
Introduction
Despite positive clinical results, failure after rotator cuff repair is common, with the large majority of these occurring within the first six months following surgery.1 A successful outcome after surgery is dependent on a myriad of factors, including the quality of repair tissue, pre-operative tear size, the repair technique and individual patient factors such as smoking, body mass and physical activity.2,3 Post-operative rehabilitation is also one of the more important factors in determining a successful outcome, with exercises aimed at restoring glenohumeral motion often utilized within the first post-operative month.4 Current expert consensus states that rehabilitation after rotator cuff repair should include a two-week period of strict immobilization followed by a staged introduction of range of motion (ROM) activities, initially with protected, passive ROM (PROM) exercises to six weeks, followed by restoration of active ROM (AROM).5 However, the time in which certain exercises may be implemented, and progressed from PROM to AROM has been debated. This is especially important during the early post-operative stages, where loading should not exceed the biomechanical limits of the healing tissues, while still facilitating the alignment of newly formed collagen fibers.6
Deciding on which exercises to prescribe in these first six weeks following repair is largely based on clinical opinion and patient feedback, with limited evidence regarding whether a particular exercise may be adversely loading the repair tissues. Muscular activity measured by electromyography (EMG) remains the best available direct estimate of stress placed on the rotator cuff tendon, to guide clinicians through appropriate exercise selection following cuff repair.5,7 In the earlier post-operative stages, a better understanding of how commonly employed PROM and active-assisted ROM (AAROM) exercises specifically load the rotator cuff would be of benefit to the therapist prescribing these activities to patients. The purpose of this study was to investigate EMG activity of the rotator cuff and deltoid musculature during PROM and AAROM exercises commonly performed in post-operative rehabilitation.
Methods
Participants
A total of 16 physically active healthy volunteers (11 males, 5 females) with normal shoulder examination, no previous shoulder injury, and no pain with activities of daily living were recruited for this study. Participants were recruited using flyers on community notice boards and on social media platforms. Inclusion criteria for the study included participants 18 to 40 years of age, no previous shoulder injury or surgery to the dominant arm, no current shoulder pain, and the ability to demonstrate full active shoulder ROM. The study received approval from the University of Western Australia Human Research Ethics Committee (HREC), and all participants provided written informed consent prior to their study participation. This study conforms to all STROBE guidelines and reports the required information accordingly.
Instrumentation and Electrode Insertion
Participants attended a single two-hour EMG testing session, whereby electromyographic data were collected simultaneously from six muscular locations around the dominant shoulder, using a combination of surface and indwelling fine-wire electrodes. A 16-channel telemetry EMG system (Myon 320, Myon AG, Zurich, Switzerland) sampling at 4000 Hz was used to record muscle excitations. The anterior deltoid, middle deltoid, and posterior deltoid were assessed with disposable, self-adhesive pre-gelled surface EMG electrodes (3M, Minnesota, USA), and placed on participants as described by Basmajian and De Luca.8 Electrode placements were confirmed by visualization of the EMG signal during active muscle activation, and all transition cells were secured with adhesive tape. Prior to electrode placement, the area was scrubbed with an abrasive sponge, then cleaned with isopropyl alcohol to reduce skin impedance. Intramuscular fine-wire electrodes were used to record muscle excitations of the supraspinatus, infraspinatus, and subscapularis. Using aseptic technique, the skin was prepared using a chlorohexidine solution. Intramuscular fine wire electrodes were inserted via a sterile 30 mm, 27-gauge hypodermic needle with a pair of 0.051 mm, insulated, bent end Teflon coated stainless steel wires and 200 mm tail with 5 mm bare-wire terminations (Chalgren Enterprises, USA) in accordance with the protocols described by previous studies.8–10 All electrode insertions were performed by a trained medical professional experienced in the practice. All fine wire insertions were guided by real time ultrasound (Telemed Echo Blaster 128 EXT-1Z, TELEMED Medical Systems, Italy). The ultrasound unit was also used to confirm electrode placement, in concert with visual inspection of live EMG time traces during isometric contractions.
Experimental Protocol
Prior to the commencement of data collection, participants were instructed to complete a brief warm-up by moving their arms through full active flexion and abduction ROM to ensure that the intramuscular electrodes had settled into position within the muscle, and the signal from each muscle was adequately detected. All participants underwent a familiarization session approximately one to two days before testing. During these sessions, each participant was given verbal and visual instruction of each exercise from a qualified Exercise Physiologist, upon which they subsequently practiced the exercise techniques and maximal voluntary isometric contraction (MVIC) protocols that will be discussed later.
Exercises
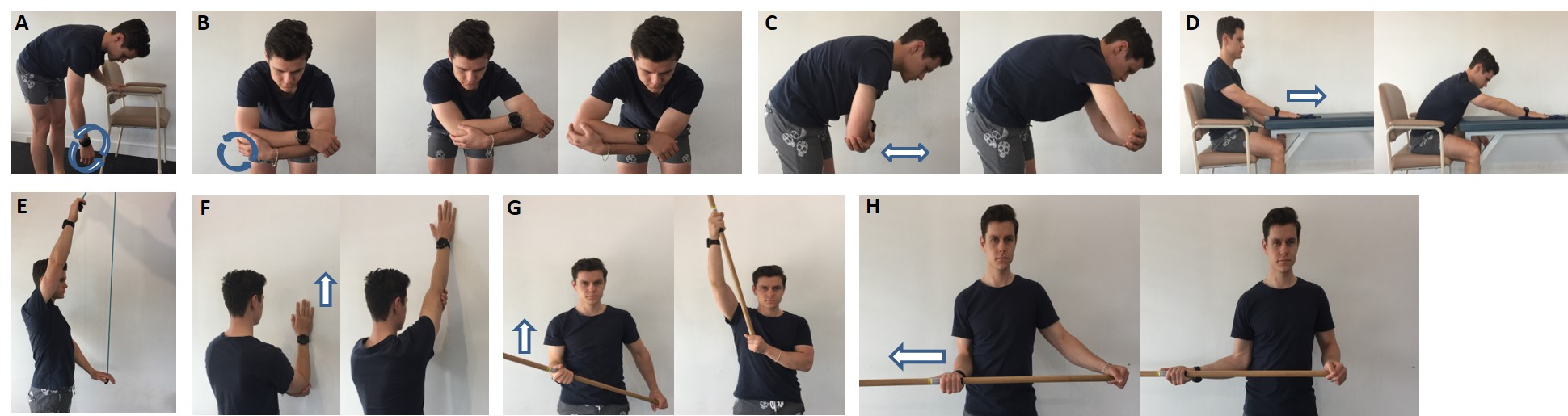
Eight ROM exercises, including four PROM and four AAROM, that are commonly prescribed during early rehabilitation following rotator cuff repair were included for evaluation in this study (Table 1, Figure 1). Active arm flexion and abduction were also evaluated against gravity to serve as a comparison with the PROM and AAROM exercises (Table 1, Figure 1). One set of six repetitions for each exercise was performed. A metronome was used to control arm speed, following a cadence of 15 beats per minute. Previous EMG studies have evaluated exercises at a speed of 60 beats per minute,11,12 while Gaunt et al13 in their study of active-assisted shoulder exercises, evaluated exercises at a speed of 30 degrees per second (approximately five beats per minute). Participants were given a 30 second rest between each trial to reduce fatigue effects. The order of these exercises was performed in a randomized fashion between participants to prevent order effects.
Maximal Voluntary Isometric Contraction (MVIC)
Prior to the exercise testing session, participants were instructed to perform a series of three MVICs, across a total of four muscle tests (Table 2). The four MVIC positions tested in this study have been previously reported (Table 2).9,14 Each contraction lasted for approximately five seconds, with a gradual increase of contraction strength over one second, sustained maximum contraction for three seconds and a gradual release over the final second. To reduce the effects of fatigue, each MVIC trial was performed three times for five seconds, with a three-minute rest between each trial. The highest value from the middle one-second interval of each MVIC trial was recorded for each portion of each muscle.
_pendulum__(b)_rock_the_baby.jpeg)
Data Processing and Analysis
For surface and fine wire EMG data processing, a customized software platform in MATLAB (2009a, The Math Works, Inc., Natick, Massachusetts, USA) was employed, following SENIAM standards.15 For both the fine wire and surface EMG data, direct current offsets were removed. For the surface EMG data, a fourth-order, zero-lag bandpass digital Butterworth filter between 20 and 500 Hz was used. For the fine wire EMG data, a fourth-order, zero-lag bandpass digital Butterworth filter between 20 and 750 Hz was used. Both the surface and fine wire EMG data were then full-wave rectified and then linear enveloped by low-pass filtering with a zero-lag fourth-order Butterworth at 6 Hz. All data were then normalized to each muscle MVIC and expressed as a percentage MVIC (%MVIC). For the analysis of the surface and fine wire EMG outputs, R language (R Core Team, version 3.6, Vienna, Austria) and RStudio (version 1.2.1335, RStudio Team RStudio, Inc., Boston, MA) were used. For each condition (i.e., exercise), the first and sixth repetition were discarded from analyses, leaving four repetitions for each condition. The peak muscle activation (%MVIC) from each of the four trial was obtained, then averaged for each individual participant, which is consistent with previous methods to obtain a %MVIC.13 An ensemble average across all participant’s mean peak muscle activations were then calculated for each muscle and condition.
Data Analysis
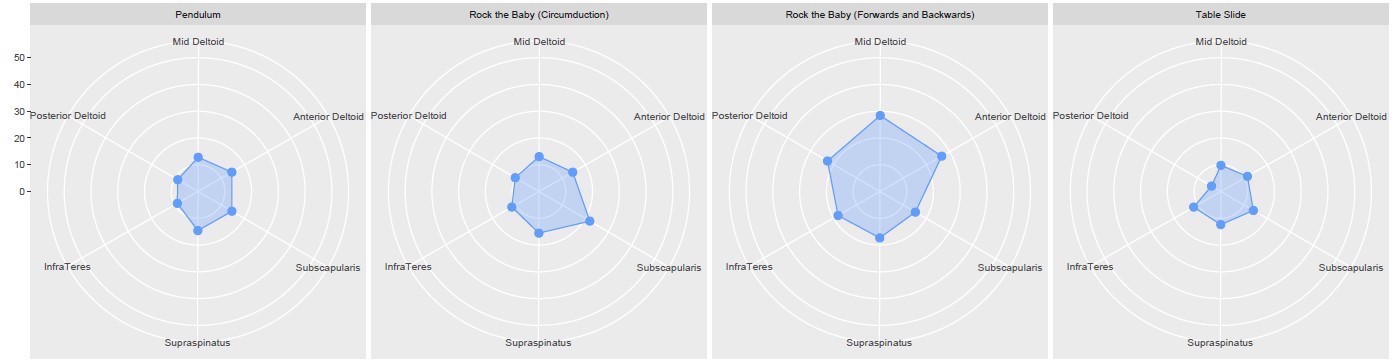
Descriptive statistics are reported and displayed for each individual muscle as mean ± 95% confidence intervals. Maximum EMG expressed in %MVIC values for each muscle were averaged for the participant’s three trials. Muscle activity was categorized as low, 0% to 15% MVIC; low to moderate, 16% to 20% MVIC; moderate, 21% to 40% MVIC; high, 41% to 60% MVIC; and very high, greater than 60% MVIC.7 Descriptive statistics and radar plots for each condition were presented.
Results
The mean (± SD) age, height, and weight for the entire group was 28.5 ± 4.6 years, 1.75 ± 0.10 m, and 75.9 ± 13.8 kg, respectively. Table 3 shows mean %MVIC values and 95% confidence intervals for the supraspinatus, infraspinatus, subscapularis, and deltoid muscles according to exercises performed, ranked from least to the most amount of activity generated. Specifically, for the supraspinatus, the standard pendulum, and gravity-minimized exercises, such as the table slide and assisted wall slide, were the only exercises to generate low-levels of activation (i.e., below 15% MVIC). Interestingly, the rock-the-baby exercises recruited the shoulder muscles to a greater extent than that of the standard pendulum exercise; especially the elevation version of the exercise which consistently generated moderate levels of activity.
Figures 2 and 3 present radar plots visualizing comparisons between evaluated muscles in terms of muscle activation expressed as %MVIC during the four PROM (Figure 2) and four AAROM (Figure 3) exercises.
Discussion
The main finding of the current study was that clear differences were observed between active and assistive (PROM and AAROM) exercises for the anterior deltoid and supraspinatus, but not for the infraspinatus or subscapularis. However, a clear distinction between PROM and AAROM exercises could not be identified. Furthermore, the majority of PROM and AAROM exercises (apart from the pendulum exercise, table slide exercise and the supported vertical wall slide) all exceeded the 15% MVIC threshold, which has been suggested as an upper limit of a safe loading range during exercises in the early stages following rotator cuff repair.16 As such, many of the exercises evaluated in this study, and their use in the earlier stages of a rehabilitation continuum to regain active motion should be questioned, and moreover, subdividing exercises into categories of PROM and AAROM may not be necessary following rotator cuff repair. Instead, progression of exercises prior to commencing active motion should be based on factors such as patient comfort, pain tolerance, and available ROM.13
In the current study, active flexion and abduction for the supraspinatus, anterior deltoid, and middle deltoid elicited high mean %MVICs, compared to all assistive (PROM and AAROM exercises) which generated low, low-to-moderate and moderate mean %MVICs. For the infraspinatus, active flexion and abduction was only seen to generate a moderate mean %MVICs, clearly not differentiating between assistive exercises which were also found to generate low, low-to-moderate and moderate %MVICs. This finding is similar to that by Gaunt et al,13 who also observed clear distinctions between assistive exercises (PROM and AAROM) and active exercises for the supraspinatus and anterior deltoid, but not infraspinatus. In the current study, the subscapularis was also found to only generate moderate mean %MVICs, which did not materially differ from more assistive exercises. However, no clear differences were observed between exercises categorized as passive (PROM) or active-assisted (AAROM), which suggests further subdividing assistive exercises into PROM and AAROM exercises based on muscle activity is not necessary to protect the supraspinatus following a rotator cuff repair, nor for scenarios in which deltoid protection is necessary, such as for an open rotator cuff repair.13
_rehab.jpg)

In the current study, the pendulum exercise was one of two exercises considered “passive” which did not generate >15% MVIC in the supraspinatus. The pendulum is a popular exercise amongst therapists, and commonly employed early in rehabilitation to restore shoulder mobility following rotator cuff repair.16 Indeed, the pendulum has been the subject of many EMG analyses which have frequently found it to generate low levels of EMG activity.17–19 The mean %MVIC of the supraspinatus during pendulum exercises in the current study was 14%, greater than that reported by Gurney et al (12%),18 McCann et al (9%),19 and Ellsworth et al (10%),20 though more similar to the large, correctly performed pendulums in the study by Long et al (13.7%).16 In their study, Long et al16 found that large, incorrectly performed pendulums generate moderate levels of supraspinatus muscle activity (18.8%). In what is meant to be a PROM exercise on the shoulder generated by trunk motion, patients often perform this as an AROM exercise by using their shoulder muscles to swing the arm rather than simply allowing it to hang in a relaxed state.16 Given that pendulum exercises are often prescribed as a home exercise, it is possible that patients may incorrectly perform these without proper instruction and supervision, which may potentially overload a newly repaired rotator cuff.
The rock-the-baby exercise is an alternate version of the standard pendulum exercise performed by having the patient control the operated arm with the non-surgical arm, with the goal of protecting the repair from increased stress that the standard pendulum can cause if performed incorrectly. With the non-surgical arm guiding and supporting the surgical arm, the weight of the arm is reduced and, theoretically, reduces the demand on the shoulder musculature. Previous research has supported this rationale of unloading the surgical arm during AROM and AAROM exercises.21 In the current study, it was interesting to note that the rock-the-baby exercise (when performing circumduction) elicited a low-to-moderate mean %MVIC (17%), and a moderate mean %MVIC (22%) when performing elevation on the supraspinatus. This was higher than the mean %MVIC during pendulum exercise reported in this study, as well as others.13,16–18 No previous studies have directly compared this assisted version of the pendulum with the standard pendulum exercise, making comparison to existing literature difficult. However, it is possible that the rock-the-baby produced more muscle activity than standard pendulum exercises were that, despite being unloaded by the contralateral arm, these exercises may have been supported through a larger ROM, generating more muscle activity. This is consistent with the findings by Long et al16 who found that pendulums, when performed in a larger diameter, generated significantly higher mean %MVICs. Future research could look to expand on this research by controlling for small and large diameter versions of this exercise.
The table slide was another exercise below the 15% MVIC threshold which could be considered appropriate to be prescribed in early-stage rehabilitation. The primary concentric phase of the table slide, that is the forward motion of the exercise, moves perpendicular to gravity with the weight of the arm supported and removing a large gravitational burden on the shoulder, subsequently reducing the demand on the shoulder musculature.21 The mean %MVIC of the supraspinatus during this exercise produced similar MVICs to that reported by Gaunt et al (12%),13 yet much higher than those reported in the study by Jung et al (4%).22 It is possible these differences are due to how the exercise was performed. In the study by Jung et al,22 participants were instructed to generate forward movement by flexing the trunk, with the hand passively sliding until reaching an end range. Conversely, in this present study, forward movement was generated preferentially by the shoulder, similar to that by Gaunt et al,13 which may explain the reason for the larger mean %MVICs in the supraspinatus, and also for the infraspinatus and subscapularis. The mean %MVIC of the anterior deltoid and middle deltoid produced similar MVICs to those observed in the study by Cools et al23 (11% and 11.9%, respectively).
The supported vertical wall slide was the only AAROM exercise which did not generate over 15% MVIC. The mean %MVIC of the supraspinatus during this exercise produced similar MVICs to those reported by Wise et al (13%)21 and Gaunt et al (21%).13 This observed low muscle activation is potentially due to unloading and compressive effects of the supporting surface, and possibly due to additional support of the shoulder from the contralateral arm, throughout AROM.21 However, this exercise has conflicting clinical evidence regarding its use in early rehabilitation. It has been suggested this exercise, also known as the wall slide or wall walk, is more appropriately used in later stages of rehabilitation once the patient can actively elevate the arm to at least 130° without pain, to build endurance for active elevation rather than as an assist for improving elevation ROM.5 Mean %MVICs observed for the anterior and middle deltoid were similar to those observed in the study by Cools et al23 (11% and 11.9%, respectively).
Dowels and pulleys are often used by patients to actively assist forward flexion motion so as not to place excessive stress on an early cuff repair. AAROM exercises using a dowel or pulley to elevate the arm were shown to generate over 15% MVIC for muscles of the rotator cuff which is consistent with previous studies, suggesting that their use early in rehabilitation might not be appropriate.13,17,18 The mean %MVIC of the supraspinatus when using a pulley to elevate the arm in the current study (20%) was similar to that reported by Gurney et al (18.5%),18 Gaunt et al (17%),13 and Dockery et al (17.6%),17 all classified as low-to-moderate.
No exercises employed in the current study were found to generate low levels of muscular activation in the subscapularis. This is an important consideration for clinicians working with patients undergoing rotator cuff repair involving the subscapularis, or even in shoulder arthroplasty surgery whereby the release and subsequent repair of the subscapularis tendon is involved. In these cases, clinicians should abide by soft-tissue precautions; so as not to jeopardize the newly repaired tissue. The mean %MVICs in the current study were inconsistent when compared with those reported by Gurney et al.18 In their study, pulley elevation, pendulums and dowel-assisted elevation generated 7.3%, 9.4% and 9.6% median MVIC, respectively; all falling considerably below the low activity threshold.18 Aside from the differences in statistical reporting, the differences observed between the study by Gurney et al.18 and the present study are possibly due to variances in testing procedures. In the current study, peak amplitudes across four repetitions were averaged over three trials to provide a mean %MVIC value, which differs from the study by Gurney et al,18 who reported mean EMG activity values for one repetition (or 10 seconds in the case of pendulums) of a task.
Limitations
Firstly, this study evaluated participants with healthy functioning shoulders in order to obtain an accurate maximal voluntary contraction for comparison. As a result, the activity of the shoulder muscles in healthy participants may not be representative of the activity of individuals with a pathological or post-surgical shoulder. Previous authors have suggested that patients with painful, symptomatic shoulders activate muscles differently and are unable to remain as passive as healthy control subjects.20,24 Therefore, caution should be applied in extrapolating data collected from healthy subjects and applying results to clinical populations. We did have concerns about undertaking such a study in an early post-operative cuff cohort, given the risk of introducing infection and seeking more insight into the specific loading capabilities of each exercise initially.
Secondly, the mean age of the participants in our cohort is younger than the typical patient undergoing rotator cuff surgery. However, the current study sought to initially recruit a cohort with a lower risk of asymptomatic shoulder pathology. Furthermore, many of the participants in the current study were either physiotherapists or exercise physiologists and, therefore, were familiar with most of the rehabilitation tasks which also served to ensure the exercises were performed correctly.
Finally, repair site tension can only be estimated, as EMG is not a direct measurement of the potential damaging force incurred at the site of repair. As a result, EMG studies cannot provide definitive guidelines on ‘‘safe’’ versus ‘‘unsafe’’ exercises applicable to all patients without assumptions regarding the force-EMG relationships, as well as the force levels that will cause damage (or failure) to a repair. Muscle activity level, along with the plane of motion, cyclic loading and the weight and length of an individual’s upper limb, are also likely to affect the tension on the repaired tissue.5,7 While only moderate correlations have been made between muscle tension and EMG activity,25 in the clinical setting, where stress and tension imparted by rehabilitation exercises cannot be measured, EMG evidence does offer a pragmatic method to base the progression of therapeutic exercises on likely stress on the repaired rotator cuff.5,7
Conclusion
The results of the current study indicate that commonly performed PROM and AAROM exercises, with the exception of the pendulum exercise, table slide exercise and the assisted wall slide, all exceeded the 15% MVIC threshold of the supraspinatus. Fifteen percent or below (defined as low activity) has been suggested as an upper limit of a safe loading range during exercises in the early stages following rotator cuff repair.16 A clear distinction between PROM and AAROM exercises could only be identified for the anterior deltoid, and not for the supraspinatus, which suggests that subdividing PROM and AAROM forward flexion exercises based on muscle activity is not necessary to protect the supraspinatus following rotator cuff repair. The current study, which was undertaken in normal, asymptomatic shoulders, would suggest that the early progression of exercises prior to commencing active motion after rotator cuff repair may be better based on factors such as patient comfort, pain tolerance and available ROM.
Ethics approval
Ethics approval was obtained by the University of Western Australia Human Research Ethics Office (RA/4/1/7559).
Conflict of Interest Statement
No other authors have any conflicts of interest.
Acknowledgements
The authors thank Daniel Cottam and Jonathan Staynor from the School of Human Sciences Biomechanics Laboratory at University of Western Australia for their help with data collection.