
INTRODUCTION
The tibialis posterior (TP) muscle is the main dynamic stabilizer of the medial longitudinal arch and is critical to normal foot function during gait.1–5 It is located in the deep posterior compartment of the lower limb along with the posterior tibial artery and vein and the tibial nerve. The muscle becomes a tendon in the distal third of the leg. The tendon passes posterior to the medial malleolus where it is held in place by the flexor retinaculum.5 By virtue of its position posterior to the axis of the talocrural joint and medial to the subtalar joint, the tibialis posterior muscle is responsible for plantarflexion and inversion and helps to create a rigid lever by locking the hindfoot for efficient push-off at terminal stance.1,2,4,6
Several factors can lead to overuse and degeneration of the tendon. The TP is constantly resisting arch flattening effects of the triceps surae.3 Shortening of the triceps surae can lead to excessive eversion during stance phases of gait.7 When the hindfoot is in an everted position in the late stance phase of gait, the midfoot complex is unlocked. This position can place excessive forces through stretching of the static structures that support the medial longitudinal arch such as the plantar ligaments.4 As these static structures begin to lose integrity, the load on the posterior tibialis muscle increases to compensate for the soft tissue laxity. Over time, decreased support from the posterior tibialis muscle can result in flat foot deformity.3 Therefore, the TP is an important muscle to consider clinically when creating a therapy management plan for individuals with foot and ankle pathology.
Dry needling is an invasive procedure in which a solid filament needle is inserted into muscles in an attempt to reduce pain and normalize muscle function.8,9 Dry needling has been shown to be a valuable clinical adjunct to the management of individuals with a variety of lower extremity conditions.10–16 Although dry needling may be effective for individuals with lower extremity injuries, it is important to recognize that, although rare, significant complications may result from needling intervention.17 In the largest study to date documenting adverse events after dry needling, Brady et al.18 reported that approximately 8% of patients exhibited bleeding, 5% exhibited bruising, and 0.01% reported lasting numbness after dry needling. A recent case study specifically described a radial nerve injury resulting in wrist drop following a dry needling session to the lateral aspect of the upper arm around the distal third of the humerus, which had yet to resolve.19 Although vascular injuries appear to be fairly common after dry needling, no serious adverse consequences have been reported. Nerve injuries after dry needling appear to be rare, but may cause lasting effects and create substantial disability.
Due to the location in the deep posterior compartment, determining accurate placement of a needle into the TP muscle is difficult to confirm. In addition, reliably avoiding the posterior tibial artery and vein and the tibial nerve may be challenging due to their proximity to the TP muscle. Diagnostic ultrasound imaging has been shown to reliably measure the thickness of tibialis posterior muscle and identify muscle contraction.20 Ultrasound has been utilized in previous studies to confirm needle placement, but not of the TP muscle.21–23 Therefore, given the clinical relevance of the TP muscle for normal foot and ankle function, the purpose of this study was to assess the accuracy of needle placement in the TP muscle and determine the needle placement in relation to the neurovascular structures located within the deep compartment.
METHODS
This study was approved by the Human Research Ethics Committee of Regis University and was performed in accordance with the Declaration of Helsinki. Twenty healthy participants signed an informed consent prior to their inclusion in the study. Participants were excluded if they had operative treatment of their lower extremity within the past 3 months, had received dry needling within the past 30 days, were pregnant, had a history of systemic disorders in which dry needling would be contraindicated (bleeding disorders or current anticoagulant medication use), or were immunocompromised. This population was a sample of convenience and participants were recruited by word of mouth. Individuals’ height and weight were documented.
Dry Needling procedure
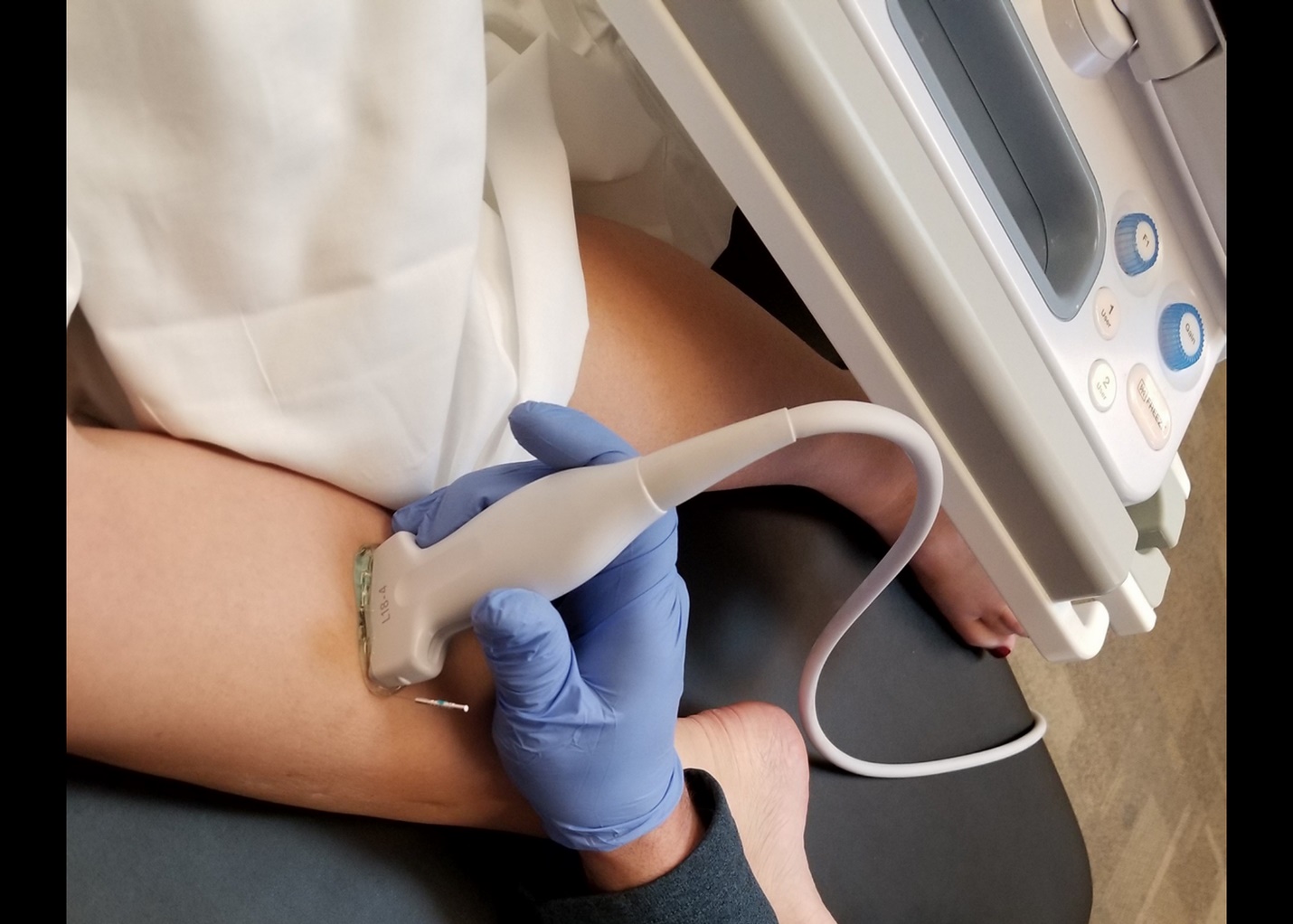
Dry needling was performed in routine clinical fashion without ultrasound guidance. Filament placement was initially estimated consistent to clinical practice, and then the distance from the medial joint line was measured and recorded. Sterile stainless-steel needles with a plastic cylindrical guide, 50mm or 60 mm in length and .30 mm caliber were used. The length of needle selected for the procedure was based on the size of the individual’s leg. A “clean technique” was utilized which included hand washing, sterile latex-free gloves, and cleaning the skin with alcohol prior to needle insertion. The participant was positioned in a right side-lying position for the procedure, and the right posterior tibialis was needled in all individuals. The tibia was measured from the medial joint line to the tip of the medial malleolus and the needle placement occurred between approximately 30-50% of the tibial length measured from the medial joint line. This is consistent with previous research assessing reliability of ultrasound imaging of the tibialis posterior muscle.20 In addition, this range was selected to target more of the muscle belly of the tibialis posterior given the muscle transitions to tendon more distally in the deep posterior compartment. Due to the location of the TP muscle within the deep posterior compartment and the inability to directly palpate the muscle, the needle approach and insertion was based on anatomical aspects. The neurovascular bundle lies posteriorly within the deep posterior compartment and therefore, the needle was inserted parallel to the border of the tibia from a medial to lateral direction avoiding a posterior angulation (Figure 1).

Ultrasound imaging
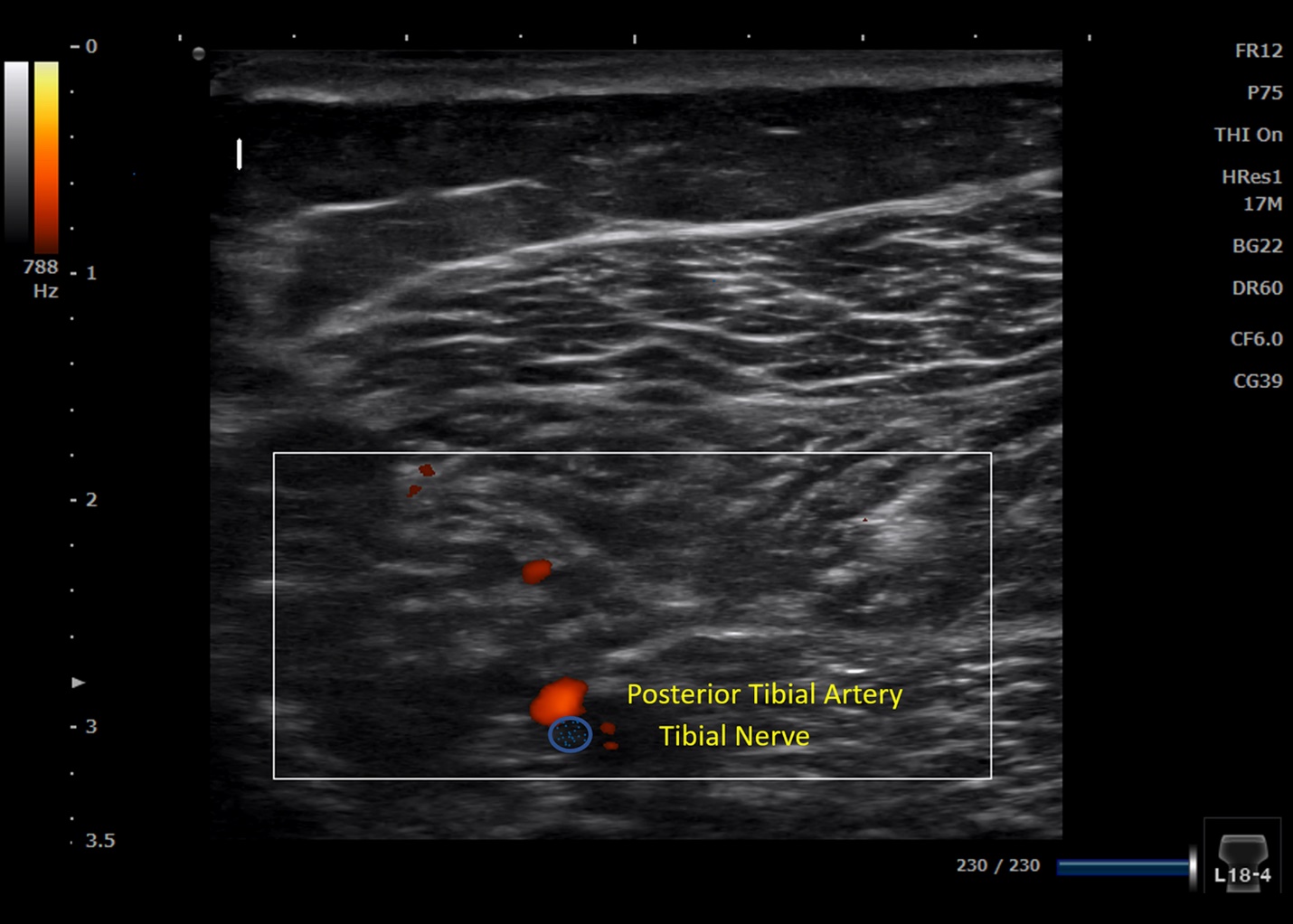
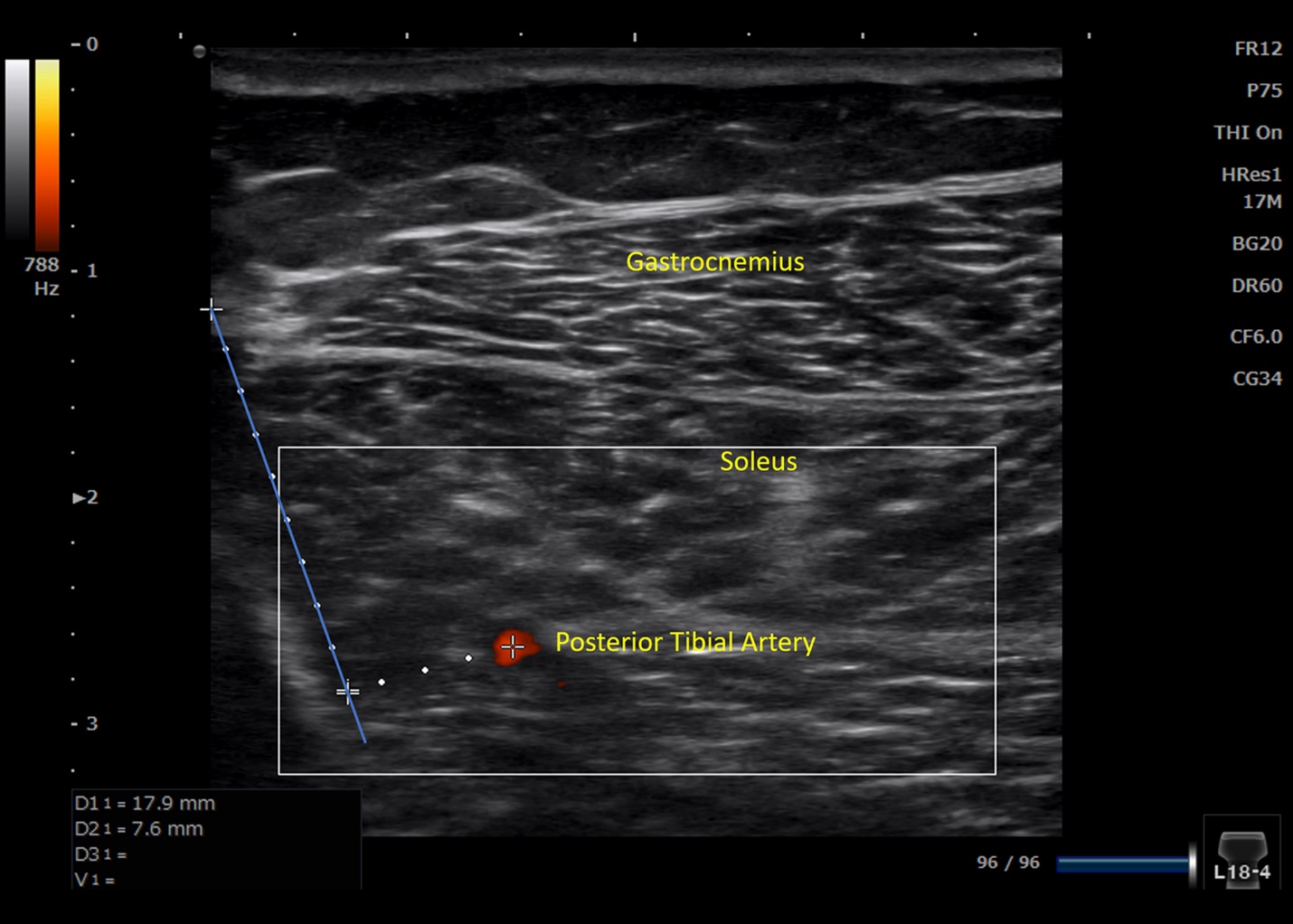
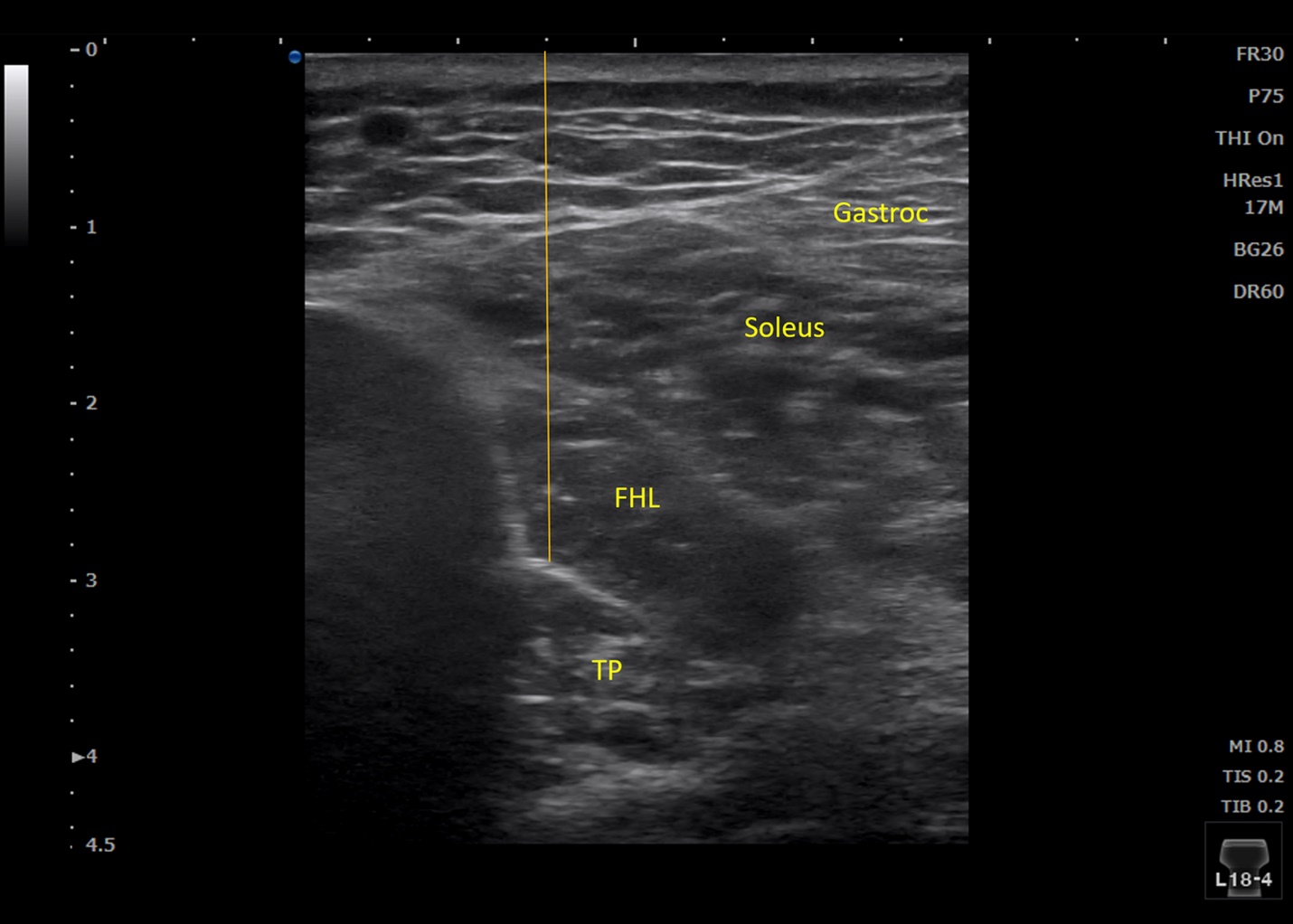
After the filament was placed, a Sonimage ultrasound unit with a 4-15 MHz linear transducer (Konica Minolta, Wayne, NJ) was utilized to verify anatomic placement. Sterile ultrasound gel was used on all individuals. All ultrasound imaging was conducted by a physical therapist with 10 years of experience in musculoskeletal ultrasound imaging. The physical therapist performing the ultrasound imaging had been mentored in the use of diagnostic ultrasound by experienced practitioners and had done training provided by the manufacturer as well as continuing education courses. Images were performed in short axis of the posterior tibialis muscle (Figure 2). All superficial musculature was identified in addition to the neurovascular bundle (Figure 3). The simple needle visualization (SNV) setting of 6 was used and the needle contrast was set at medium. The depth and time-gain-compensation were adjusted as needed to enhance clarity of the image. Once the needle was in place, the transducer was moved and positioned until the needle was displayed on its longitudinal axis. The needle was left in place throughout the procedure and light pistoning was used to confirm the needle imaging. Screen capture via frozen image was utilized, and the shortest distance from the needle to tibial nerve was measured. The screen was unfrozen, and the Power Doppler mode was turned on to identify the posterior tibial artery. Again, the screen was frozen and the shortest distance from the needle to the posterior tibial artery was measured (Figure 4). The needle was then removed from the participant, and the depth from the skin to the most superficial border of the TP muscle where the needle had been inserted was measured (Figure 5).




Data Analyses
Data analyses were performed using SPSS Version 27.0 statistical package (IBM Corporation, Armonk, NY). Baseline characteristics were summarized. Averages and standard deviations of the distance from the needle to the posterior tibial artery and tibial nerve were calculated. Previous studies utilizing ultrasound imaging to validate needle placement have included a sample size of 10-20 individuals; therefore, this studyincluded a sample size of 20 individuals.21,22
RESULTS
Needling and ultrasound imaging of the posterior tibialis muscle was conducted on 20 healthy individuals (8 male and 12 female) between November 2020 and February 2021. See Table 1 for baseline characteristics. A 50 mm filament was used in 8 (40%) of the individuals and a 60 mm filament for the remaining 12 (60%) of individuals, and the size of needle selected for the procedure was based on the size of the individual’s leg. The average needle placement was 41.1% ± 4.7 % the length of the tibia as measured from the medial joint line. No individuals in this study incurred any serious adverse events. Three individuals (15%) experienced a minor adverse event consisting of minimal bleeding that ceased in less than a minute of the needle being withdrawn.
Ultrasound imaging confirmed that the needle was in the tibialis posterior muscle in all 20 individuals. The needle was not inserted into the neurovascular bundle in any individual. See Table 2 for results. The superficial border of the tibialis posterior muscle from the skin was at a mean depth of 25.8 ± 4.9 mm.
DISCUSSION
The importance of the tibialis posterior muscle in normal foot function cannot be understated. Therefore, identifying interventions that promote the health of this structure is imperative. Research has demonstrated that dry needling can help increase blood flow, improve muscle activation, and affect muscle stiffness.24–26 Therefore, needling of the tibialis posterior may be prudent within overall patient management. The results of this current ultrasound study demonstrate that the tibialis posterior muscle can be consistently needled, noting no individuals in this study incurred any serious adverse events. The needle was not inserted in the neurovascular structures in any individuals.
Due to the deep anatomical nature of the tibialis posterior muscle, it cannot be directly palpated. Therefore, dry needling may be an important therapeutic tool for individuals with posterior tibial dysfunction. However, it is important to note that in some individuals, the needle was 2.1 mm away from the posterior tibial artery and 3.5 mm away from the tibial nerve. In this study, the needle was inserted in close proximity to the tibia in a medial to lateral direction running parallel to the posterior border of the tibia. It may be important for clinicians to keep in mind that if the needle is angled more posterior instead of running parallel to the posterior border of the tibia, it is likely to be in closer proximity to the neurovascular structures. The mean depth of the superficial border of the TP muscles was 25.8 ± 4.9 mm. Previous research has demonstrated that the largest bulk of the TP muscle belly is located between 30% and 50% of the length of the tibia as measured from the medial joint line. The cross-sectional area of the TP muscle at this location is approximately 3.5 to 4.0 cm2.20 This is important for clinicians to consider when determining appropriate needle length for needling the TP muscle, and in this study supports the selection of 50-60mm filament/needle length allowing for 1-2 cm filament length outside of the body at full insertion.
While this study preliminarily validates that clinicians can safely place a solid filament needle into the TP muscle, potential limitations should be recognized. One limitation of this study is that all needling was performed by one experienced clinician with greater than six years of experience in dry needling, and therefore, it is not known if the accuracy of this needling approach can be extrapolated to less experienced clinicians. As this study did not assess the effectiveness of dry needling of the TP in individuals with dysfunction, future randomized controlled trials in patients with potential TP dysfunction should be performed and include dry needling as currently described. Lastly, it is important to keep in mind that variations in anatomy exist which could impact the risk of the needling procedure in a larger sample of individuals. The point where the popliteal artery bifurcates into the posterior and anterior tibial arteries is fairly regular. The split takes place proximally and deep to the origin of the soleus. If there is a variation in the posterior tibial artery, it is typically a variation of the fibular artery as the fibular artery usually branches off of the posterior tibial artery distal to the formation of the posterior tibial artery.27
CONCLUSIONS
Preliminary data from this ultrasound imaging study indicate that placement of a solid filament needle into the TP muscle with avoidance of the neurovascular structures of the deep posterior compartment is promising; however, further validation studies are needed.
Financial Disclosure
We affirm that we have no financial affiliation or involvement with any commercial organization that has a direct financial interest in any matter included in this manuscript, except as cited in the manuscript.
Statement of Institutional Review Board
This study was approved by Regis University’s Institutional Review Board.