INTRODUCTION
Physical activity is an important component of good health for all individuals and recommended for improving cardiorespiratory and muscular capacity, bone health and reducing the risk of depression and non-communicable diseases.1 However, participation in recreational or competitive sports is not without an increased risk of acute injury or overload.2,3 Many interventions have been developed to reduce the risk of sports-related injuries, especially at the lower limb. In particular, prevention programs composed of several neuromuscular training components such as muscle strengthening, balance and agility training have demonstrated preventive effects for lower limb injuries.4–7 While these programs have around 39% efficacy in reducing the risk of lower extremity injury and even higher efficacies of 54% and 50% for acute knee injuries and ankle sprains respectively,8 the effects may vary.
Compliance with injury prevention programs plays a key role in achieving the greatest possible preventive effect.9–12 To increase compliance, it has been suggested that the coach is the most important person to promote the process of implementing an injury prevention program,13,14 and regular practice of these programs is also required to achieve the desired outcome.5,15,16 Yet a coach can more easily be persuaded when a better understanding of the motivations and facilitators behind program implementation is attained.15,17 From the trainer’s perspective, one of the key factors in sport is performance; the implementation of prevention programs could be facilitated if these protocols were to demonstrate positive effects on performance.11,18–21 In fact, performance is identified as the primary goal of elite sport by coaches as well as athletes and sport physiotherapists.22 Athletic performance is defined as the ability to respond effectively to the specific physical demands of the sport being played.23 Several performance factors include maximum muscle strength and muscle power, agility, speed, flexibility, balance and stability.23 Furthermore, injury prevention is defined as an accessory goal in achieving athletic performance.24
The effects of injury prevention programs on performance must be clearly understood to facilitate the primary implementation of these programs by coaches. Therefore, our study objectives were to summarize the findings of current systematic reviews on the effectiveness of lower limb injury prevention programs with multiple neuromuscular components on sports performance and to quantify their effects. We hypothesized that injury prevention programs can improve certain performance criteria.
METHODS
This umbrella review was carried out according to the model of Aromataris et al.25 Details of the review protocol are registered on PROSPERO and can be accessed at https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42020162334.
Search Methodology
For this umbrella review, two authors compiled all evidence from pertinent systematic reviews found within the following databases: PubMed, CINAHL, Ovid, Cochrane Database of Systematic Reviews, and PEDro. The search strategy was guided using the Population Intervention Comparison Outcome Study Design (PICOS) approach and selected terms were combined in a Boolean search. Key terms used were “sportsman”, “sportswoman”, “injury prevention program” and “performance”. More details about the search strategy used and the results for every database can be found in Appendix 1.
All systematic reviews had to be written in French, German or English and published between January 1, 1990 and January 31, 2020. Thereafter, a sports injury prevention expert/co-author identified any further references relevant to the topic, which had not been identified by the initial search strategy and to ensure comprehensive coverage of the literature.
All identified references were imported into the Covidence systematic review software (www.covidence.org) (Veritas Health Innovation, Melbourne, Australia) to identify and remove duplicates. Two authors then independently screened all article titles and abstracts to select relevant reviews eligible for full-text reading. The inclusion criteria were defined as follows:
Population: athletes of all ages and sex who participate in any sport (e.g. soccer, basketball, volleyball, ice hockey)
Intervention: all types of multicomponent exercise intervention (e.g. strength, balance, plyometrics…) used with the goal to prevent injuries of the lower limb
Comparison: usual training and/or usual warm-up procedures
Outcomes: performance criteria defined as: (1) strength, (2) balance, (3) agility, (4) jumping ability, or (5) speed.
Exclusion criteria were defined as not meeting one or more of the defined inclusion criteria. If there was any doubt about the eligibility of a screened reference, consensus was reached primarily by discussion and a third author was only consulted when the reference’s eligibility could not be established.
Methodological Quality Assessment
The Assessing the Methodological Quality of Systematic Reviews (AMSTAR) tool was used to classify the reviews according to their methodological quality. Eleven items are assessed using the options of “yes”, “no”, “not applicable” and “cannot answer”, where single points on the AMSTAR scale can only be accumulated for each “yes” answer. The AMSTAR ranking is based on three categories indicating low quality reviews with scores of 0 to 3 points and reviews of moderate (4 to 7 points) and high quality (8 to 11 points).26,27 Two authors independently assessed the methodological quality of the included systematic reviews according to AMSTAR and only those of moderate or high quality were included, as summarized in Table 1. Any AMSTAR rating conflicts were resolved by discussion with a third author until consensus was reached.
Data Extraction and Analysis
The data extraction process was carried out independently by two authors. Information on the author, publication year, sample size, intervention and study outcomes was collated and managed in Microsoft Excel 2020. For any conflicting data, a third author was consulted until consensus was reached.
The outcomes analyzed for this umbrella review included the following performance measures of: strength (quadriceps and hamstring isokinetic strength and hamstring/quadriceps ratios), balance (ability to maintain one’s center of gravity within their base of support), agility (ability to change direction), jumping abilities (horizontal and vertical jumping as well as reactive jumping [e.g. drop jumping]) and sprint speed (in a straight line). Further data on the number of study participants, sex of the study population, and type of sport participated in were also exported. If a meta-analysis was conducted within the systematic review, the results of the studies were reported using the standardized mean difference (SMD), 95% confidence interval (95% CI) and I2 test. When the SMD was not reported, other measures including either the mean difference (MD) or percentage of change from baseline were noted as available. When a meta-analysis was not performed, a narrative synthesis of the study results—describing the findings of the included studies based on outcomes and intervention types executed—was provided.
For all meta-analyses, effect sizes were categorized according to Cohen27 as follows: values of 0 to 0.19 indicate a negligible effect, 0.20 to 0.49 represents a small effect, 0.50 to 0.79 a moderate effect, and greater than 0.80 a large effect.
Based on the umbrella review guidelines,25 a “traffic lights” system was used to summarize the effectiveness of prevention programs on the various performance criteria selected. A red color indicates that the intervention may be detrimental or less effective than the comparator (i.e. normal training program). An orange color was set for reviewed studies showing no difference between the comparison and intervention, and green denoted any beneficial effect of the intervention.
RESULTS
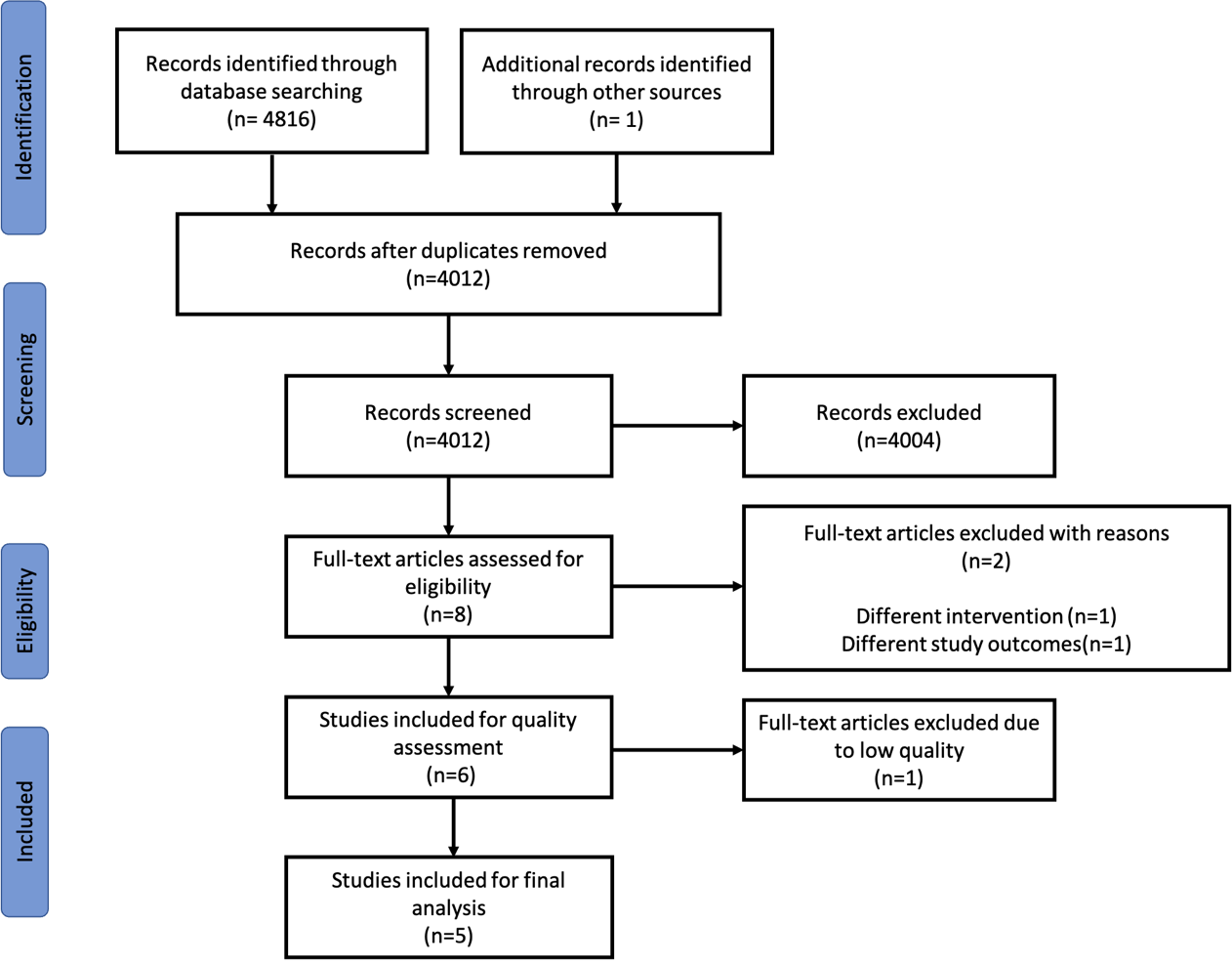
A total of 4,816 studies were initially identified with an additional reference discovered by the injury prevention expert (Figure 1).
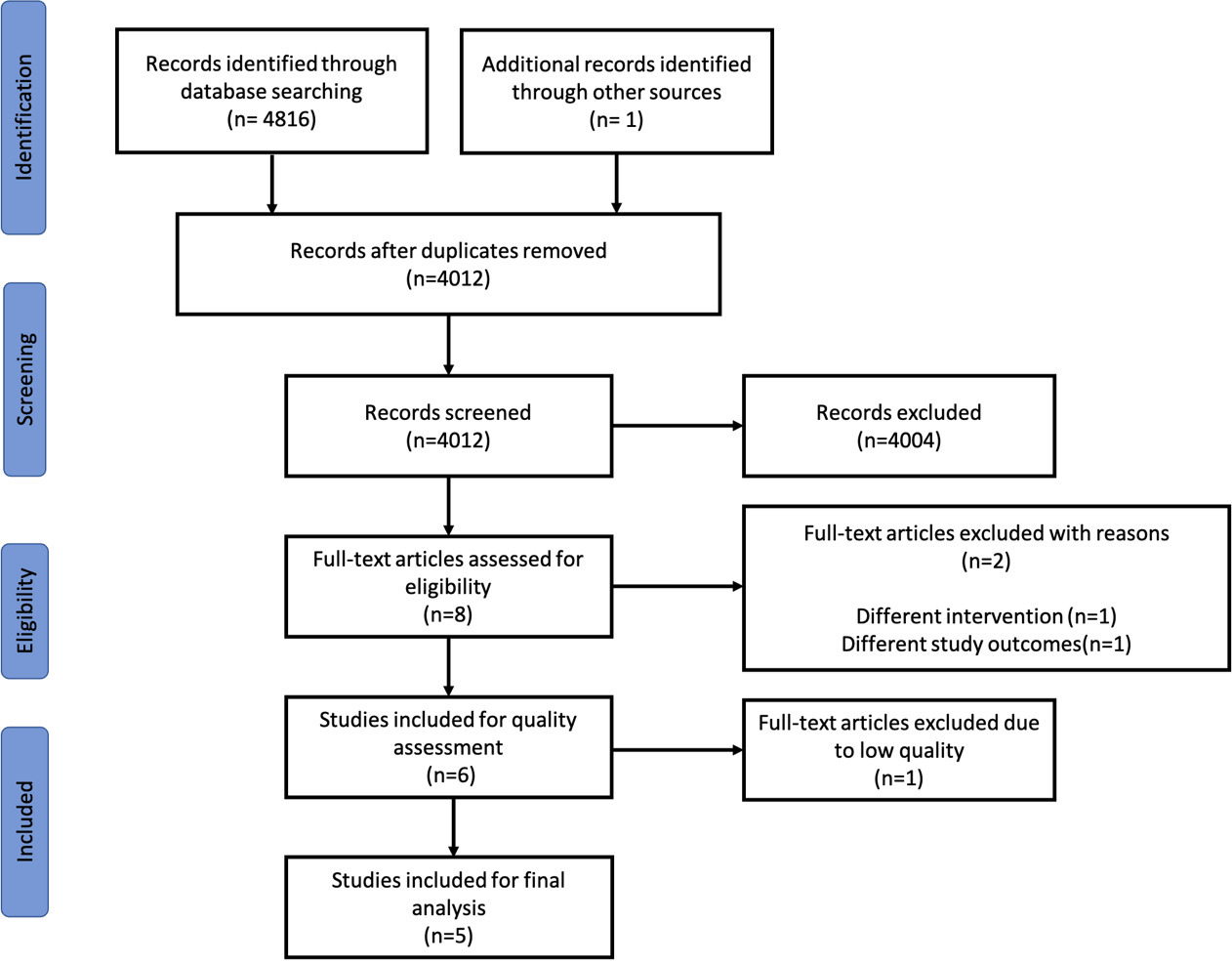
After the removal of all duplicates, 4,012 abstracts and article titles were screened, and 4,004 references were excluded after reading the titles and abstracts. The full text of the remaining eight references was read and two studies were excluded because they did not meet the inclusion criteria. The methodological quality of the remaining six studies was assessed, which resulted in the exclusion of one study28 due to its low methodological quality (AMSTAR score ≤ 3). The overall methodological quality of the final reference selection—comprising five systematic reviews that assessed the quality of 61 primary studies—as summarized in Table 1.
Injury Prevention Programs
A comprehensive summary of the review findings outlining the effects of injury prevention exercises on the selected performance criteria is detailed in Appendix 2.
Effects on Strength
Of the five systematic reviews, four evaluated the effect of neuromuscular exercise programs aimed at reducing the risk of injury on strength.29,31–33 For hamstring strength, small to moderate improvements were reported for isokinetic speeds of 60°/s (SMD: 0.56) and 240°/s (SMD: 0.31).29 Another review found an improvement in hamstring strength when interventions included eccentric hamstring strengthening exercises.32 Yet only small to negligible effects were observed in favor of improving quadriceps strength at isokinetic velocities of 60°/s (SMD: 0.49) and 240°/s (SMD: 0.19).29 The group of ter Stege reviewed studies focused on overall strength of the lower limb and found an improvement in the strength of the entire lower limb.33 For hamstring-quadriceps ratios, a small positive effect was noted only at an isokinetic velocity of 60°/s (SMD: 0.40) with negligible effects at 240°/s (SMD: 0.13).29 The effects of interventions on hamstring-quadriceps force ratios were variable,32,33 but an 11.3% improvement in strength in favor of prevention programs was reported.31
Effects on Balance
Four reviews evaluated the effects of prevention programs on balance. A small positive effect (SMD: 0.29) was noted for static balance.29 For dynamic balance, the effects were also positive but variable: one review found a small effect (SMD: 0.31),29 another found a large effect size (MD: 2.68),30 and a third review reported the overall effectiveness of interventions on balance with an average improvement of 5.2% in scores between the baseline and post-intervention time points.31 The fourth review highlighted the variability in outcomes, but noted that dynamic balance can be improved in both groups; there was no improvement in dynamic balance in the pediatric group.33 For dynamic stability, moderate effects were observed (SMD: 0.72).29
Effects on Agility, Jumping and Speed
Two reviews identified large (SMD: 0.88) as well as weak effects (SMD: 0.25) in favor of prevention programs on agility.29,30
Two reviews identified the effects of prevention programs on vertical jumping and demonstrated small (SMD: 0.3129 and 0.2430), yet overall effectiveness of interventions on this outcome. For reactive jumping, weak effects (SMD: 0.29) were seen and for the horizontal jumping, there were negligible effects in favor of implementing prevention programs (SMD: 0.04).29 Three reviews evaluated the effects of prevention programs on speed. There were moderate effects of prevention programs (SMD: 0.66) on sprint speed,29 although another review only found a weak effect (SMD: 0.36).30 As a result of injury prevention programs in youth athletes, Hanlon et al only found a 2.2% improvement in speed,31 whereas an earlier review also focused on youth sports observed a large effect in favor of such programs (SMD: 0.92).29
DISCUSSION
The results of this umbrella review showed that there were five systematic reviews of moderate to high quality that examined the effects of lower extremity injury prevention programs on the performance outcomes analyzed. While the results for strength were quite variable, there was a trend indicating small to moderate improvements in this performance parameter as a result of prevention exercises. For the performance criteria of balance, agility, jumping and speed, the reviews demonstrated the clinical efficacy of prevention programs over control interventions. It is important to note that we considered prevention programs as effective for speed based on the systematic review of Hanlon et al.31 and the clinical effect observed. Nevertheless, it is necessary to interpret this result with caution due to the lack of reported confidence intervals.
Not all performance outcomes were collectively targeted in any one of the five systematic reviews included in this analysis. Strength was analyzed in four systematic reviews29,31–33 covering 22 unique primary studies, which is the largest number of primary studies for any one of the outcomes studied. The parameters of balance, agility, jumping and speed were evaluated by fifteen, nine, ten and eleven unique primary studies, respectively. Furthermore, many of the primary studies were included in more than one review among the selected articles. This could have an influence on the results of this umbrella review.
This work provides a synthesis of the effects of lower extremity injury prevention programs on performance in sport populations. These elements allow the clinician to make more informed choices when implementing such strategies. While the results demonstrate the overall effectiveness of prevention programs for sport performance, caution should be applied when interpreting the results because the efficacy of an intervention is defined in terms of its clinical significance and not only its statistical significance. The analyzed studies revealed vast heterogeneity among the populations that practiced a wide range of sports including soccer, floor hockey, futsal, volleyball or basketball. This may be due to selection bias, since we included studies covering a wide range of sporting populations of varying age, sex and playing level. The risk of publication bias also exists and while studies showing a statistically significant effect are more likely to be published, this aspect may play a role in the interpretation of the study results. A third important element is the study protocol variability; in fact, the length of implementation and frequency in practicing each of the different prevention programs was highly diverse. Consequently, performance bias may play a role in the analysis, but should be partially limited because the main outcomes of performance are objective measures. Furthermore, compliance was not comprehensively reported for all the included reviews and thus, could not be adequately presented within this umbrella review. Indeed, when studied, injury prevention program compliance is known to largely influence the outcome of the intervention (report bias).9,10 Additionally, current research suggests that adherence (proactive behavior) may be a more appropriate measure than compliance (passive behavior) when implementing exercise interventions.34,35 As noted by Brunner et al.,36 further studies should consider the systematic documentation of specific information such as the target population, details of performed drills with focus on intensity, frequency, type of exercise and duration, and a description of program implementation. Only through systematic documentation can data reproducibility be ensured for consistency when interpreting the reported results.
Further research should attempt to investigate some of the less studied outcomes such as agility or jumping, to better understand the potential improvements when practicing prevention programs. A second opportunity would be to study the effects of the different components (e.g. plyometrics and strength training) of the prevention programs separately. Understanding the individual effects of these components on performance and prevention would make it possible to (1) adapt these preventive programs to a specific sport context and (2) target certain determining aspects of sport performance in this context. The ultimate goal would be to encourage coaches to adhere to these programs as well as encourage athletes to regularly comply with them in an assiduous manner.
CONCLUSION
Injury prevention programs with multiple neuromuscular exercise components demonstrate overall efficacy to improve balance, agility, jumping and speed. For strength, the effects are varied, yet show a positive trend towards the usefulness of prevention programs. These beneficial effects on performance, coupled with demonstrated effectiveness in injury prevention, can be used as evidence for coaches to promote their implementation on a regular and consistent basis.
Conflict of interest
None of the authors have any conflicts of interest pertinent to this manuscript to disclose.