INTRODUCTION
A rupture of the anterior cruciate ligament (ACL) is one of the most common sport related injuries. Patients who want to continue to pursue pivoting type of sports often undergo ACL reconstruction (ACLR) followed by extensive periods of rehabilitation. However, patients after ACLR still may have up to a 40 times greater risk of reinjury relative to those without injury.1 Following ACLR, aberrant movement patterns have been linked to an increased risk of a second ACL injury and may also explain why not all patients return to their pre-injury level.2–4 Current rehabilitation approaches may not optimally target deficits in motor control. An emphasis on the dynamics of skill (re)acquisition in current rehabilitation programs have been recommended to target these motor control deficits.5–9 To best improve motor learning and performance after ACLR clinicians may need to consider the way in which verbal instruction and feedback influences attentional focus and thus skill development throughout the rehabilitation process.9–11
A traumatic injury, such as an ACL rupture, may trigger a cognitive disruption and has the potential for maladaptive neuroplasticity with motor and premotor areas of the cortex being more active during simple movement tasks compared to uninjured individuals.12,13 Loss of function, pain, fear of reinjury, and other psychological factors may cause a shift in focus towards the injured area such as the knee. Therefore, the patient recovering from the injury is excessively focusing on the injured area during movement execution.14–17 This focus directed towards body movements, and accompanying brain adaptations, potentially deters motor performance after sports injury. Return to high level performance may benefit from the adoption of an external focus of attention when providing instructions directed towards the intended movement effect.17,18 However, clinicians utilize internal focus instructions over 90% of the time.19,20 This extra focus on the body may stimulate the motor and premotor areas of the cortex to be active to a greater degree. While a rationale may be that an internal focus is necessary to progress from the cognitive stage of learning to the associative and automatic stage, this view is not well supported in the motor learning literature.21,22 Furthermore, misconceptions regarding when to use an external focus of attention (e.g. early vs. late rehabilitation or description vs. execution of movement) alongside a recent body of literature that has attempted to extend this work into hybrid models, warrants a critical evaluation. Therefore, the purpose of this commentary is to provide a clinical framework for the application of attentional focus strategies and guide clinicians towards effectively utilizing an external focus of attention throughout ACLR rehabilitation.
CONSIDERING AN EXTERNAL FOCUS OF ATTENTION TO OPTIMIZE MOVEMENT OUTCOME
A subtle change in the wording of exercise instruction prior to movement execution can promote an external focus of attention so that attention is directed to one’s intended effect of the movement (goal-directed attention), in contrast to paying attention to one’s own body movements (i.e., internal focus of attention or self-directed attention). This external focus of attention centers on the ability to engage both the perceptual-cognitive and physical performance factors in the functional task environment.23 For example, in an effort to improve balance performance, a patient may perform a single leg balance task on a Bosu ball (BOSU, Ashland, OH). A clinician may instruct the patient using an internal focus of attention such as, “minimize movement of the feet”. However, by just changing one word to “minimize movement of the Bosu” the instructions become externally focused. In addition, an external focus of attention can also be elicited by means of a metaphor (e.g., “stand still like you are stuck on Velcro”), analogy ("imagine you are on the peak of a mountain, stay on the mountain!), an object attached to the body (“keep the tape attached to the chest still”), or an imagined object, where a mental image of the movement goal is obtained (e.g., thinking of the leg as a line, “keep the line straight”).24–28
The benefit of an external focus of attention compared to an internal focus of attention for enhancing motor skill learning and performance has consistently been shown through a large body of evidence across different populations, tasks, and skill levels.10,29,30 These include tasks such as balancing, running, agility performance, change of direction performance, force production, and horizontal and vertical jump performance.6,31–38 Collectively, an external focus of attention has been shown to produce more accurate performance, improved reaction time, and more efficient movement (e.g., reduced muscular activity).39–41 Also in athletes following an ankle sprain, those who received external focus instructions to “keep your balance by stabilizing the platform” demonstrated improved balance after training compared to an internal focus group instructed to “keep your balance by stabilizing your body”.18
In primary ACL injury prevention, there is evidence which illustrates how an external focus of attention can lead to improved movement form, jump performance, and result in safer landing mechanics. A literature review on jump and landing technique showed that an external focus of attention improves movement with greater knee flexion angles, greater center of mass (CoM) displacement, lower peak vertical ground reaction force (vGRF), and improved neuromuscular coordination, while maintaining or improving performance (i.e., jump height or distance).6 These findings suggest a decrease in ACL injury risk.
In another example, the effects of an internal and external focus of attention on landing forces were compared in adolescent rugby players before and after a two-week training program. An external focus directed to “focus on landing softly” resulted in a reduction in landing forces with the addition of a secondary cognitive task compared to an internal focus of attention directed to “focus on bending your knees when you land,” which showed an increase in landing forces with the addition of a secondary cognitive task.42 Therefore, an external focus of attention utilized less conscious control in dual-task conditions which is similar to the conditions that athletes may face when returning to sport. Similarly, using an external focus of attention was also shown to immediately result in reduced landing stiffness in female athletes as well as improved landing technique compared to an internal focus of attention.43,44 In a recent study utilizing the Landing Error Scoring System (LESS), colored tape was attached to each participant’s mid patella alongside the tips of their shoes.45 The external focus of attention instructions were: “when landing from the box, focus on pushing the red tapes (attached to the mid patella) forward, and pointing the green tapes (attached to the tips of the shoes) forward.” The internal focus instructions were, “when landing from the box, focus on pushing your knees forward, and pointing your toes forward.” Better landing quality, expressed by a lower LESS score, was achieved using an external focus of attention compared to internal focus of attention. In another jump landing study, athletes training with an external focus of attention (“push yourself as hard as possible off the ground after landing on the force plate”) demonstrated greater knee flexion range of motion compared to another group training with an internal focus of attention (“extend your knees as rapidly as possible after the landing on the force plate”). These results were not only retained one week later, but also carried over to an unanticipated sidestep cutting task.46
An external focus of attention may be successful by facilitating functional connectivity, modulating surround inhibition, and increasing intracortical inhibition to resemble the sensorimotor integration typically seen in more skilled action.47–49 The constrained action hypothesis suggests that an internal focus disrupts the motor system by promoting conscious control which leads to a breakdown in the in the otherwise natural organized coordination of one’s movement. On the other hand, an external focus allows for a greater degree of self-organization by promoting automatic control processes.32 Therefore, if movements are not planned in terms of the intended movement effect, but in terms of specific body movements, the outcome will be less-than-optimal.50 Additionally, an external focus has been recognized as a critical element to goal-action coupling, strengthening the neuromuscular processes between the patient’s movement goal and desired movement action.51
Thus, it is clear that just a slight change of wording can affect motor learning and performance.52,53 Because instructions and feedback are constantly used in rehabilitation of ACLR patients, the effect of different constructs of language on movement mechanics should not be underestimated. Recent literature shows that several misconceptions of what an external focus is and how it should be implemented within ACL injury rehabilitation exist. In the following sections, a brief review of this literature along with clinical examples is provided to help aide clinicians in effectively utilizing an external focus of attention.
STAGES OF LEARNING
Rehabilitation after ACLR can be categorized into three stages: early, intermediate and late. For the intermediate phase, it has been recommended that an internal focus of attention is necessary to achieve sound movement patterns to restore motor function (i.e., muscle contraction ability) with patients only being able to adopt the ‘right’ way of moving when you tell them explicitly how to do it.22,54 Then, during the progression of the exercises, external factors that increase task complexity such as hurdles or unstable surfaces should be added.22 These assumptions are based on more traditional views of motor learning where a linear progression for learning or re-learning motor skills is paramount.55,56 Traditional teaching of exercise also tends to emphasize specific step-by-step detailed instruction of a movement pattern for repetitive rehearsal (providing an “optimal” way to perform a specific movement), as well as the application of corrective and frequent feedback in repeating a movement technique.57,58 Briefly, through this lens, attentional demands transition from being under high conscious control to being controlled with very little cognitive effort over time as movements become more accurate, consistent, and efficient. However, as described by a more recent non-linear progression for learning, a given range of possible movement solutions should allow clinicians to guide patients as they self-organize and find their optimal movement to reach the goal of the movement (e.g., soft landing).7,57 As compared to internal focus of attention, an external focus provides the opportunity for self-organizing, as shown by efficient recruitment of motor units, fewer co-contraction of muscles, increased functional variability, and a “freeing” of the body’s degrees of freedom.58–60 An external focus seems to speed up the learning process, displaying adoption of movement patterns similar to more skilled performance. This effect can be seen in both the early stages of learning (i.e., novice) and the later stages of learning.10 For example, in an early-phase rehabilitation isometric force production task performed by healthy physically active individuals, an external focus directed to “focus on pushing up into this pad as hard as you can” resulted in an 8% increase in force production of the gluteus medius compared to an internal focus of attention directed to “focus on contracting the muscles of your outer hip as hard as you can.”61 Moreover, using an app-based active muscle training program (GenuSport Knee Trainer, Weber-Spickschen) where the aim is to produce force by pushing the knee down into the measuring unit, patients post ACLR improved strength significantly more compared to a control group who trained with an internal focus of attention. In the former, the patient attends to a game on the tablet, rather than their body part, to control a flight course of an airplane with the aim to destroy balloons.62
The second assumption is that once one starts to transition into the late rehabilitation phase, adding aspects to the environment (e.g., hurdle, ball, or an unstable surface) leads to a shift to an external focus of attention.22 However, adding environmental factors do not shift the patient’s attention to an external focus but simply refer to objects in the environment and not one’s intended movement effect. Likewise, in the later stages of rehabilitation, it is suggested to progress from closed skills (e.g., usually self-paced, predictable skills that are decontextualized from the environment) with an internal focus of attention to more open, sport-specific skills with an external focus.22 Here, it is assumed that an internal focus of attention is better or equivalent for closed skills and external focus for open skills (e.g., patients have to make decisions and adapt their skills to an unpredictable environment).22 In contrast, it is also assumed that practicing closed skills cannot benefit from external focus instructions because the individual lacks correct movement patterns. However, the benefit of an external focus has been shown in both closed and open skills.10,34,63,64 This effect also extends across early and late stages of learning. Therefore, clinicians should evaluate the task goal, establish an optimal challenge level, consider patient preferences regarding the appropriate instructions, and create an external focus in relation to the patient’s action capability within the functional task environment.32,65–68 Regardless of utilizing a closed or open skill, it is recommended to keep exercises as representative as possible of conditions that patients will return to through all stages of rehabilitation.23
DESCRIPTION VS. EXECUTION
Another misconception is that with an external focus of attention, patients are not allowed to know the goal of the exercises (e.g., increase knee flexion, deeper landing) or focus on their body to perform the requested movement.69 However, an external focus does not mean that the patient is not aware of her or his body movements50 but rather means the patient is focusing on the intended movement effect – while preparing for the execution of a ballistic skill (e.g., throwing or hitting a ball) or during the execution of a continuous skill (e.g., balancing, swimming, cross-country skiing). Adopting an external focus is thus related to the planning of the movement, not with the processing of intrinsic feedback or bodily awareness.50 This does not mean that a clinician must never use body related words that elicit an internal focus of attention but verbiage should be limited to the description portion prior to the execution of the motor skill.
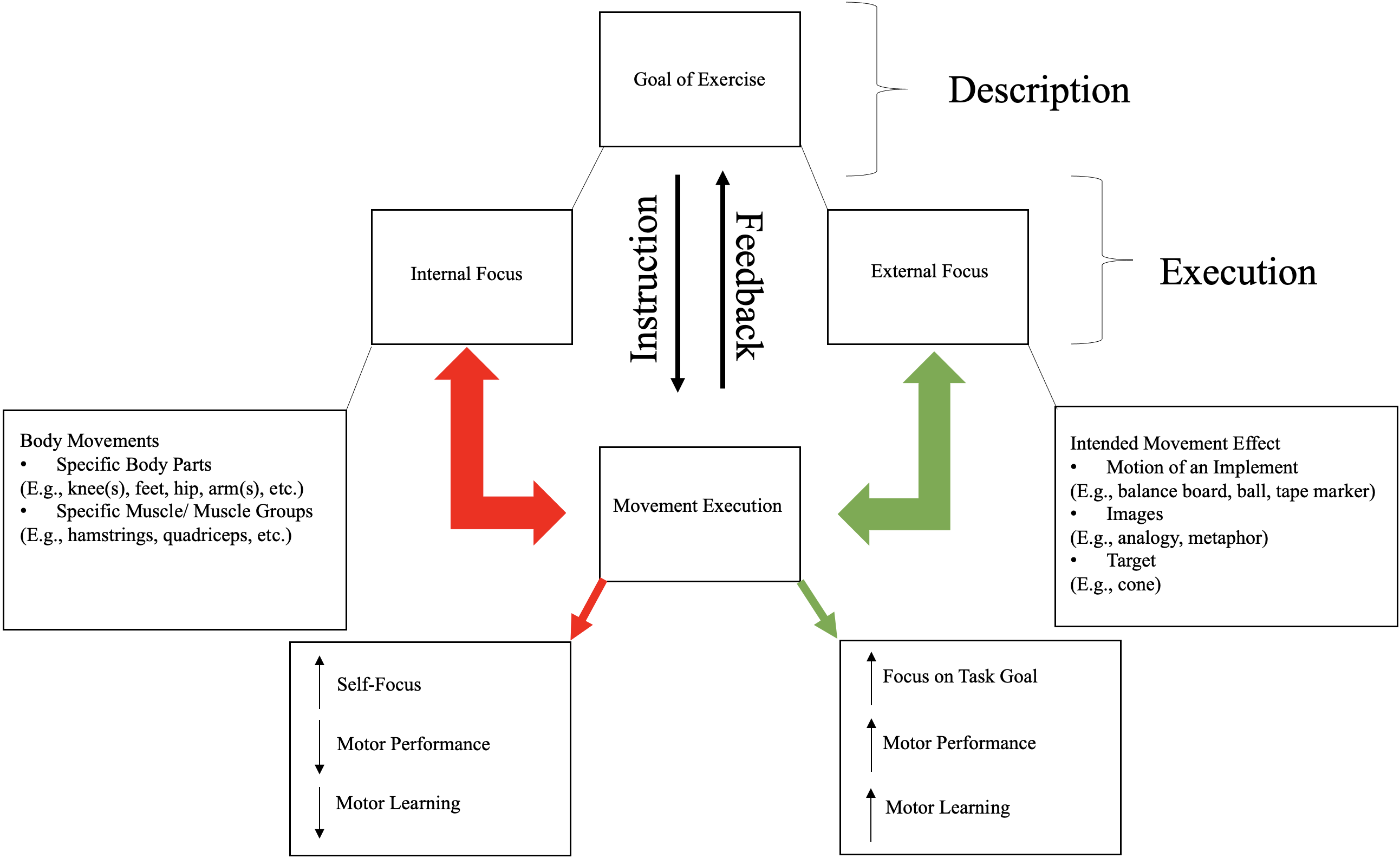
It is important to differentiate between telling the patient the goal of the exercise and the instructions and feedback being provided during practice. In case of rehabilitation after ACLR, this would mean that you can explicitly tell the patient the general goal of an exercise. For example, “the goal of this exercise is to improve your knee bending while landing, as this promotes a softer landing, which is better for your knee.” Then, as your patient is preparing to execute the exercise, it is critical to shift their attentional focus that corresponds closest to the task goal. This means, the physiotherapist can choose either an internal focus of attention (e.g. “flex your knee when landing”, as most frequently done) or an external focus of attention (e.g. “focus on landing with as little noise as possible” or “pretend you are going to sit on a chair when landing”) (Figure 1).6 With the external focus of attention, you do not have to explicitly tell the patient how, rather give the patient the freedom to come up with a solution to complete the goal of the task in the functional environment (less noise during landing from a jump). Here the patient is allowed to seek out relevant features of the task environment to shape self-organization. One must recognize there will not be one perfect movement solution.7 Based upon the intrinsic dynamics of the patient and the channeling of exploratory movement solutions, clinicians should highlight the existence of a multitude of stable movement patterns and solutions for a task.70 In the example above, the end effect is the same (i.e., increased bending in the knee when landing), however the focus of the patient when executing the motor task is different. As a result, shifting to an external focus may lead to better movement form both in practice, during retention, and upon transfer to more competition and game-like interactions.

THE RIGHT FOCUS
While the purpose of this commentary is to illustrate that word choices are crucial to implement an external focus of attention, this is not a new phenomenon or discussion. Over the last several years there has been an increase in research related to attentional focus, ACLR rehabilitation, and biomechanical risk factors related to ACL injury. However, the terminology encompassing an external focus of attention has lately been extended to descriptions such as: 'external factors’, ‘external cueing’, ‘external focus of control’, ‘external goal’, ‘externally focused motivation’, ‘external feedback’, ‘external feedback motivation’, ‘visual external focus’ and ‘external visuospatial environment’.54,71–74 As a result, the research relating to attentional focus can be hard to interpret. Attentional focus is defined as the conscious effort of a patient to focus their attention on explicit thoughts or feelings in an effort to execute a task with superior performance.69Attentional focus relates closely to what you tell your patient(s) prior to the execution of the exercise whereby you direct them where to focus their attention: internally (i.e. on body part(s) and movement(s)s) or externally (i.e. on intended movement effect). Hybrid instructions, such as “step toward the cone by pushing the floor away with your back foot” for the execution of a lunge or “balance a board flat across your shoulders” for the correction of excessive lateral trunk flexion on squat jump landing are not recommended.54,74 These hybrid instructions are not purely an external focus of attention as they include a reference to a body part: the back foot. This “self-invoking trigger” may result in inefficient activation of the neuromuscular system.75,76 A minor change such as “step toward the cone by pushing the floor away with your back shoe” or “balance a board flat across your shirt” would make this instruction solely an external focus instruction. While the inclusion of motor learning principles in physical therapy have been around for over a decade, the above-mentioned misinterpretations regarding the definition and application of an external focus offer an opportunity to re-evaluate how motor learning principles are being applied as a means to treat complex injuries such as the ACL injury.6–9,11 Creating and implementing an external focus takes time and requires practice but may help to optimize patient care. Clinical examples that will offer clinicians examples of how to incorporate external focus in their practice are provided for the early (Table 1), intermediate (Table 2), and late (Table 3) phases of rehabilitation.
CONCLUSION
Targeting deficits in motor control is a critical component for ACLR rehabilitation. One way to potentially improve neuromuscular control is by altering how attentional focus is directed when performing motor skills across early, middle, and late phases of rehabilitation. An external focus of attention offers an alternative strategy that facilitates automatic movement control and results in more effective performance and learning than an internal focus of attention. Clinicians are encouraged to adopt an external focus of attention in their practice over an internal focus of attention to promote optimal movement strategies throughout rehabilitation interventions. Further, researchers should strive to use similar terminology when it comes to describing attentional focus interventions into experimental designs.
Disclosure statement
No financial interest or benefit has arisen from the direct applications of this research. The authors report no conflicts of interest.