




INTRODUCTION
It is well known that athletes are at risk for foot and ankle injuries. These include injuries in the forefoot, defined as the region of the foot distal to the tarsometatarsal joints. The forefoot, unlike the mid- and hindfoot, is unconstrained with movement occurring freely in all three planes. Because the forefoot is the most distal weight bearing segment of the lower extremity, it can undergo a substantial amount of stress and strain, and can be affected by footwear, terrain, and biomechanical factors in the entire lower kinetic chain. Despite the prevalence of forefoot related problems in athletes, there are few comprehensive summaries on examination and intervention strategies for those with forefoot related symptoms. The purpose of the clinical commentary is to integrate a movement system approach in pathoanatomical, evaluation, and intervention considerations for athletes with common forefoot pathologies, including stress fractures, metatarsalgia, neuroma, and sesamoiditis.
Anatomy of the Forefoot
The forefoot is composed of five rays that are functionally divided into a medial component, including the first metatarsal and great toe (hallux), and the lateral component, consisting of metatarsals and toes two to five. The distal aspect of the medial longitudinal arch is formed by the first metatarsal. The first tarsometatarsal and Lisfranc articulations join the midfoot to the forefoot, with these joints being supported by a dense interconnection of dorsal and plantar tarsometatarsal, intermetatarsal, and Lisfranc ligaments. Distally, the hallux is joined with the first metatarsal by the first metatarsophalangeal (MTP) joint and is supported by the joint capsule and plantar, medial collateral, and lateral collateral ligaments. The five rays of the forefoot are supported by a tensed interconnection of ligaments, joint capsules, and fascia that create a transverse arch.1 This interconnected weave of tissue includes the plantar plate, which is a fibrocartilaginous structure that runs from each metatarsal head to the respective proximal phalanx. The plantar plate also serves as an attachment for the plantar fascia and supports the transverse arch.1
While it is recognized that abnormal function of the medial longitudinal arch can affect lower extremity biomechanics and contribute to pathology, abnormalities of the transverse arch and forefoot may also affect lower extremity biomechanics and contribute to pathology. Robberecht et el.1 found collapse of the transverse arch to be associated with forefoot pathology. During the propulsive phase of gait, representing the last 30% of the stance phase, only the forefoot is in contact with the ground. Consequently, abnormal forefoot biomechanics may negatively affect the entire lower extremity during propulsion. Likewise, any abnormal biomechanics in the lower extremity can affect propulsion and contribute to forefoot pathology. A comprehensive examination and intervention plan for forefoot pathologies therefore needs to consider the entire lower extremity and how biomechanical abnormalities may affect movement and thus contribute to symptoms.
Biomechanical Considerations
While many factors may contribute to pathology and injury, the presence of abnormal foot alignment can negatively affect lower extremity biomechanics and be associated with injuries.2–8 Abnormal pronation is typically defined by excessive calcaneal eversion, plantarflexion and adduction of the talus, collapse of the medial longitudinal arch, and abduction of the forefoot on the hindfoot. Abnormal pronation has been associated with increased foot mobility, collapse of the transverse arch, and compensatory knee and hip medial rotation.9,10 Abnormal supination is typically defined by excessive calcaneal inversion, dorsiflexion and abduction of the talus, high medial longitudinal arch, and adduction of the forefoot on the hindfoot. This foot type is usually more rigid and may be associated with compensatory knee and hip lateral rotation.9,10 Altered movement patterns caused by abnormal pronation and supination may be identified during static standing, gait, and functional movement testing. The single leg squat and step-down tests are functional movement tests that can be used to assess neuromuscular control and identify potential impairments of the trunk, pelvis, hip, knee, and ankle with evidence of reliability and validity to supports its use.11,12 Because the step-down test may place a greater emphasis on ankle motion, it may be a better measure than the single leg squat test in those with foot and ankle pathologies.13 Compensatory lower extremity movements can be identified and characterized as being associated with abnormal pronation or supination during gait and functional movement assessment. Physical therapists may use the general characteristics associated abnormal pronation or abnormal supination to describe the movement system disorder and serve as a guide for evaluating and managing athletes with common forefoot pathologies such as stress fractures, metatarsalgia, neuroma, and sesamoiditis.
FOREFOOT PATHOLOGIES
Stress fracture
Stress fractures are microscopic bone injuries resulting from repeated bouts of physiological overload without adequate time for tissue remodeling and adaptation.14,15 Athletes who have a sudden increase in weight bearing activities are at risk for a stress fracture, with runners and military recruits seemly being at higher risk.16–20 The shafts of the metatarsal bones are common locations for stress fractures, with the occurrence at the second and third metatarsals being more common than at the fourth and fifth.15–17,19 Athletes with a movement system diagnosis of abnormal supination may be at risk for metatarsal stress fractures because of the reduced ability to attenuate weight bearing stressors associated with a more rigid foot. An abnormal pronation movement system diagnosis can also increase the risk of sustaining a stress fracture because of atypical loading pattern associated with a more mobile foot.15,21,22 Increased risk for stress fracture has been associated with poor pre-participation condition, older age, female sex, Caucasian race, decreased bone density, hormonal and menstrual abnormalities, low calorie and low fat diet, inadequate sleep pattern, and collagen disease.22 Athletes with a stress fracture may complain of an insidious onset of chronic aching pain that is activity related and associated with an increase in weight bearing activity or training intensity.22,23 Examination should find the involved metatarsal shaft to be tender with palpation.23 Stress fractures of the second and third metatarsals generally heal well requiring only activity modification without a reduction in weightbearing.14 Stress fractures of the proximal intermediate zone of the fifth metatarsal are considered high risk for delayed healing or non-union and require more restrictive weight bearing, partial immobilization, and may progress to surgery if healing does not occur.14 Imaging such as radiographs or MRI may be necessary to identify and grade stress fractures. Higher grade stress fractures may require 16 or more weeks of activity modification while lower grade stress fractures may improve with just three weeks of relative rest.24 Treatment for stress fractures should include modifications of factors that contributed to the injury.14,22,25 A comprehensive lower quarter biomechanical examination and a sport-specific movement analysis will help identify and guide treatment to address contributing factors such as leg length discrepancy, abnormal foot posture, lower extremity malalignment, muscle imbalance, flexibility insufficiency, and range of motion (ROM) deficits. Athlete education should address any training errors, improper diet, or inadequate sleep patterns that are identified. Relative rest with low/non-impact aerobic activity, stretching and strengthening exercises, and immobilization in a removable boot are generally recommended until the pain resolves.22 Training can resume with a 10% increase in intensity per week after the patient has been pain free for 10–14 days.26
Metatarsalgia
Metatarsalgia is a non-specific diagnosis given to athletes with pain on the plantar aspect of one or more of the metatarsal heads that is exacerbated by physical activity, barefoot walking, and/or walking in shoes with an elevated heel. This condition typically results from repetitive overloading of the metatarsal head(s) due to anatomic or biomechanical abnormalities such as first ray hypermobility, hallux abducto valgus (HAV), ankle equinus, claw or hammer toe deformities, lesser MTP joint instability, atrophy of the plantar fat pad, and/or improper footwear. A movement system diagnosis of abnormal pronation or supination may also contribute to overload the development of metatarsalgia because of altered loading of the metatarsal head. Athletes, particularly middle-aged females, may note a gradual onset of pain related to a rapid increase in training intensity, inappropriate shoe wear, or a change in running terrain. Examination should identify local tenderness at the metatarsal head and possibly a prominent metatarsal head(s). Muscle imbalance, ROM deficits, and/or biomechanical abnormalities in the lower quarter that may contribute to overloading the metatarsal heads should be identified and corrected. Assessing for and addressing any loss of ankle dorsiflexion ROM should be a primary focus. Treatment can also include orthoses, a metatarsal pad, and shoe modifications which may promote redistribution of plantar pressures and reduce pain. Taping to redistribute the plantar fat pad with or without techniques to correct hammer or claw toe deformity, when appropriate, may be beneficial (Figure 1A-B).

Neuroma
An interdigital neuroma (Morton’s neuroma) is a mechanical entrapment neuropathy of one or more of the interdigital nerves in the forefoot. The nerve may become enlarged because of fibrotic tissue and/or endoneural edema. This condition primarily involves the third common (64%–91%) digital branch of the medial plantar nerve between the third and fourth metatarsal heads, followed by the second (18%–31%), first (0%–2.5%), and fourth (0%–6%) interdigital nerves.27–29 Runners and dancers are especially susceptible to interdigital neuroma due to repetitive hyperextension and longitudinal metatarsal torsional trauma at the MTP joints and resultant tissue thickening and swelling which may compress the nerve.30 Narrow shoes, over-training with repetitive MTP extension are the primary risk factors for developing an interdigital neuroma.31 A movement system diagnosis of abnormal pronation may also contribute to the development of a neuroma. Athletes with abnormal pronation and a hypermobile foot may be a higher risk because of the narrower intermetatarsal space associated with a collapsed transverse arch. Signs and symptoms of interdigital neuroma typically begin insidiously and include neurogenic pain in the plantar aspect of the forefoot.32 The pain may be associated with tenderness, cramping, burning, tingling, and/or numbness in the toes of the involved interspace. Some athletes will report a sensation of walking on a lump.27,33–35 During the examination, manual compression of the transverse arch and Mulder test should reproduce symptoms in athletes with interdigital neuroma.36 In athletes with chronic interdigital neuroma, weakness of the intrinsic muscles may be present. Interventions such as shoe modifications, such as custom orthotics, rocker-bottom shoes, the use of a wide toe box, and metatarsal head unloading with a metatarsal pad may also be helpful at decreasing symptoms.27,30,33,37,38 Metatarsal mobilization (Figure 2) and taping to correct abnormal pronation and promote the transverse arch for patients with interdigital neuroma.

Sesamoiditis
Hallux sesamoid syndrome, or sesamoiditis, are nonspecific descriptive terms referring to pathologies, anatomical anomalies, or adaptive changes of the sesamoid bones. These injuries are associated with inflammation of the peritendinous structures of the sesamoids and possible osteochonditis.39–41 Most sesamoid injuries are overuse injuries, but direct trauma or forced extension of the hallux can cause an acute injury. Overuse of the sesamoids and the supporting structures can occur with repetitive activities such as running, jumping, tennis, and ballet. Those with an abnormal supination movement system diagnosis may be at risk to overload the sesamoids because of the associated high arch and plantar flexed first ray. Symptoms of sesamoiditis include pain that occurs with weight bearing, direct palpation, or with passive extension of the first MTP joint. Forefoot swelling,40 tenderness, crepitus, decreased strength of the flexor hallucis longus and brevis tendons,41,42 decreased extension of the first MTP joint, and impaired first ray and/or first MTP joint mobility may also be present.39,43,44 Decreased sesamoid mobility or abnormal position of the sesamoids may also be determined during palpation by comparing sesamoid position between the involved and uninvolved sides.41,42 Interventions for sesamoiditis should focus on unloading the sesamoids and forefoot or protecting the first MTP joint.45 Orthotics can be used to decrease the load on the involved sesamoid and foot and may include a cut-out for the sesamoids, metatarsal bars, a rigid shank, and/or a first metatarsal extension.39 Taping of the sesamoids can help improve forefoot position and function and may decrease shear forces on the sesamoids and plantar aspect of the forefoot.42 If malposition or decreased sesamoid mobility is found, corrective sesamoid mobilizations and/or taping can be implemented (Figure 3).

EVALUATION AND TREATMENT TECHNIQUES
A comprehensive examination of an athlete with forefoot pathology should include a comprehensive assessment of the foot and ankle as well as static standing, gait, and functional movement evaluations. An appropriate lower quarter screen may also be needed to identify potential contributing impairments. A standard examination can consist of range of motion and strength assessment of the lumbosacral spine, hip, knee, ankle, and foot, with select special tests being used based on the athlete’s history and potential differential diagnoses. Specific attention should be directed toward ankle dorsiflexion ROM, assessing for potential limitations in gastrocnemius-soleus flexibility, and talocrural joint posterior capsule mobility. The weight bearing lunge test can be used as a functional measure of tibiopedal dorsiflexion, with ROM coming from not only the talocrural joint but also the subtalar and midtarsal joints as well.46 An assessment of great toe extension ROM in weightbearing and non-weightbearing should include evaluating mobility of the first ray tarsal-metatarsal joint, first MTP, and sesamoids. Likewise, assessment of hindfoot and forefoot ROM should include evaluating subtalar, calcaneocuboid, and talonavicular joint mobility. Because foot alignment is commonly associated with forefoot pathology,2–8 the Foot Posture Index-6 (FPI-6) can be used to assess static weight bearing alignment in the sagittal, frontal, and transverse planes and classify foot type as being normal, abnormally pronated, or abnormally supinated (Table 1).47 A total score of 0 to +4 on the FPI-6 indicates a normal foot posture in adults.8 Gait assessment, single leg squat test, and the step-down test can be used to identify abnormalities in the movement system. The findings from this comprehensive examination of the entire lower quarter will identify impairments and generate a prioritized, objective problem list that can be used to develop an intervention plan within the context of the specific forefoot pathoanatomical diagnosis. The results of the FPI-6 and movement examination can identify a movement system diagnosis of abnormal pronation or supination to assist in directing intervention strategies.
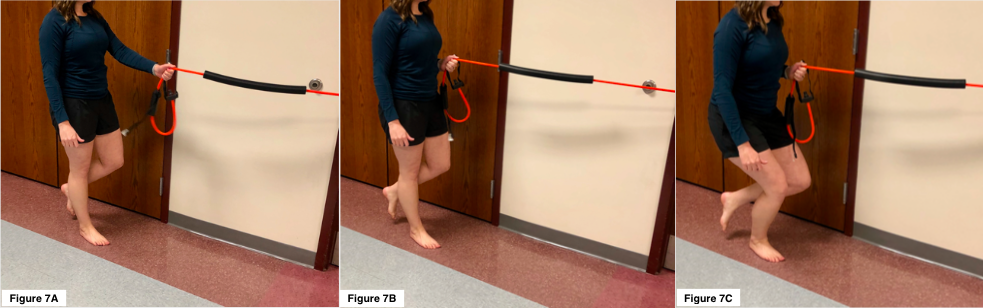
Forefoot pathologies can be difficult to diagnose and often present with common impairments and movement system disorders. Using a prioritized, objective problem list and movement system diagnosis will place less emphasis on a pathoanatomical diagnosis-based treatment plan and more emphasis on the identified impairments and abnormal movements. Athletes with an abnormal pronation movement system diagnosis typically demonstrate foot hypermobility, have decreased strength of the tibialis posterior muscle, and present with a medially rotated position of the lower extremity. Treatment for those with abnormal pronation can include a grade V mobilization to the navicular to facilitate tibialis posterior function (Figure 4A-C) and antipronation taping to support the medial longitudinal arch (Figure 5A-D). Neuromuscular reeducation and strengthening exercises can be directed at the intrinsic and extrinsic foot muscles that support medial longitudinal and transverse arches. These exercises can also work to correct the medially rotated lower extremity and stabilize the hip and lumbosacral spine. The single leg squat with proximally resisted hip lateral rotation (Figure 7) can be used to facilitate the tibialis posterior, hip lateral rotators, hip abductors, and lumbosacral spine stabilizers. Athletes with abnormal supination movement system diagnosis typically demonstrate foot hypomobility, decreased strength of the fibularis muscles, and a laterally rotated lower extremity position. Treatment for those with abnormal supination can include joint mobilizations to improve foot mobility, with an emphasis on improving lateral subtalar glide (Figure 8). Exercises to facilitate fibularis activity and foot pronation while engaging the trunk and hip musculature can include the outward pivot (Figure 9A-B). The characteristics, select treatment techniques, and forefoot pathologies associated with abnormal pronation and supination movement system disorders summarized in the Table. Joint mobilization, taping technique, and exercise should be appropriately selected based the athlete’s impairment and movement system diagnosis while considering their unique treatment goals and desired outcome.



CONCLUSION
Forefoot injuries are common in athletes because of the stress and strain that occur during competition and training. Many biomechanical factors can contribute to forefoot symptoms and therefore a thorough examination, that includes a functional movement assessment, should be performed in order to identify contributing factors throughout the entire lower quarter. An evaluation should include a comprehensive history with a description of training and competition regimen, as well as a systematic examination for the entire quarter to identify impairments and generate a prioritized objective problem list. Using a movement system diagnosis of abnormal pronation or supination may also help in directing treatment to correct the associated abnormal movements.
CONFLICTS OF INTEREST
The authors have no conflicts to disclose.
DISCLOSURES
This study received no funding