

Reviewing Current Practice Patterns
Anterior cruciate ligament (ACL) injuries are all too common in athletic participation. Sources have reported the incidence as high as 200,000 ACL injuries per year in the United States alone.1 It is customary in the United States to pursue anterior cruciate ligament reconstruction (ACLR) after injury in order to return to the previous level of sport. While many healthcare professionals and athletes are painfully aware of how common ACL injuries are, few realize, or at least openly acknowledge, that the likelihood of returning to sport is far from guaranteed. Pooled data from a systematic review and meta-analysis found that only 65% of individuals returned to their preinjury level of sports participation following an ACLR, with only 55% going on to participate in competitive sports.2 Other studies have shown that, of those athletes under 25 years of age, approximately 23-29% will go on to incur a second ACL injury.3,4 While there are many factors to consider when reviewing this data, it should, at minimum, cause us all to question whether the current state of ACL management is acceptable. Stakeholders would benefit from taking a step back and reflecting on whether current practice patterns reflect what is truly in an athlete’s best interest.
Sports medicine personnel should acknowledge and respond to the problem of high reinjury rates and relatively low rates of returning to sport. A recent scoping review identified the most common criteria used to clear individuals to RTS after primary ACLR.5 Of the 209 studies reviewed, 85% reported the use of time as a criterion for RTS, with 42% using it as the sole criterion.5 This fixation on using time as a RTS determinant is deeply engrained in the physical therapy profession, so much so that ever since Dr. Shelbourne began discussing accelerated rehabilitation after ACLR in the 1990’s, patients and sports medicine providers have pushed the speed limits of rehab. Kevin Wilk spoke to this in 2005,6(p51) poignantly noting, “Speeding through the rehabilitation program may have more risks than benefits. When we speed in our automobiles we may be caught by the law and pay a fine. If we speed in the rehabilitation program, we may have to suffer more significant consequences—patients with unsatisfactory knee function for the rest of their lives.” The authors of this manuscript argue that the majority of sports medicine professionals – physicians and physical therapists alike – are dangerously exceeding the speed limits of rehab.
Looking closer at the issue of time as a RTS determinant, Burgi et al.5 noted that 72% of practitioners use ≥6 to <9 months as their standard to clear an athlete for play. Is waiting six to nine months sufficient to maximize potential for a safe RTS? The vast majority of the time, the answer is an emphatic, NO! Cristiani et al.7 found that of 4093 individuals assessed at six-months post-operative ACLR, only 35% and 47% achieved ≥90% limb symmetry for isokinetic quadriceps and hamstring strength, respectively. Additionally, only 67% achieved ≥90% limb symmetry for a single-leg hop test. Collectively, only 19.6% achieved symmetrical knee function with all three standardized tests (isokinetic quadriceps strength, isokinetic hamstring strength, and single-leg hop test). Similar data has been shown for athletes nine months post-operatively, noting that only 11% of subjects (7 of 62) passed RTS testing that included the Landing Error Scoring System, three single-leg hop tasks, isokinetic quadriceps and hamstring strength, as well as two outcome measures (IKDC and ACL-RSI).8 A similar study had equally striking findings, noting a seven-fold greater risk of injury for individuals who RTS before nine months post-operatively.9
Some authors have gone so far to suggest that RTS should be delayed until two years after ACLR,3 noting that baseline joint health and function are not typically achieved until 24 months post-operatively; thus, delaying RTS until this is achieved significantly reduces the incidence of second ACL tears.3 While this may scream in the face of current practice patterns, the sports medicine community should not be quick to discount it.
The use of a limb symmetry index (LSI) is of particular interest when qualifying someone’s RTS readiness. It is vital to appreciate that symmetry may not correlate with movement quality nor does it indicate whether the athlete has achieved pre-injury status or acceptable population norms. Gokeler et al.10(p948) notes, “An athlete may have perfect limb symmetry and yet be underprepared to compete because both extremities are much weaker or more poorly controlled than a healthy athlete.” Despite these shortcomings, LSI is often used in association with strength and hop testing. While there is considerable variation between studies regarding an acceptable LSI, the majority of authors suggest that a LSI of 85-90% is satisfactory.5 While this may be normative practice, is it truly best practice? Gokeler et al.10(p949-950) goes on to note that, “Despite achieving a LSI > 90%, patients demonstrated significant and clinical relevant deficits in performance for both limbs when compared to normative data from healthy athletes.” A similar study, albeit small, demonstrated that individuals achieving a LSI of >93% still exhibited markedly asymmetrical movement patterns during hop testing.11 A larger study revealed that athletes who achieved >90% LSI for strength and hop testing did not achieve 90% of their estimated pre-injury capacity with the same tests.12 At best, all of these athletes likely demonstrate compensatory adaptations (eg. detraining) on their uninvolved extremity; at worst, they demonstrate involuntary neurologic inhibition of the uninvolved limb due to the contralateral ACL tear.
No matter the mechanism, one can conclude that using LSI for hop testing and strength assessment has the potential to overestimate knee function. Therefore, interpretation of this data must be done cautiously.10 To be clear, the authors of this manuscript are not suggesting practitioners abandon LSI altogether; instead, the authors advocate for careful interpretation of the data in addition to raising the bar for what is considered passing. Clinical practice guidelines recommend a minimum of 90% LSI, yet advocate for a much higher standard of up to 100% symmetry.13 It is the opinion of the authors that despite the limitations associated with using LSI for RTS testing, and the apparent lack of consensus regarding passing scores, athletes should aim for 100% LSI for both strength and hop testing, with 97% the lower cutoff for hop testing and 90% the lower cutoff for isokinetic strength testing.
Another area that should draw attention in current practice is the use of patient-reported criteria. For example, in Burgi’s scoping review,5 only 12% of studies assessed personal or contextual factors, including confidence and self-reported knee function. The low utilization of patient-reported assessments contrasts recommendations from recent literature demonstrating that lower psychological readiness correlates with a higher risk of second ACL injury when returning to play among younger patients.14 Lower psychological readiness can also lessen the likelihood that an individual returns to sport at all, inciting fear of reinjury and decreased self-efficacy, even after one is deemed physically ready to return to play.15
As readers evaluate current practice patterns for ACL injury management, it is important to compare how these stand up to current recommendations. A consensus statement on RTS from the First Congress in Sports Physical Therapy outlines five specific recommendations to guide the practitioner when deciding to clear an individual for RTS.16
-
Use a group of tests (aka: a test battery).
-
Choose open tasks (less controlled) over closed tasks (more controlled) when possible.
-
Include tests with reactive decision-making elements.
-
Assess psychological readiness to RTS.
-
Monitor workload throughout the RTS transition.
When examining these recommendations in light of current practice patterns,5 it is clear that a sizeable gap exists. In retrospect, it appears as though the sports medicine community may have a monocular, often short-sighted view of ACL rehabilitation and RTS testing, which may be a notable contributor to low RTS rates as well as high reinjury rates. In response to this hypothesis, the authors of this manuscript aim to disseminate a robust model for RTS testing that incorporates temporal and criterion-based factors, as well as intrinsic and extrinsic data.
Let’s Get Back to the Basics
It is commonplace for sports physical therapists to commence an athlete’s rehabilitation by creating a needs analysis that details his or her athletic demands. Take for instance, a high school soccer player. The athlete needs to be able to sprint, cut, jump, hop, take contact from other players, give contact to other players, rapidly accelerate, and rapidly decelerate, all while filtering the onslaught of visual, proprioceptive, vestibular and somatosensory inputs. In short, the athletic demands of soccer (or any sport at that), are complex and not easily captured by one or two simple tests. Therefore, using the individualized needs analysis, specific targeted interventions and functional testing can be developed in preparation for the athlete to RTS.
While every sport is unique and criteria must be tailored for individual needs, many commonalities span athletes of all levels, positions, and sports. Table 1 offers the reader a list of extrinsic criteria that most athletes will require to minimize the potential for re-injury, along with the various means of measuring the variable. While the proposed list is not exhaustive, it offers a practical testing battery when completing RTS testing based on available literature. Table 2 provides the rationale for the proposed recommended cut-off values.8,10,12,15,17–32
The vast majority of applied research to date has focused on modifiable risk-factors as criteria for RTS testing. There is an equally important arm of this discussion that needs to be explored: that of intrinsic risk factors. It is the opinion of the authors that many healthcare professionals often undervalue the influence of intrinsic risk factors on ACL reinjury when making RTS decisions. Female athletes, for example, are two to eight times more likely to sustain an ACL injury.33 Multiple anatomic factors, unable to be ameliorated by the patient, may predispose one to ACL injury.34 A list of these intrinsic risk factors is available in Table 3.34–36 While these factors may indeed be non-modifiable, their correlation with ACL tears should be acknowledged and influence one’s timeline for sports participation.
Practically speaking, the reader should compare two athletes who pass RTS testing seven-months following ACLR. Consider one patient who has no intrinsic risk factors: the athlete is male, a senior in college, and sustained a contact-related ACL tear during intramural flag football. In contrast, a 16-year-old female is also looking to go back to sport seven-months following ACLR. She has a history of a contralateral ACL tear, a family history of ACL tears, marked laxity of the knee, as well as a primary injury that was non-contact. Even if both athletes pass their respective RTS tests, the clinician should appreciate how uniquely different each athlete is, and how they should be managed as such. The authors offer specific recommendations for reconciling common intrinsic factors by delaying an athlete’s RTS and requiring them to complete a standardized ACL injury prevention program (IPP) that has been demonstrated to decrease the risk of ACL injury37,38 (Appendix 1).
Specific Testing Consideration
In order to account for the plethora of modifiable and non-modifiable risk factors associated with an ACL tear, the authors propose the use of a RTS testing battery similar to Appendix 1. Make note of the “Ticket to Entry.” These tests were selected as part of a screening tool in order to ensure the athlete is safe to undergo and complete RTS testing. If the athlete does not successfully pass the “Ticket to Entry,” they should not complete the remainder of the assessment.
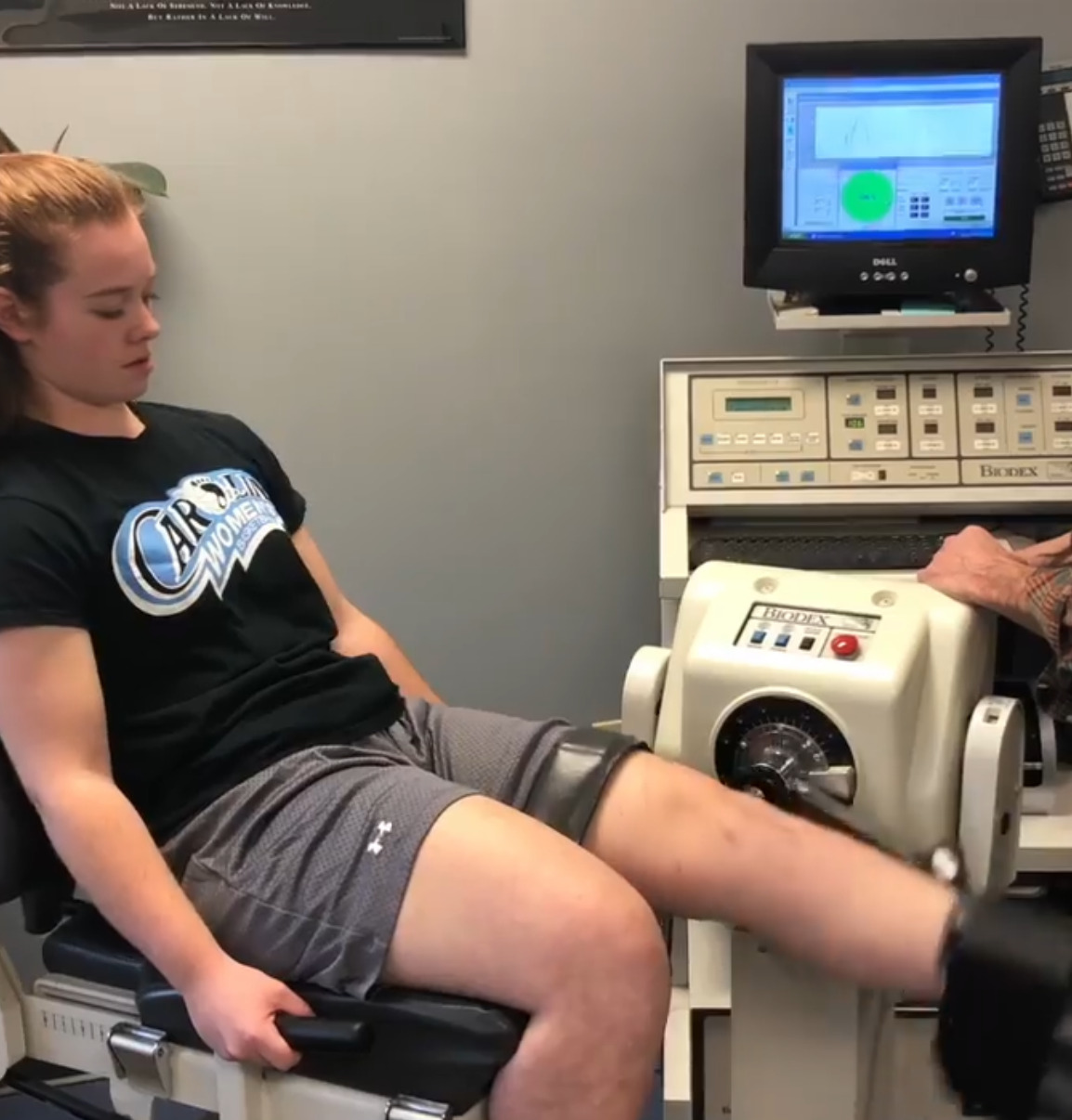
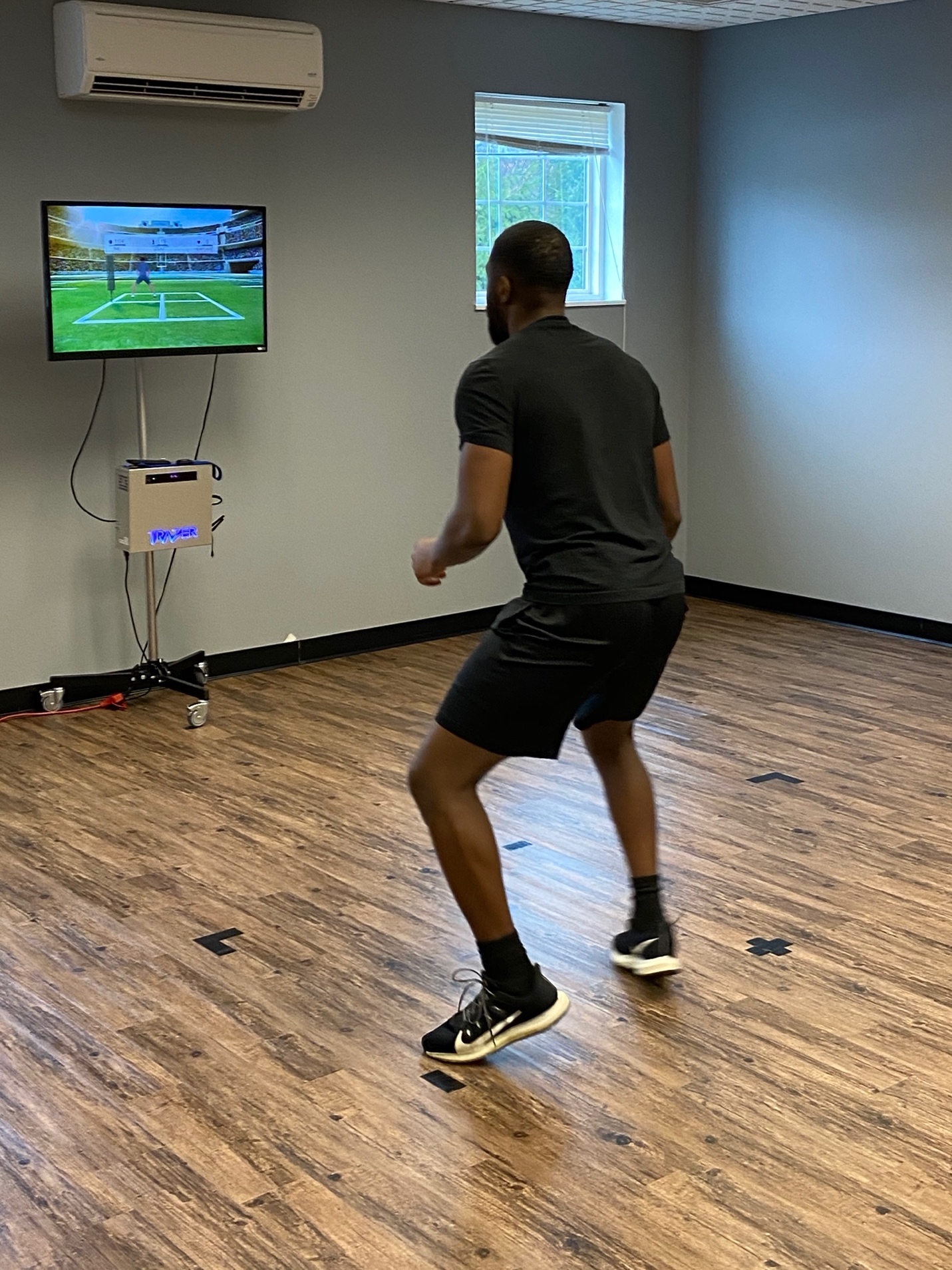
Given the complexity of some of the tests, as well as the necessary equipment (Figures 1-3), not all outpatient physical therapy facilities are poised to conduct RTS testing. Athletes may need to be sent to specific RTS testing centers that have the equipment and expertise in order make the determination. Finally, given the implicit bias that many physical therapists have towards their own patients, and the reality that physical therapists are not only assessing the athlete during testing but, in essence, their own performance as therapists, the authors recommend having a practitioner complete the testing who was not otherwise directly involved in the patient’s care.


Lastly, while a thorough discussion on acute:chronic workload ratios is beyond the scope of this paper, the authors of the manuscript would be remiss to not mention the importance of the concept, especially in light of the current RTS Consensus Statement.16 Simply put, as an athlete transitions back to participation, sport, and performance, it is important to achieve and maintain optimal loading. Monitoring an athlete’s current training load (acute) against the load imposed over the preceding four weeks (chronic) provides what is known as the acute:chronic workload ratio.16 Great debate exists on and off the field regarding the utility of the acute:chronic workload ratio and its ability to predict injury. The authors refer readers to a recent systematic review detailing many of the advantages of workload monitoring, along with many of the associated controversies.39
An Uphill Battle
Utilizing temporal and criterion-based assessments when making RTS decisions, as well as considering intrinsic and extrinsic risk factors, goes against the grain. It is likely that many physicians, physical therapists, and patients may look unfavorably upon these recommendations. Additionally, the proposed RTS criteria have not yet been validated. While this approach to RTS testing may provide more information than current RTS criteria, it may also be less feasible for some clinicians and patients, considering the additional equipment, training, and time required to execute it. However, the pressures for an athlete to RTS the season following their injury should not permit clinicians to put on blinders and throw clinical reasoning out the window. Instead of focusing on getting an athlete back on the field as soon as possible, what if physical therapists were to actively shift the sports medicine culture to focus on long-term athlete health and wellness, as well as athletic viability and performance? What if therapists start seeing post-operative protocols as guides and not rules, cease conveniently simplifying RTS testing to one-dimensional methods that check a box, and instead embrace a holistic approach to evaluating an athlete’s readiness for sport? What if sports medicine providers are transparent enough to arm patients with accurate RTS and retear rates instead of pretending that waiting six to nine months to RTS guarantees success? The authors of this manuscript encourage each clinician to honestly reflect on their current practice patterns for RTS testing. The time is now to push the envelope forward. Please consider joining the movement.
Conflicts of Interest
The authors affirm that we have no financial affiliation (including research funding) or involvement with any commercial organization that has a direct financial interest in any matter included in this manuscript.