angles. Thus, the ST dominance may partly be explained by the fact that ST, in contrast to BF, are parallel fibered and characterized by long fiber lengths and a high number of sarcomeres in-series.49 This arrangement results in a large total shortening capacity (i.e. ensures large joint ROM) along with a high maximum velocity of contraction.50,51 Even though the KS may be superior to DL in reflecting real life sports activities due to its functional execution, our study clearly demonstrates that when DL is performed explosively using either a single leg or two legs, it evokes high preferential activation of the ST muscle.
Unilateral exercises
Although the present study did not find a difference in the medial-lateral hamstring activation levels between bilateral and unilateral DL exercises, as a novel observation the present data indicated unilateral DL to involve high ST muscle activity while incorporating an important element of postural balance control. This may be relevant to consider in rehabilitative and prophylactic hip and knee stability training planning.
To the authors’ best knowledge only two studies have previously examined hamstring muscle activity during single-leg DL exercise.48,52 Examining female athletes, Tsaklis and coworkers reported higher ST muscle activity compared to BF during DL-1leg,48 even though muscle activity levels per se were lower compared to the present study. The fact that DL-1leg is a ST dominant exercise, despite low exercise loads,48 indicates that it may be relevant to implement this exercise in early rehabilitation after ACL reconstruction, where high exercise loads are contraindicated.
No previous studies have examined hamstring muscle activity during unilateral HT, however, neuromuscular activity has been assessed in various lower limb muscles including the hamstrings during different bridge exercises using a single leg.53–55 The bridge exercise is comparable to the HT, but the shoulders are supported on the floor instead of a bench, while still involving extension of the hip. When ST muscle activity was examined during single-leg bridge exercise performed with different knee joint angles, higher ST muscle activity was noted between 90° (57±31 %) and 60° (79±32 %) compared to the 120° (19±12 %) knee joint flexion.54 Similar activity levels were noted in the Lehecka study for the BF muscle (69±18 %), which more or less is comparable to the results from the present study (ST: 69±18 % and BF: 66±18 %).
Unilateral HT exercise revealed significantly lower HAV compared to bilateral HT, KS and DL exercises. Furthermore, unilateral HT demonstrated the smallest medial-lateral hamstring activation difference. In the execution of this exercise, stability around the hip and core is essential for ensuring a stable (i.e. non-tilting) pelvis. This weight shifting caused by the unilateral execution of the exercise might have caused a more equal medial to lateral activation. Notably, unilateral HT did not seem to be effective of elevating ST muscle activity over BF. However, this exercise could be preferable when focusing on improving hip and core stability, as well as eliciting high overall hamstring muscle activity, without increasing direct load on the knee joint.
Limitations
During the process of off-line data analysis, a number of participants demonstrated knee joint flexion angles in the KS that were more flexed (~25-30°) than the target position of 15°, which were not readily apparent during the time of testing. Furthermore, as this study evaluated selected lower limb training exercises among female athletes, the present findings and conclusions may not be readily transferable to male athletes or untrained persons.
Conclusions
In conclusion, the present study identified a number of lower limb strength exercises with high levels of neuromuscular activity in the hamstring muscles. As the main study finding, all these exercises involved higher ST activity over BF. Equally important, unilateral as well as bilateral DL exercises showed the greatest medial-lateral activation difference favoring ST activation compared to all other exercises.
The kinematic data furthermore illustrate that ensuring extended knee joint angles and increasing HAV may be key focus areas for health care professionals and physical conditioning coaches, and these aspects may be more challenging to achieve during explosive-type exercise such as the KS.
Conflicts of interest and source of funding
The authors report no conflicts of interest and no source of funding.