


Introduction
Despite recent international consortium1 and clinical practice guideline2 recommendations that ankle dorsiflexion range of motion be targeted during rehabilitation after ankle injury, evidence to guide the clinician regarding the effects of specific interventions remains unclear.3,4 Dorsiflexion range of motion limitation has been identified as a prospective risk factor for a number of lower-limb injuries including ankle injury,5,6 Achilles tendinopathy,7 patellofemoral pain,8 plantar fasciopathy,9 and hamstring injury.10 Additionally, limited ankle dorsiflexion range of motion is associated with impaired dynamic balance11 and increased chronicity1 and recurrence12 in those recovered from lateral ankle sprain. Those with chronic lateral ankle instability display lower dorsiflexion range of motion during gait13,14 as well as drop jumps,15 and presumed compensatory movements in other parts of the kinetic chain.15–18 During rehabilitation from ankle injury, restoration of this range of motion is often identified as an important treatment goal to address impairment.11,19–22
Weight-bearing dorsiflexion range of motion is typically measured as a “knee to wall” distance, or as an angle of inclination of the tibia.23 Previously we have documented normal dorsiflexion range of motion as approximately 35° in an athletic population24 using this measure. Many physiotherapy interventions have been described to improve ankle dorsiflexion range of motion including electrotherapy, ice application, relaxation and imagery programs, passive mobilization, psychological interventions, stretching, and mobilization with movement techniques.4 Manual therapy interventions (joint mobilization, mobilization with movement, and high velocity low amplitude techniques) used on patients with reduced dorsiflexion after ankle injury have shown short-term improvements of 6 to 22mm25–30 and 3.0° to 5.5°31 depending on the intervention and measurement method employed. Stretching interventions have shown short-term improvements in range of 2° to 5.3°32,33 depending on the technique and duration with larger effects seen for two- to six-week home programs.3
Research in this area typically examines single interventions in a pre- post- treatment design considering only the immediate effects of intervention. Multiple applications of joint mobilizations appear to show no further benefit beyond the second application34 although this research is sparse35especially in professional athletes. Clinically, therapists will often employ a number of interventions on any single patient during a single session. It is not known if the addition of further interventions provides greater improvement in range of motion, and it is unusual to have any published information regarding anything other than the immediate effects of such interventions. It is possible that some improvement in range of motion is simply due to either test-retest variability independent of any real gain in flexibility, or test-retest improvement.36 Clinically, therapists will often aim to improve range of motion and then capitalize on this by performing other exercises in this newly acquired range of motion in an effort to provide a more lasting benefit. It is not known if these gains persist throughout the duration of any clinical encounter.
Accordingly, the purpose of this case series was to document the change in dorsiflexion range of motion after stretching and mobilization-with-movement and exercise and a novel manipulation intervention in a population of injured athletes. It was hypothesized that each of the interventions would be associated with an increase in dorsiflexion range of motion.
Methods
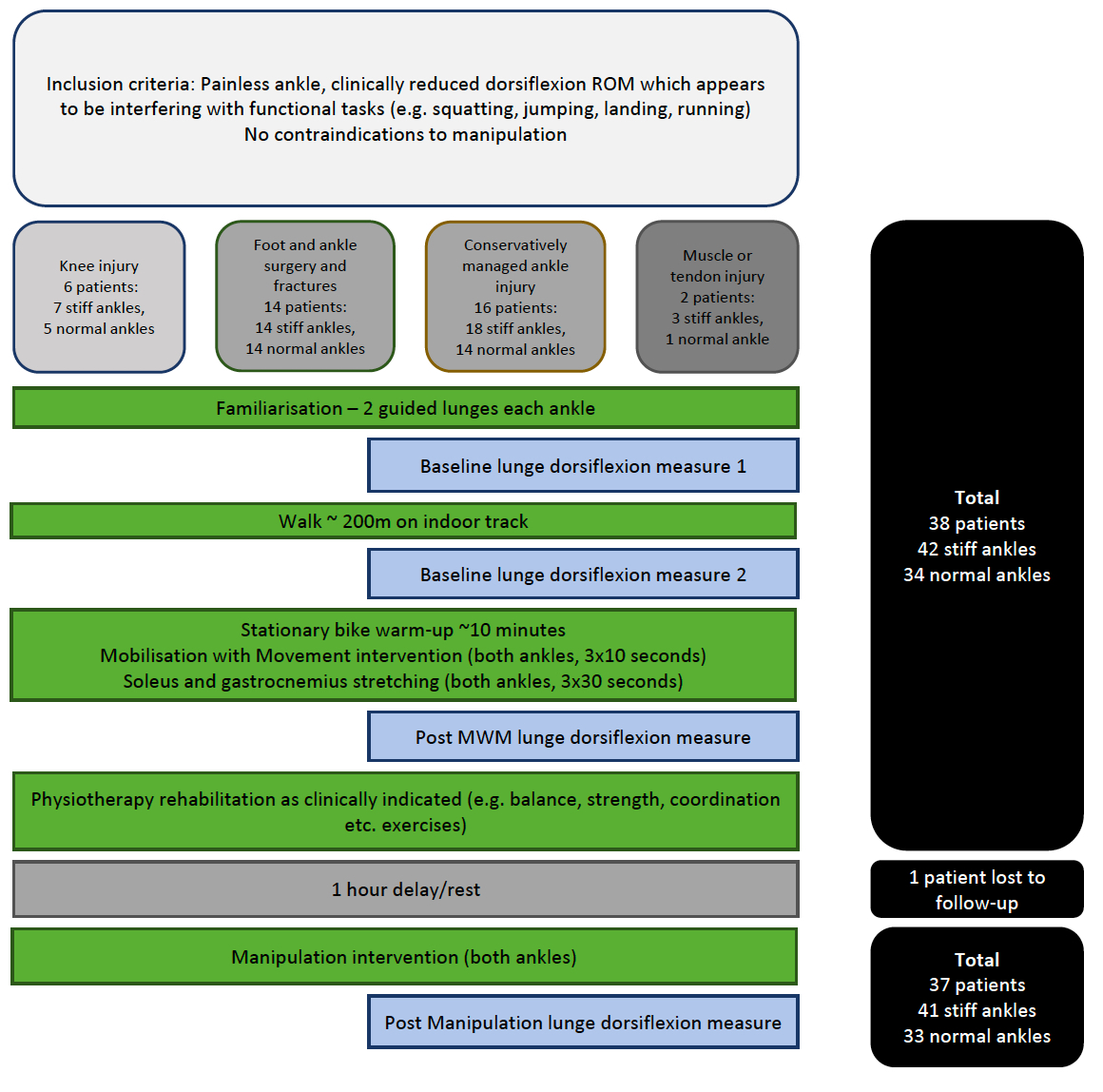
Patients attending an outpatient sports physiotherapy clinic were targeted for inclusion after clinical identification of a relative reduction (compared to the uninjured side) in dorsiflexion range of motion along with one of several features during rehabilitation which suggested the athlete required more ankle joint dorsiflexion to reestablish normal movement under load. These features included observation of excessive pronation on the injured side during a bilateral squat, weight-shift toward the uninjured leg during a heavy squat, off-loading of the injured leg during bilateral jump-landing, reduced distance toward the posterior targets during star excursion balance testing on the injured leg. Four broad categories of patients were examined who had a reduction of ankle dorsiflexion identified as a therapeutic limitation. The first group were athletes at end-phase rehabilitation following knee injury with painless difficulty achieving full range during full squats or unable to land properly from a jump (6 patients with 7 stiff ankles). The second through fourth groups were all pain-free patients being treated for foot (second group), ankle (third group), or posterior lower leg (fourth group) injuries with similarly interfering ankle stiffness whose rehabilitation had persisted for more than 6 weeks (32 patients with 35 “stiff” ankles, Figure 1).

Contraindications for inclusion were medical diagnosis of acute anterior or posterior impingement, imaging-identified cartilage damage, or history of cartilage repair in either the tibiotalar or subtalar joints. Additionally, any patient from either group complaining of an ankle pain during active dorsiflexion, plantarflexion, one leg squat, one leg jump, or one leg hop were excluded.
Pilot investigation suggested that an improvement of approximately 5° (0.5° SD) was possible for this intervention. Thirty-three subjects would give a power of 0.8 to detect such an effect with a Type I error rate of 0.05, therefore we planned to enroll 36 subjects (allowing for data loss). Ultimately 38 consecutive patients met the inclusion criteria in this pragmatic clinical outcome trial. The study was conducted in accordance to the STROBE guidelines for cohort studies,37 informed consent was sought and obtained for the use of these clinical data from the patients, and the study was approved by the local ethics committee (application number: E202009010).
Inter-rater reliability and baseline measurement
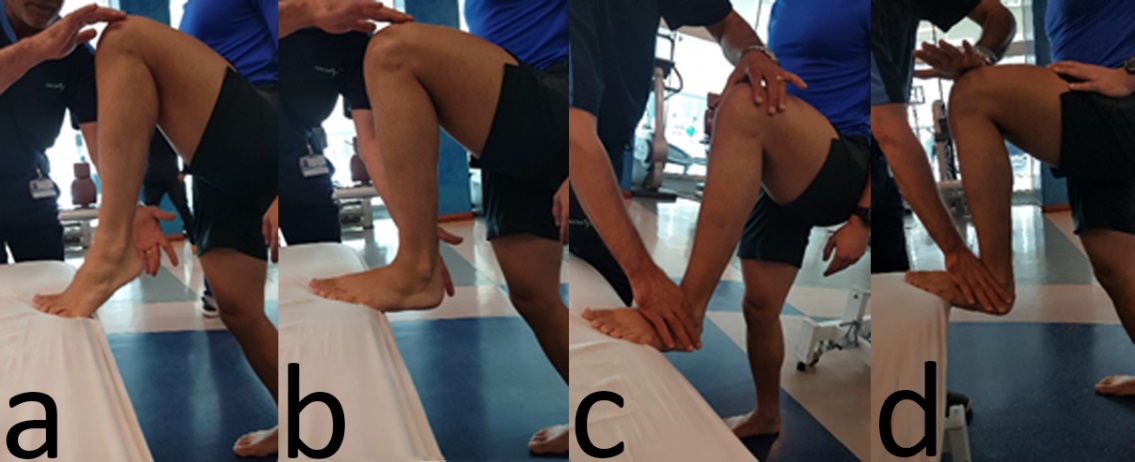
The baseline dorsiflexion range of motion was measured before any treatment or exercise was given at the beginning of the session. The patient started in a lunging position facing a wall, “knee over middle toe” where the pelvis remains parallel to the wall (figure 1). An initial familiarization of two lunges to the limit of dorsiflexion were performed. Subjects were instructed and manually guided, if required, to maintain neutral tibial rotation during these lunges. Two physiotherapists who were blinded to the intervention, injured side(s), and to each other’s measurements recorded the subsequent clinical measurement on each ankle. For the measurement, an inclinometer (Magnetic Polycast Protractor, Empire, USA) was placed 4 fingers width proximal to the ankle joint line on the tibia avoiding the antero-lateral muscular compartment (Figure 2). Two baseline measurements were taken to determine within session inter-rater reliability, with the subject walking approximately 200m between these tests on an indoor track (Figure 2). Inter-rater reliability was assessed using ICC(2,1) (absolute agreement) and the minimum detectable change (MDC) through calculation of the Standard Error of the Measurement from the ICC ANOVA table.38 Statistical analyses were performed using SPSS (v23, IBM Amarok, USA) and R39,40 with the dabest 0.2.2 package.41

Interventions
After a self-paced warm-up on a stationary bike for approximately 10 minutes, the patient had a series of three, 10-second mobilization with movement techniques performed on each ankle (Figure 3) at a rate of 1Hz followed by soleus and gastrocnemius self-stretching for 3 repetitions of 30 seconds each with 10 seconds rest between repetitions (Figure 4). Immediately after this, dorsiflexion measurement was taken by the experimental physiotherapist, blinded to the baseline measurements. The only difference in measurement technique described above is that no familiarization trials were conducted. The patient then continued with their scheduled rehabilitation treatment session. Typically, this session would include a variety of balance, strength, and coordination exercises relevant to the athlete’s sport and their rehabilitation stage. After one hour of rest that followed the end of this session, the athlete was then recalled for a manipulative intervention technique which was applied to both ankles. After this intervention, the dorsiflexion range of motion was again assessed by an independent physiotherapist, blinded to the previous findings in a similar manner to the previous measurements (with no warm-up trials).

Mobilization with movement
The technique utilized incorporated Mulligan principles of applying subtle pain-free overpressure to an end-range movement, or specifically a “sustained passive accessory force / glide to a joint while the patient actively performs a task that was previously identified as being problematic.”42 The patient was supine, foot off the edge of the treatment plinth so that the joint line is about 1 cm away from its edge (Figure 3). A rigid mobilization strap was placed at the level of the joint line its length is then adjusted to be 5 cm from the floor. The belt was folded at its upper part to cover the anterior surface of the talus only (i.e., avoiding coverage of the other tarsals and/or the tibia). The clinician inserted his foot in its lower part to create a downward pressure on the talus. While controlling the stability of the tibia with one hand ensuring full knee extension along the maneuver, the other hand grasping the heel and passively mobilizing the foot from plantarflexion to dorsiflexion. Three sets of 10 consecutive mobilizations with movement are applied with 10 seconds rest between sets.
Stretching
Soleus and gastrocnemius stretching were performed standing on a small (6.5 cm) platform for 3 repetitions of 30-seconds each with 10 seconds rest after each stretch (Figure 4).

Manipulative technique intervention
The manipulation technique (Figure 5) was performed on both ankles without any additional warm-up.

Results
Subject characteristics
Subject characteristics are presented in Table 1. One subject was unable to be measured for the final (post-manipulation) measurement. Sensitivity analysis (imputing these missing data from linear regression) showed no meaningful differences therefore these data were omitted from the final analysis.
Reliability and Minimum Detectable Change
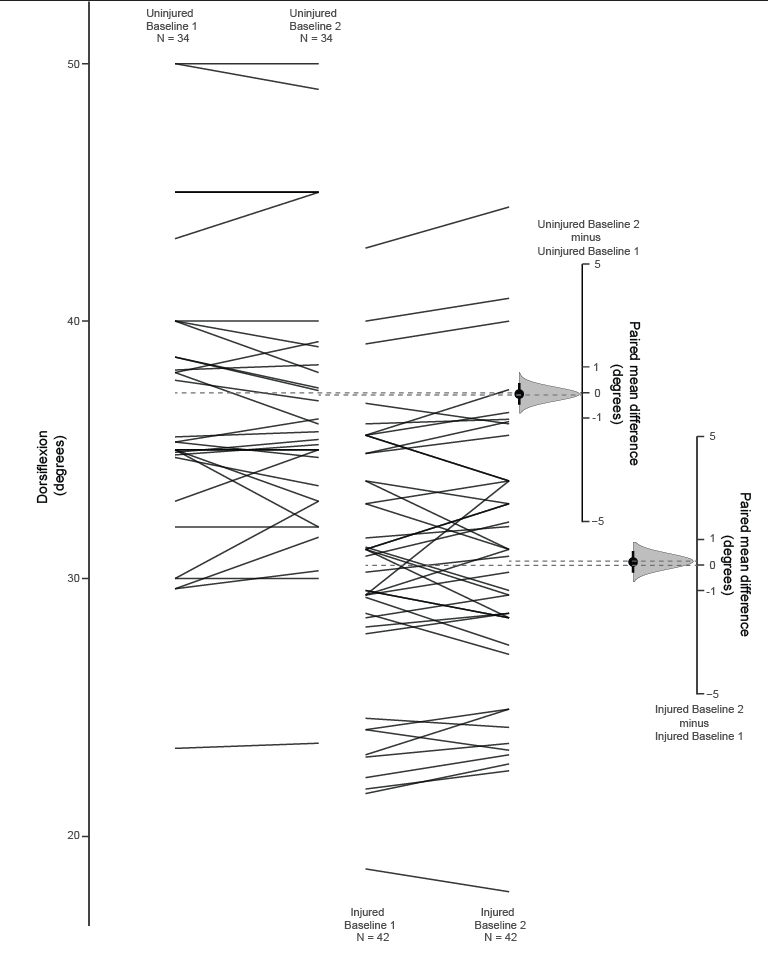
Given the differences in range of motion for the uninjured and injured legs, inter-rater reliability was calculated initially for the injured (ICC2,1 (absolute error) = 0.96, 95% confidence interval: 0.93 to 0.98, p<0.01) and uninjured (0.98, 0.98 to 0.99, p<0.01) legs separately, and then for all legs combined (0.98, 0.97 to 0.99, p<0.01). As these results were essentially the same the pooled (all legs) results are used for calculation of the minimum detectable change which was 3.5°. These measurements and the between group differences are depicted using bootstrap confidence intervals in Figure 6.
Treatment effects
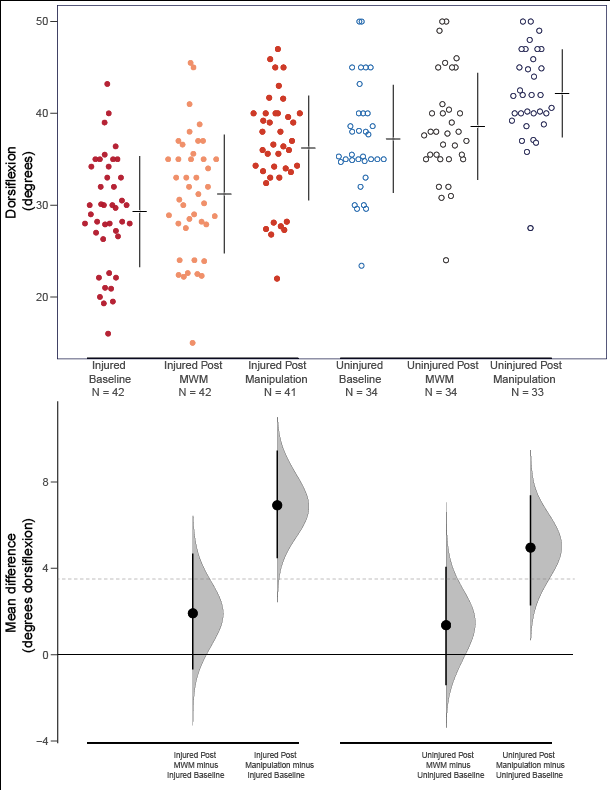
A one-way repeated measures ANOVA was conducted to see if there were statistically significant differences in dorsiflexion range of motion at the three time points (Baseline measurement 1, post-MWM, and post-manipulation) for each of the injured and uninjured legs separately. There were no outliers and the data were normally distributed (visual inspection, Q-Q plots, and Shapiro-Wilk tests). The assumption of sphericity was met for both analyses (injured legs: χ2 = 8.59, p = 0.014; uninjured legs: χ2 = 9.97, p = 0.007). After post-hoc adjustment for multiple comparisons (Sidak) statistically significant differences were seen for dorsiflexion at all time points (p<0.01) except for the two baseline measures. It should be noted however that only the differences between baseline and manipulation for the injured and uninjured legs (6.9° and 4.7° improvement respectively), and injured leg mobilization with movement to manipulation (5.1°) exceeded the dorsiflexion minimum detectable change of 3.5°. These differences are depicted using bootstrap confidence intervals in Figure 7 and Table 2.
Between group comparisons for the baseline (reliability) measures, and the first baseline measure compared to the post-mobilization with movement, and post-manipulation conditions for both the injured and uninjured legs. Note that the MDC for this measurement is 3.5° therefore the only measurements to be considered clinically significant are: the injured leg from baseline to post-Manipulation and from post-MWM to post manipulation, while for the uninjured leg only baseline to post-manipulation reached this hurdle (“MWM”: mobilization with movement).
Discussion
The approach described here documents, for the first time, baseline dorsiflexion range of motion, and test-retest reliability for this measure along with in-session measurements after both a mobilization-with-movement and stretching, and exercise and a novel manipulation intervention. The stretching and mobilization with movement was associated with a likely clinically insignificant improvement of approximately 1-2°, and a further improvement of about 4-5° after the exercise treatment and the novel manipulation technique. The combination intervention appears to largely restore the injured ankle dorsiflexion range of motion compared to the baseline range of the healthy ankle (from 28° to 35° and 37° respectively). Previously we had documented healthy athletes’ weight-bearing dorsiflexion range of motion to be approximately 35° which suggests this combination of interventions is restoring “normal” range of motion in athletes.24 It should be noted however that the uninjured ankle demonstrated an improvement of a similar magnitude compared to the injured ankle. It is not clear if the therapeutic target value of the baseline uninvolved ankle’s range of motion is appropriate, or if clinicians should aim for the “best possible” range available on the uninjured ankle.
The effects of the clinical intervention demonstrated here reflect usual clinical (multimodal) practice. Typically, clinical research will consider only a single intervention performed in isolation which allows for a clearer depiction of such an isolated intervention. This does not reflect usual clinical practice however where multimodal interventions are commonplace during an encounter. The authors’ suggest that this approach may be useful to further tease out aspects of a clinical encounter which contribute to improvements as well as their relative contributions, although future research will need to consider the order of application, more frequent measurements, the longer-term maintenance of these ranges of motion, and whether these improvements in flexibility transfer to daily activities.
The actual anatomic effects of the interventions cannot be inferred from this research. While some researchers ascribe treatment benefits to changing joint mechanics others suggest combinations of soft tissue relaxation and/or stretch tolerance are more important factors.6,43–50 The data presented here suggests that stretch tolerance is less likely to be a major contributor to the improvements seen given the two baseline measures remained essentially unchanged however beyond this we are unable to speculate as to exactly how these ranges of motion are improving. Future work might consider muscle tone, tissue compliance, and arthrokinematics as potential sources of the improvements seen.

To the authors’ knowledge, there is little research describing within-session changes in populations of ankle injured athletes with reduced dorsiflexion undertaking typical multimodal rehabilitation. Serial changes after repeated application of the same (mobilization) intervention34 or the results of complete heterogenous treatment approaches are more commonly reported.3,51 These approaches do not allow understanding of the different components of usual multimodal interventions and require different research methods.52
Importantly, the changes seen here are only documented within the session, in a static measurement, not during gait or other athletic tasks. Future research should examine the time course of these changes, specifically how long changes persist in the absence of further intervention, and whether these static improvements in flexibility are associated with altered kinematics and kinetics during functional tasks such as running, jumping, and direction change. These limitations notwithstanding, the previously documented association of reductions in dorsiflexion range of motion with adverse outcomes make the current findings likely of interest to clinicians and researchers alike.
Clinical Implications
The multi-modal intervention presented here resulted in potentially clinically important improvements in ankle dorsiflexion range of motion in a population that had failed to show sufficient improvement in this rehabilitation goal. Incremental improvements were seen with both the mobilization with movement and stretching, and subsequent exercise and manipulation interventions. Clinically, the authors have noticed this combination of treatment interventions to show larger effects than any single intervention in the management of ankle dorsiflexion range of motion deficit. While we might attribute short-term improvements in flexibility to the application of manual therapy techniques, clinicians should consider the possibility that the exercise interventions may have contributed to these improvements when applied in combination with these techniques. The order of applications as well as the dose and the grade of the manual therapy techniques (repetitions and force applied) and exercises should be investigated in future research.
__post-str.png)
Limitations
Due to the nature of the clinical setting, this research was conducted only on adult male professional athletes; extrapolation to adolescents, females, and non-athletes should be done with care. As we only measured dorsiflexion range of motion four times during each session, we are unable to describe the independent effects of the exercise and manipulation interventions performed, nor the possible effects of a sham intervention. Future research could address this limitation but would need to control for differences in exercise prescription and baseline characteristics of the patients. The longer-term effects of these interventions were not documented need to be investigated in future research.
Conclusion
A combination of a mobilization with movement, exercise and stretching, and a novel manipulation induced changes in weight-bearing ankle dorsiflexion which were likely clinically meaningful. These represent relatively simple interventions which can be safely applied clinically for patients with persisting restrictions in ankle dorsiflexion. Future research needs to describe how long these changes are maintained, and if these changes are associated with other functional improvements such as performance and re-injury risk.
Conflicts of Interest
The authors state no conflict of interest perceived or actual in the creation of this research.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.