
Youth baseball is extremely popular, with an estimated 3 million children playing yearly in the United States alone.1 While baseball is a relatively safe sport, injuries are unavoidable with overuse throwing injuries to the elbow and shoulder remaining a significant issue. Much of the elbow and shoulder injuries sustained by the pre-adolescent baseball athlete are overuse injuries that may be avoided with proper training and exercise interventions.
The number of reported injuries in baseball has continued to rise throughout all levels of competition.2 In particular we are seeing a larger number of injuries in the youth population than previously. Conte et al. acknowledged that up to 74% of players ages (8-18) report arm pain while throwing with about 23% consistent with overuse.
Medical professionals have done a good job at establishing potential risk factors for injury and have implemented guidelines for youth players and associated personnel to follow. However, little has been documented with regards to preventative arm care programs for the youth population. In an effort to reduce the likelihood of injuries related to overuse the American Sports Medicine Institute provides recommendations regarding risk-prone pitching activities to help reduce the likelihood of injuries related to overuse. These recommendations include (1) no competitive baseball pitching for at least 4 months per year, (2) following limits for pitch counts and rest days, (3) avoiding pitching on multiple teams with overlapping seasons, (4) not playing both catcher and pitcher, (5) playing other sports in addition to baseball, and (6) discontinuing pitching if the pitcher reports pain in the shoulder or elbow.3
Compared to the elite level professional, the youth athlete has unique characteristics, which may alter the way in which arm care programs are developed. These individuals are skeletally immature and often present with reduced core strength, hip strength, posterior chain strength, compromised single leg balance, coordination and scapular dyskinesia. Sakata et al. identified increased risk of medial elbow injury with pitching in those with increased thoracic kyphosis and deficits in elbow extension.4 Previous prospective studies reported altered shoulder range of motion, posterior shoulder tightness,5 rotator cuff weakness,6 scapular dysfunction,7 lower extremity muscle tightness, and deficits in single leg standing balance,8 as physical risk factors associated with throwing injuries of the shoulder and elbow.
The purpose of this manuscript is to discuss the risk factors of injuries in the youth baseball player and to describe a modification of the Thrower’s Ten exercise program that addresses the unique characteristics of the youth baseball player.
Risk Factors
The overhead athlete, particularly overhand pitchers, are at risk for injury due to the aggressive demands of throwing. Throwing, specifically the late cocking and acceleration phase of the pitch, from fully externally rotated cocking to early acceleration in the adult elite thrower, is the fastest functional movement recorded. The internal rotation movement is produced in 0.03 seconds at angular velocities of 7,250 degrees per second, resulting in anterior shear and distraction forces across the glenohumeral joint of 0.5 times, 1.5 times that of the throwers body weight respectively. While strenuous on the entire body, it is for these reasons that much of the injuries seen in throwers manifest themselves in the shoulder or elbow.9
Lyman et al.10 performed a longitudinal study following youth baseball players ages 9 to 12 years old over the course of 2 consecutive seasons. The authors reported older individuals with increased weight and decreased height were at higher risk for injury. Additionally, those who lifted weights, pitched outside of little league (such as during showcase events), and reported decreased self-satisfaction with performance were also at an increased risk. Interesting to note they were able to correlate that there was a 1.5% increased risk of shoulder pain with each pitch thrown, however for every 10 pitches thrown in game there was a 6% increase odds of elbow pain with significant trends per 25 pitches. Based on these findings they suggest that a pitch limit be implemented for 75 pitches, because those who exceeded this count were at 3.2x more likelihood of experiencing shoulder pain.
Following this study Olsen & Fleisig11 reported additional risk factors associated with overhand pitching in the youth population. The study suggests that the primary risk factors for these individuals was pitching with arm fatigue (36x increased risk), over use (80+ pitches per game (increased 4-fold), 8+ months per year (increased 5-fold), starting pitching, showcases or playing outside of little league, 100+ innings pitched) and velocity (85mph+ with 2.58 times risk). Additionally, individuals who were (4cm) taller and (5kg) heavier for their age group were at higher risk of injury and special attention should take place. The authors’ primary suggestion was the importance of long-term health education for all members assisting to care for the individual. The individuals should incorporate an active warm up that includes arm care and aerobic conditioning, not just throwing. They should avoid pitching 80+ pitches per game, 2,500 pitches per year, 8 or more months per year. Lastly, they acknowledge that those under the age of 13 should avoid breaking pitches.
Other studies report the loss in glenohumeral proprioception up to 78% during fatigued throwing.12 Thus an arm care program can be designed to improve endurance and strength of the upper extremity but should encompass the entire body to aid in injury prevention.
The principle predictive risk factor for injury in the overhead athlete is throwing while fatigued. This is supported at the elite, professional level in a study conducted by Murray et al.13 This group documented effects that occur throughout the body such as decreased shoulder external rotation, shoulder adduction torque, and lower extremity knee flexion which in turn led to diminished ball velocity. Despite this documentation Makni et al. reported in a survey that 46% of athletes were encouraged to continue playing with arm pain.14
In a national study of 754 pitchers Fleisig, Yang et al.15 found that; 69.2% reported pitching with arm tiredness, 37.9% with arm pain, 43.5% pitched on consecutive days leading to 4 times greater risk for experiencing tiredness and 2.5 times greater risk for pain, 30% of which pitched for multiple teams with overlapping seasons regardless of the 3 times increased risk of tiredness compared with those who pitched for 1 team, and 20% pitched in multiple games in one day which led to 89% greater odds of experiencing arm pain.
While risk factors for overuse are clearly established, there continues to remain a disconnect between players, coaches, parents and personnel; further stressing the importance of medical education.
Prevention Program
As stated previously the literature concludes that arm care programs are essential to the overhead athlete. However, there is little documentation with regards to specific programming for the youth athlete. Sakata et al.16 aimed to study the efficacy of a prevention program in youth baseball players. The author’s analyzed risk for medial elbow injury in males and females ages 9 to 12 who played either pitcher, another position or both. Based on their findings; total shoulder rotational motion, hip internal rotation range of motion, and thoracic kyphosis angle were the primary modifiable risk factors for medial elbow injury. They created a program consisting of 9 stretching and 9 strengthening exercises aimed to improve these areas. 305 (male and female) players, ages 8 to 11 were included with 136 allocated to the intervention group and 169 for the control. The intervention group performed their program at a minimum of once per week and both groups followed up with physicians every 3 months. Results indicate a significantly lower incidence rate of medial elbow injury, improved total range of shoulder rotation (dominant side), hip internal rotation (nondominant side), shoulder internal rotation deficit (bilaterally), lower trapezius muscle strength (dominant side) and thoracic kyphosis angle. These results, while promising, do not analyze a homogenous population which led the authors to develop a program of their own.
The Thrower’s Ten Program, established by Wilk et al.17, is an evidence-based exercise program for the overhead athlete. This program utilizes isotonic movements that are derived from electromyographic research to specifically address vital muscles involved in the throwing motion. In 2011 Escamallia et al.18, reported that participating in this program for 6 weeks enhanced athletic performance by indicating approximately 2% increase in ball velocity. While the documented results are beneficial, they are indicated for an older population.
A recent clinical consensus by Matsel et al.19 suggests that youth overhead throwers should participate in an arm care program that addresses the entire kinetic chain through a multiphasic approach. This article presents a variation of the Throwers Ten Exercise Program, which has been utilized with excellent results in clinical practice and athletic performance training. The purpose is to incorporate the entire kinetic chain in a simple, easy to follow manner, to prepare the youth population for the demands of overhead activity.
The Youth Throwers Ten Exercise Program outlined in this article contains alterations to a previously outlined Throwers Ten Exercise Program by Wilk et al. This new program emphasizes technique and movement awareness, where individuals will frequently be cued to maintain a posteriorly tilted, externally rotated, and retracted scapula. All exercises performed involve the use of body weight or a single piece of theraband and thus can be performed by all individuals. The individual is instructed to perform 2 sets of 10 repetitions for each exercise with minimal to no rest between movements.
The Youth Throwers Ten Exercise Program begins with IR and ER theraband exercises at 0 degrees of abduction with a towel roll between the individual’s arm and side. Reinold et al.20 documented greater electromyographic activity of the posterior cuff musculature when the towel roll is used. The idea is that the shoulder will be placed into slight abduction and the authors suggest that if a player does not have a towel that they substitute with the use of their glove.
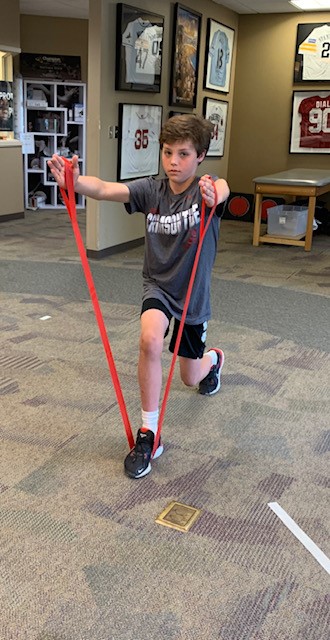
Next is the full-can from a split stance lunge (Figure 1). The exercise set up begins with the individual in half kneeling with a piece of theraband under their lead leg with the ends in each hand by their sides. They are next instructed to partially stand up holding an isometric lunge position, maintaining 90-degree hip and knee flexion angles in their lead leg, neutral extension with 90-degree knee flexion angle in their trail leg, upright posture and scapula positioning as previously described. While holding this position, they are instructed to raise both arms, with straight elbows and thumbs pointed upward, to shoulder height at 30-degree angles holding for 2 seconds at the apex of the movement and slowly lowering to the starting position. To perform the second set the athlete will switch their footing such that their lead leg in the first set will now be their trail leg in the second, and vice versa. The purpose of the sustained split stance lunge position is to elicit activation of the entire kinetic chain, particularly the gluteus medius; which is reported to have high activity during early acceleration and ball release.21

This is followed by shoulder abduction to 90 degrees from a split stance lunge. This will be performed in the set up described for the full-can but the individual will raise their arms to shoulder height, with elbows extended and palms facing down. If the individual does not have access to a theraband they can use their glove, a baseball or a combination of the two for resistance.
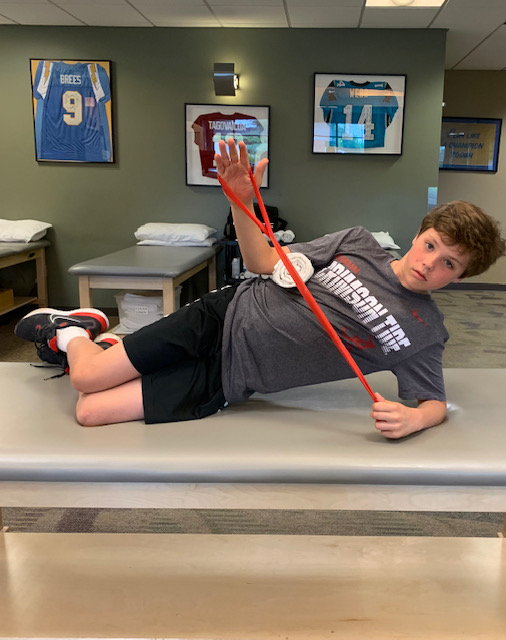
Side-lying ER is performed with a theraband under the floor-side arm and may be progressed to a modified (knee-bent) or standard side plank position to challenge the athlete (Figure 2). Caution must take place to ensure that the athlete has the dynamic stability required to support the weight of their body and perform the task with neutral spine alignment.

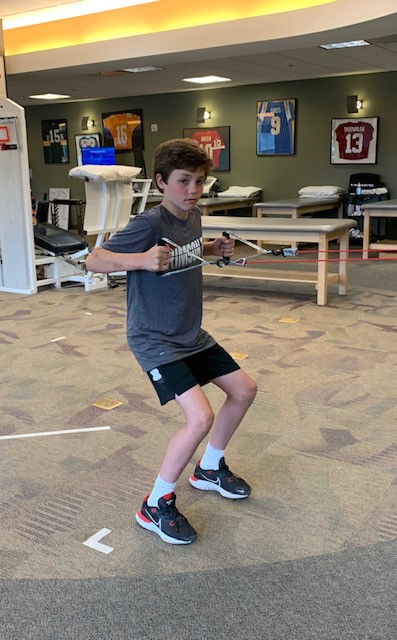
The following three exercises are all to be performed while standing in a partial squat position. The athlete should flex at the hips and knees to 90 degrees, maintaining an upright trunk with scapula posteriorly tilted, externally rotated and retracted to improve coordination between the muscles of lumbo-pelvic hip complex and scapula musculature. The theraband should be anchored to the backstop fence or held by a partner. The first of three exercises is low rowing (Figure 3), followed by the modified robbery (Figure 4), and a high row at 90 degrees abduction into 90 degrees of external rotation. These exercises aim to enhance scapula neuromuscular control via synchronicity of muscle firing for scapulothoracic musculature. A lack of scapular muscle synchronicity, particularly of the lower and middle trapezius, is a key factor in overhead athletes with shoulder pain.22 To address the remainder of the upper extremity and protect the individual from the inherent stresses on the elbow joint during the throwing motion, elbow strengthening exercises such as biceps curls, triceps extensions, and wrist/forearm four-ways (flexion, extension, pronation, supination) with theraband are to be performed.


The final two exercises aim to address the entire kinetic chain, specifically the diminished lower extremity neuromuscular coordination and reduced core strength commonly seen in the youth athlete. The single leg squat or front-step down (Figure 5) is an exercise that doubles as a clinical exam used to assess balance, coordination, neuromuscular control and strength.

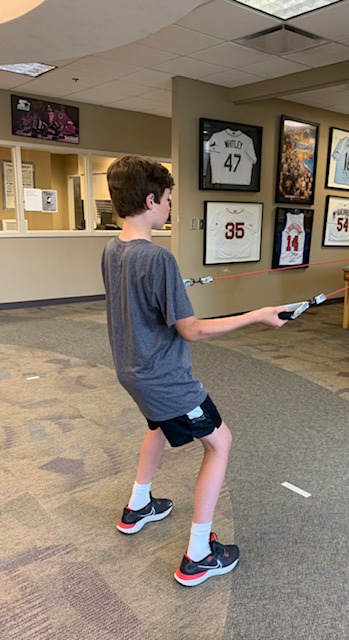
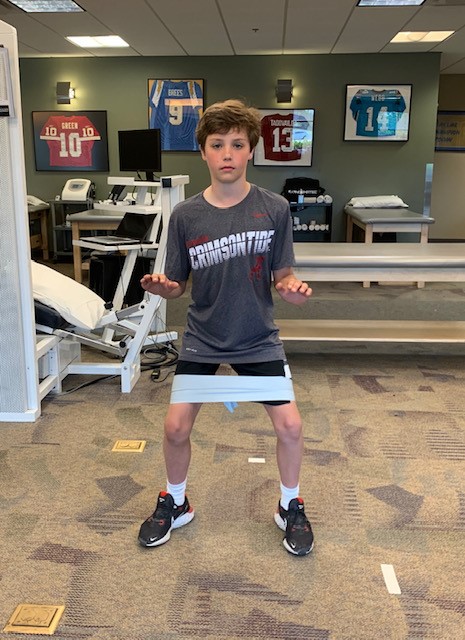
Common faults seen with this task are trunk lean (torso outside of the individual’s base of support), dynamic knee valgus “wiggle-wobble” and excessive pronation. The coach or supervisor should be aware and able to correct or cue the individual performing the task out of these positions. Lastly the athlete is to perform a lateral slide with theraband (Figure 6) which has high electromyographic activity for gluteus medius.23 The theraband is to be placed around the individual’s knees and progressed towards the feet as they gain strength. The athlete should be instructed to perform a partial squat position and side step slowly, keeping tension on the band and the height of the squat.

Summary
Overhead throwing is a physically demanding task and typically leads to upper extremity injuries. In recent years there has been a rise in the frequency and likelihood of these injuries. It is imperative that coaches, parents and youth are educated on ways to safely, efficiently and effectively train for the demands of their activity. The Youth Throwers Ten Program presented in this article provides a framework for these individuals to properly prepare for competition.