

INTRODUCTION TO PELVIC TILT
Assessment of the position and mobility of the pelvis may be relevant for a variety of conditions that a physical therapist might encounter, particularly musculoskeletal conditions of the lumbar spine,1,2 pelvis,3 hip,4,5 and knee.6 This is thought to be due to the interrelationship between the pelvis and adjacent segments of the body during movement.7 Assessment of pelvic tilt has long been a part of physical therapy practice,8 and the relevance of pelvic tilt has become increasingly studied in laboratory-based biomechanical4 and in surgical research.9 Compared to biomechanical and surgical research, there is comparatively less description or interpretation of clinical measures of pelvic tilt that are practical in a rehabilitation setting.
There are several definitions used to describe pelvic tilt.4,8,9 For the purposes of planning surgical interventions, pelvic tilt is assessed statically via plain radiographs, with several different descriptions existing without a consensus gold standard.9 In research, ‘pelvic tilt’ is usually describing the position or movement of the pelvis in the sagittal plane, but is occasionally referred to as movement of the pelvis in the frontal plane.10,11 In the physical therapy setting, pelvic tilt typically refers to the angle formed from a horizontal line and a line bifurcating the anterior superior iliac spine (ASIS) and posterior superior iliac spine (PSIS) in the sagittal plane.8,12 It is commonly assessed in a static manner, such as the pelvic tilt of an individual in a relaxed standing position. It is also sometimes assessed in an active manner, such as the ability of an individual to actively move through as much pelvic motion as possible in an upright position. It may also be assessed during a functional movement, such as the change in pelvic tilt angle during a step-down task. While there are different descriptions of pelvic tilt, for the purposes of this commentary pelvic tilt refers to the spatial position or motion of the pelvis in the sagittal plane about a horizontal frontal axis. Anterior pelvic tilt is when the ASIS is either lower than the PSIS in the sagittal plane (position) or rotating inferiorly relative to the PSIS (motion). Posterior pelvic tilt is when the ASIS is higher than the PSIS in the sagittal plane (position) or rotating superiorly relative to the PSIS (motion).
Muscle tone,13,14 pain,15 bony morphology,4,16 and altered mobility at adjacent locations14,17,18 all have the potential to influence pelvic tilt. With many potential influencing factors, there is considerable variability in pelvic tilt among asymptomatic individuals. Using radiographic analysis, Vialle and colleagues19 demonstrated an average of 13 (+/- 6) degrees of anterior pelvic tilt with range of -4.5 - 27 degrees of anterior pelvic tilt in asymptomatic adults. Nguyen and Shultz20 performed a similar study using a caliper-based inclinometer, and measured standing pelvic tilt on both the right and left side of healthy subjects. In healthy male college students, they found an average of 8.6 +/- 4.2 and 8.7 +/- 4.0 of anterior pelvic tilt on the right and left side, respectively. In healthy female college students, they found an average of 12.2 +/- 5.2 and 11.8 +/- 4.5 degrees of anterior pelvic tilt on the right and left side, respectively. Also using a caliper-based inclinometer, McKeon and Hertel21 assessed healthy active adults and collegiate athletes and found an average of 9.6 +/- 3.5 and 11.7 +/- 3.8 degrees of anterior pelvic tilt with a range of 3.0-18.0 and 2.0 – 19.0 in males and females, respectively.
THE RELATIONSHIP BETWEEN PELVIC TILT, HIP FUNCTION AND PATHOLOGY
With laboratory measures, changes in pelvic tilt have been correlated with several musculoskeletal conditions, including conditions related to the lumbar spine,1,2 pelvis,3 and knee,6 but most notably in regards to conditions affecting the hip. At the hip joint, differences in pelvic tilt are correlated with symptomatic femoroacetabular impingement (FAI)4,22 and non-specific groin pain15,23 as compared to asymptomatic controls. Differences in pelvic tilt in subjects with a symptomatic hip have manifested during kinematic assessment of a variety of basic functional movements, such as walking,24–26 a single leg step-down,17,27 and squatting.28 Significant differences of pelvic tilt during athletic activities such as cutting have also been identified in populations with a symptomatic hip condition.23 The majority of these studies demonstrate either a reduction in posterior tilt or an increase in anterior tilt in symptomatic patients with hip and/or groin pain,17,23,25–28 with one study identifying reduced anterior tilt in patients with symptomatic FAI.24
Across all of these studies there is some variance regarding whether symptomatic individuals demonstrate an increase or decrease in pelvic tilt, and to what magnitude. It has been proposed that altered pelvic tilt in individuals with FAI could be contributing to an increase in symptoms,29 such as during performance of a squat maneuver28 or a step down27 with increased anterior tilt. These scenarios would initiate earlier impingement at the hip joint5 which could potentially exacerbate symptoms. In other cases, altered pelvic tilt could be an adaptive maneuver to avoid symptom-producing mechanics, such as an individual with FAI reducing the amount of anterior pelvic tilt during walking to increase the available amount of motion at the hip.24 The reasoning behind the differences in pelvic tilt in persons with symptoms are unclear and likely diverse among different populations.4 Indeed, differences have been found in pelvic kinematics in males and females following hip arthroscopy, with increases in anterior pelvic tilt during walking evident only in females compared to healthy controls after at least 1 year post-arthroscopy.26
Alterations in pelvic tilt have been found to influence clinical hip range of motion measurements.5,30–32 In particular, anterior pelvic tilt has been shown to reduce the available range of motion at the hip until impingement occurs,5 and may contribute to range of motion losses that are sometimes seen in patients with symptomatic femoroacetabular impingement.32 Because of the ability of pelvic tilt to affect the available functional range of motion at the hip, it has been proposed that specifically assessing and targeting modifiable factors that affect pelvic tilt during rehabilitation may be of benefit.5,32–35
In addition to being associated with musculoskeletal pathology and hip range of motion, pelvic tilt may influence other objective measurements and common physical therapy interventions as well, regardless of the location of symptoms or pathology. Changes in pelvic tilt have been found to influence the muscle activation during assessment and common exercises at not only the hip and pelvis,36–38 but also the lumbar spine39 and even the shoulder girdle.40
CLINICAL MEASURES OF PELVIC TILT
In contrast to laboratory measures of movement, there is less information available to describe clinical measures of pelvic tilt common in physical therapy practice. In the rehabilitation setting, there is no consensus on the optimal method of assessing pelvic tilt. The most commonly described ways of assessing pelvic tilt in an outpatient rehabilitation setting include: visual assessment;41,42 use of a hand-held inclinometer;43 use of a specific caliper-based inclinometer,20,21,44–47 and use of a smartphone application.15,48 Table 1 summarizes the available research on the validity and reliability of each of these options. Each of these are described in more detail below.
Visual assessment is commonly described in physical therapy examination textbooks.41,42 The patient stands in a relaxed stance position, and the practitioner observes from the side. The practitioner visually observes the angle formed by an imaginary line bifurcating the ASIS and the PSIS. The resting posture is compared to a predefined “normal” posture. The practitioner can palpate the aforementioned bony landmarks in attempt to confirm their assessment. The ASIS being lower than the PSIS in the sagittal plane is defined as an “anterior pelvic tilt,” and the ASIS being higher than the PSIS in the sagittal plane is defined as a “posterior pelvic tilt.” If they are level, it is defined as “neutral.” There have been no known attempts to assess the reliability, validity, or clinical usefulness of this method. Visual assessment of lumbar lordosis, a postural measure in close proximity and directly related to pelvic tilt49 has fair intrarater reliability and poor inter-rater reliability.50
Use of a hand-held inclinometer to assess pelvic tilt has been described.43 To assess pelvic tilt, the practitioner aligns the inclinometer in the sagittal plane and places it firmly on the sacrum. The angle is interpreted as the amount of pelvic tilt, with higher numbers corresponding to greater anterior pelvic tilt and vice versa. When assessing anterior, posterior, and total pelvic tilt in males and females, reliability has been found to be moderate to excellent (ICC: 0.60 – 0.94).43 There have not been any studies on the validity for assessing pelvic tilt with a hand-held inclinometer as compared to a gold standard or identification of normative values.
More recently, applications that utilize the inclinometer functions within a smartphone have been developed and used to assess pelvic tilt. The device is used and interpreted in the same fashion as a hand-held inclinometer and demonstrates excellent (ICC= 0.97) intra-rater reliability.48 Van Goeverden and colleagues15 identified significant deficits in active pelvic tilt in athletes with groin pain using a smartphone application, although it should be noted that they used an alternative method which involved placing the smartphone in a strap that is secured around the subject’s waist.
Caliper-based inclinometers, described as pelvic inclinometers, have been developed to specifically assess pelvic tilt. Pelvic inclinometers have adjustable arms to facilitate direct contact with the bony landmarks in question. To assess pelvic tilt, the clinician aligns the adjustable arms with the ASIS and PSIS. This is most often described with the subject in a relaxed standing position. Crowell and colleagues44 demonstrated excellent reliability (ICC: 0.95-0.99) and validity (ICC:0.93) with a pelvic inclinometer as compared to a roentgenographic measure. Subsequent devices have been developed which are comparable in physical construct, such as the digital pelvic inclinometer (DPI, Sub-4 Limited, UK) and the palpation meter (PALM, Performance Attainment Associates, St. Paul, MN). The digital pelvic inclinometer has good inter-rater (ICC: 0.81-0.88) and test-retest reliability (ICC: 0.88-0.95) within a session, and moderate-to-good reliability between sessions (ICC: 0.65-0.85).45 The palpation meter has been demonstrated to have good to excellent intra-rater (ICC: 0.87 and ICC: 0.98)46,51 and good interrater reliability (ICC: 0.89).51 It also has demonstrated acceptable validity when compared to radiographs for assessing the amount of anterior pelvic tilt and total amount of pelvic tilt.47 Normative values for pelvic tilt using the palpation meter show a significant degree of variance among asymptomatic populations with the majority of individuals presenting with some degree of anterior pelvic tilt.20,21,46
DISCUSSION
Laboratory-based studies describe alterations in pelvic tilt associated with several common musculoskeletal conditions during a variety of functional and athletic movements. There are comparatively much fewer attempts to identify differences in clinical measures of pelvic tilt when comparing symptomatic to asymptomatic individuals, despite the historical usage of such measurements. The vast majority of available research on clinical measures of pelvic tilt is on healthy subjects. There is a large gap between what available research suggests and current physical therapy practice standards. This may cloud clinical decision making.
While it is not known what the most frequent methods of assessing pelvic tilt are in a practice setting, anecdotally it is the author’s perspective that visual observation is commonly utilized. Visual assessment of pelvic tilt is typically subjectively interpreted on a three-point categorical scale: “posterior pelvic tilt,” “neutral,” or “anterior pelvic tilt.” Because of the variance among normal asymptomatic populations, with the majority of asymptomatic individuals presenting with some degree of anterior pelvic tilt,19–21,46 use of this rudimentary scale may lead to misguided clinical decisions. This is further confounded by the fact that kinematic assessment of functional movements shows a precise quantifiable difference in the quantity of pelvic tilt (example: a 5 degree difference in the amount of anterior pelvic tilt between symptomatic and asymptomatic populations).15,23–28 This is in contrast to an absolute categorical difference (example: anterior pelvic tilt, neutral, or posterior pelvic tilt) which is how visual observation is interpreted. Further, variations in the pelvic morphology within a normal population may further confuse a simple visual or manual assessment.16 Visual assessment of pelvic tilt may not only be overly simplistic but may be especially prone to inaccurate clinical interpretations given the subjectivity.
Assessment of pelvic tilt using an inclinometer, whether it is hand-held, caliper-based, or smartphone application based, allows for increased precision. In addition to using an interval scale, this also reduces the subjectivity of the measurement and may be more sensitive to measure change over a treatment plan.46 These measurements have shown moderate-to-excellent reliability.45,46,51 Caliper-based inclinometers have established validity for assessing the degree of anterior pelvic tilt and the total amount of pelvic tilt.44,47 With the currently available evidence, inclinometers may be a better option for assessment of pelvic tilt due to acceptable reliability and validity, as well as the enhanced precision for measurement that might be needed to identify relevant changes. For caliper-based inclinometers only, there is normative data available which may add additional value, although these values are variable which may limit the clinical usefulness.20,21,46
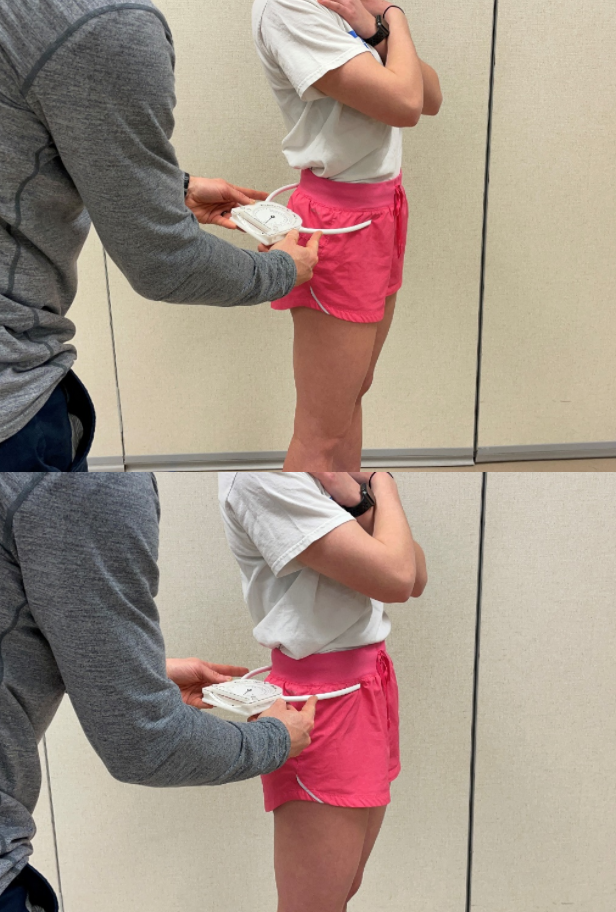
There is scarce research using any of these clinical measures to assess pelvic tilt on clinical populations. With this consideration, there are additional and more fundamental questions that have not yet been addressed. There is a poor and inconsistent link between basic static standing measurements and symptoms at the knee,52 lumbar spine,53 and shoulder girdle.54 The lack of clinical usefulness for static standing measurements elsewhere in the body raises doubts that assessing static standing pelvic tilt will add any clinical value regardless of the accuracy. Active pelvic tilt may offer more value as differences in pelvic tilt in symptomatic individuals seem to manifest during active tasks. As there are multiple potential limiting factors for active pelvic tilt, consideration of the symptom-provoking positioning or individual functional limitations when determining the best position of measurement may be beneficial. Active pelvic tilt can be assessed in the traditional standing position (Figures 1A and 1B),47 or in a position that may be closer to mimicking positions of function,15 such as a split stance position (Figures 2A and 2B).


Despite many studies finding significant differences in pelvic tilt during laboratory-based assessments of functional movements in symptomatic individuals, it is not known if there is a correlation between kinematic movement assessments and of the use of a basic clinical measure with an inclinometer during basic static or dynamic standing posture. Very limited research suggests that there may not necessarily be a relationship between measurements at the pelvis during simplified clinical measures and more athletic movements.55 Assessment of pelvic tilt during functional activities specific to the patient, provided it is done in a precise manner using validated and reliable measures may be most useful. The diagnosis, the biomechanics, when symptoms occur, and the performance goals are all worthy of consideration. Measuring the amount of pelvic tilt that occurs during a functional motion can be considered, such as assessing the amount of pelvic tilt during a step down with a smartphone-based inclinometer (Figure 3). This method is not be practically feasible for challenging or athletic movements. For example, as one part of an expanded understanding of the individual and the entire movement system, it may be beneficial to assess anterior pelvic tilt occurs during terminal stance of high-speed running for an athlete recovering from an anterior hip or groin injury, as reduced anterior pelvic tilt may lead towards increased tensile loading to these structures in this task. Conversely, adequate posterior tilt during terminal swing of high speed running may be of great interest for an athlete recovering from FAI or a hamstring injury, as reduced posterior tilt may lead towards earlier impingement in the hip joint and greater tensile loading on the posterior hip muscles. These are both active processes that require complex dynamic movement and control from the patient, and an understanding of the total task-specific pelvic tilt may be most clinically useful. A valid and reliable 3-D motion capture analysis system may be required if the goal is to understand pelvic excursion during high-speed athletic tasks due to the nature of the movement and precision required. This may not be practical for smaller clinics with a limited budget based upon currently available options.

There is limited research demonstrating an association between improving pelvic tilt during sporting maneuvers and a successful recovery from a musculoskeletal injury.56 It is not clear if the change in pelvic tilt leads to the reduction in symptoms or the other way around. It is also not known what interventions, if any, can be attributed to the change in pelvic tilt. Increased hip extensor strength is correlated with improved pelvic mobility during functional tasks which may suggest a potential intervention target.57 Core muscle function has also been associated with the ability to control pelvic tilt.38 Improving hip flexor flexibility has also been proposed as a target, although limited research suggests that addressing hip flexor flexibility in isolation does not lead to carryover in functional tasks.58 Training specific movements with improved pelvic motor control may be of benefit,23,59,60 however generalized strength and flexibility interventions may produce similarly beneficial patient-reported outcomes60 and more research is needed in this area. While there are several potential targets, it is not established if pelvic tilt can be changed because of a specific or generalized rehabilitation plan, or if specifically tracking the change in pelvic tilt might be a useful prognostic factor for a successful outcome.
In consideration of the limitations, the physical therapist or other rehabilitation clinician may consider assessing pelvic tilt in order to individualize assessment and treatment. There appears to be some variability among those who are symptomatic and not, with some presenting with a pelvic tilt that theoretically could be contributing to an increase in symptoms and some presenting with a pelvic tilt that may reflect an adaptive movement strategy to reduce symptoms.4 Assessment of pelvic tilt may be best performed in a manner that has the potential to capture the subtle differences between symptomatic and asymptomatic population, and for this reason visual assessment alone would not be helpful to guide clinical decisions. Caliper-based pelvic inclinometers offer a valid, reliable, and precise measurement and may be a superior option, although the full clinical usefulness is not known and the practicing clinician should apply critical thought with interpretation. Comparisons may be best limited to within-subjects only, as opposed to a predefined normal value, due to variability between subjects in a normal asymptomatic population.19–21,46 A clinician should consider standardization of how they measure pelvic tilt due to pelvic morphology potentially skewing results if different sides are compared.16,46 Measuring active pelvic tilt and pelvic tilt during a movement specific to the patient’s presentation may be more useful.15
CONCLUSIONS
Having a basic appreciation for pelvic tilt may be of benefit to the physical therapist, particularly for conditions related to the hip. Despite the importance of understanding pelvic tilt, there are some inherent limitations in the currently available methods for assessing pelvic tilt in the rehabilitation setting that bring caution to clinical interpretations. Further research investigating assessment methods should seek to identify any relationship of basic clinical measures of pelvic tilt to patient-specific functional movements, investigating clinically feasible methods of accurately assessing pelvic tilt during functional movements, the responsiveness to treatment, and the relevance of clinical assessment of pelvic tilt for a successful recovery.
Conflicts of Interest
The author reports no conflicts of interest.
Acknowledgements
The author would like to thank Margaret O’Neil for her contribution to the figures.