
INTRODUCTION
The analysis of human movement is central to the practice of physical therapy. Physical therapists analyze movement in order to identify impairments that contribute to activity limitations and participation restrictions in their patients. Movement analysis and interpretation is a hallmark skill of expert practitioners.1
The movement system was adopted by the American Physical Therapy Association in 2015 and has been defined as the integration of body systems that generate and maintain movement at all levels of bodily function.2 There have been several approaches to defining the movement system,3–5 but the 4-Element Movement System Model (4-Element Model) has the advantage in that it captures a wide variety of disorders, can meaningfully guide practice and education, can readily be incorporated into entry level and residency training, and is consistent with existing professional models such as the International Classification of Functioning (ICF)6 and the Patient-Client Management Model.7
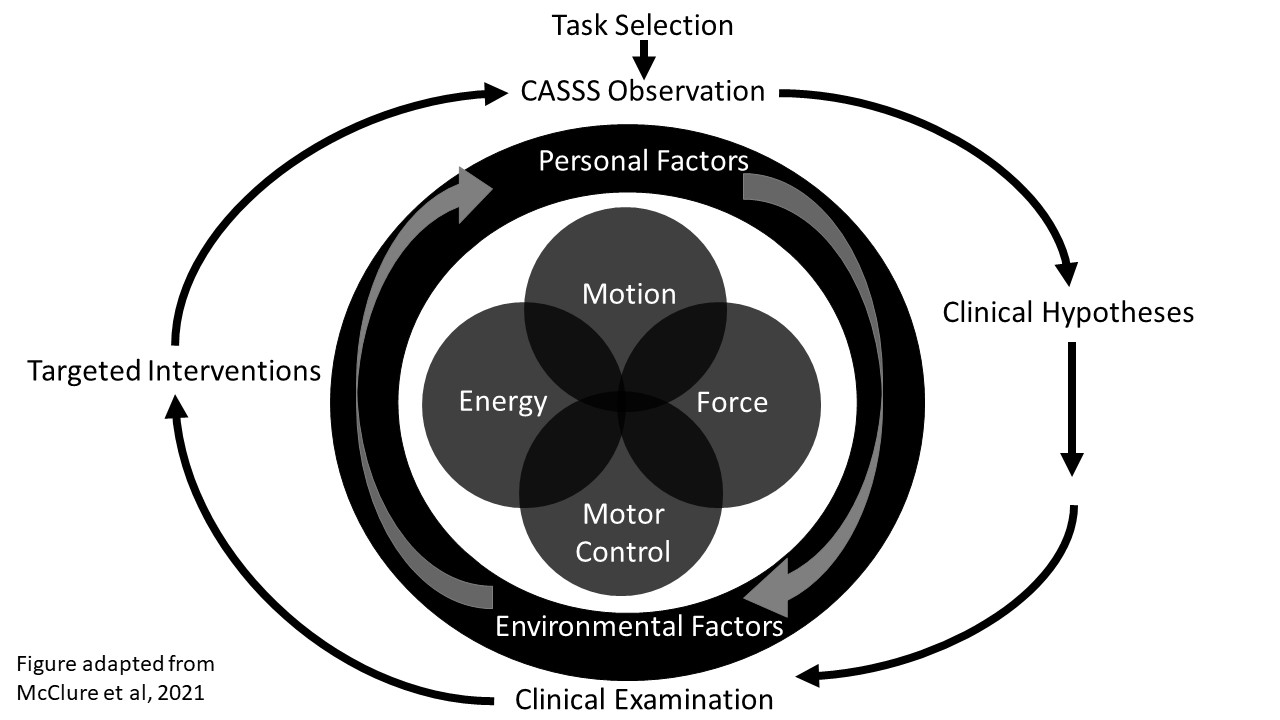
The 4-Element Model describes the primary elements essential to all movement: motion, force, motor control, and energy (Figure 1). Motion refers specifically to the ability of a joint or tissue to be moved passively. Force refers to the ability of the contractile (i.e. muscles) and non-contractile structures (i.e. tendons) to produce movement, and provide dynamic stability around joints during static and dynamic tasks. Motor control refers to the ability to plan, execute and adapt goal-directed movements such that they are accurate, coordinated and efficient. Lastly, energy refers to the ability to perform sustained or repeated movements, and is dependent on the integrated functioning of the cardiovascular, pulmonary, and neuromuscular systems. The elements overlap in many patient conditions, but can be examined and tested separately. Since all movement occurs within an environmental context and is affected by personal factors specific to the individual, the model depicts how the environment and personal factors surround the 4 elements. Environmental factors are external items that can influence movement such as terrain, support surface, and external distractions. Personal factors include age, gender, comorbidities, self-efficacy, confidence, fear of movement and motivation.5 The comprehensive description of movement in the 4-Element Model is consistent with theories of human movement being a dynamic system involving complex interactions between the task, the person, and the environment.8

Application of the model begins with the identification of an activity or task that the patient will perform, and consists of qualitative observation leading to hypothesis generation. The 4-Element Model encourages a systematic approach to the observation by using five observation targets abbreviated as CASSS (control, amount, speed, symmetry, symptoms). Briefly, control refers to the smoothness, coordination, and timing of movement; amount refers to the amplitude of movement at each joint; symmetry is observed in bilateral tasks or comparing unilateral performance between limbs; speed is the length of time; and symptoms most commonly refer to pain but also can include mechanical symptoms, reports of instability, or fatigue. After using the CASSS observation targets to describe the task, hypotheses are generated about the possible movement system elements that may contribute to the movements observed. Potential impairments are identified and tested which lead the clinician to implement treatment strategies.5 This commentary will address the application of the 4-Element Model to sports physical therapist practice, and its incorporation as part of the education of students and residents.
USE OF THE 4-ELEMENT MODEL IN EDUCATION
Case-based learning with the 4-Element Model is foundational in both the Arcadia University entry-level Doctor of Physical Therapy (DPT) and Orthopedic Residency programs. The model can be incorporated by academic faculty, clinical instructors (CIs), and residency mentors to assess and foster development of clinical reasoning of the learner. The focus of introducing the model in the entry-level DPT program is to help build decision making strategies before entering the clinical education curriculum. The model, terminology, and process are introduced in the first course of the curriculum and applied throughout the rest of the courses in the program. The repetition of 1) activity selection based on patient goals and safety, 2) use of observational targets, and 3) hypothesis driven exam and intervention design is a scaffold by which the student develops clinical reasoning in the didactic curriculum. It is this repetition that helps support the student when they enter the clinical environment and fosters the use of a common examination process and common language to explain the movement impairments with their CI.
Clinical Education
In order to facilitate successful clinical education experiences, the department’s clinical education team has provided clinical faculty with the published paper and a narrated video, as resources to educate them on the 4-Element Model.5,9 The video describes the 4-Element Model and applies it to a sample case of a young athlete with a knee injury. The paper and video help to share insight into the student’s foundational clinical reasoning strategies. We believe this knowledge may allow the CI to more accurately meet the student where they are and provide concrete tools for development. We encourage clinical sites to use the model as a conceptual and visual cue for clinical teaching and reflection in all levels of clinical education experiences, from beginner to terminal clinical affiliation. A CI may utilize specific components of the model in patient care preparation activities such as helping the student to identify meaningful goals that then drive observational targets. It is also beneficial to use the model as a cue to identify personal or environmental factors which may impact care, and therefore encourages an awareness of safety early on in any clinical experience. The CI may assist the student in streamlining the physical examination by discussing the element(s) contributing to the observed deficits and how each may be tested. To help develop basic clinical reasoning skills a CI may provide detailed prompting questions using common language such as “if this were a force problem, what is the relevant anatomy to test?” or “how do the elements of force and motor control interact during this jumping sequence?” Plan of care development can be facilitated by revisiting the outcomes of hypothesis testing with the student to develop targeted interventions, and using these outcomes in reflection activities. CI’s may also use the 4- Element Model to advance non-linear thinking, the interaction between elements and systems, which is imperative when treating more specialized populations such as the athlete.
Post-graduate training
A primary focus of a post graduate training program is to facilitate a partnership relationship with mentor and resident/fellow and to help the learner delve deeper into specialty practice for optimal patient care. A challenge with mentoring relationships in residency and fellowship education is that we do not use a common language or examination framework across physical therapy programs and practice. Frequently mentors and learners may have different backgrounds of education and training. The 4-Element Model provides a common framework for a systematic movement assessment of the athlete.
To implement the model, the resident and mentor start the examination by choosing and analyzing a specific functional task. The task is selected by what the patient reports having difficulty performing in their daily activities or sport specific tasks. We have found it beneficial to film the patient performing the challenging task such as a stair climbing, gait assessment, squatting mechanics, overhead throwing or jumping. Filming allows the mentor and resident to slow the patient’s performance to fully assess movement abnormalities. While looking at the specific functional task, the mentor will ask the resident to assess the observation targets listed in the CASSS. For example, limitations in control would prompt a discussion of what could be affecting the lack of control including poor balance, specific muscle weakness or a patient’s decreased awareness of how to perform the movement. If the resident observes a limited amount of motion this would then prompt discussion of which joints specifically to look at further in the examination of mobility. Speed impairments would prompt a discussion of incorporating a timed functional test or discussion of the “normal” parameters for someone to complete the task (30 second sit to stand test, timed up and go). Symmetry issues would prompt discussions such as “why might a weight shift occur?” Symptom provocation during movement such as pain, clicking, or stiffness and when in the movement sequence these symptoms occur would prompt a mentor and resident to perform a more specific biomechanical assessment. After hypotheses are generated, the novice clinician would continue with the examination delving deeper into the areas of deficit. The mentor and clinician would then use the examination findings to decide which specialty interventions best help that area of deficit. In a post graduate mentoring relationship, the cases that are often discussed have complex clinical presentations, and likely more than one element needs to be addressed to optimize function. It is recommended to return to the specific functional task frequently to assess if the physical therapy interventions are translating into improved functional movement with the limited task.
It is our belief that use of the 4-Element Model in education can be beneficial to both the learner and CI/mentor to help assess and solidify clinical reasoning. This may be demonstrated in entry-level DPT programs, as we look to scaffold learning and build initial reasoning processes, and in post graduate education as we guide novice clinicians to more effective and specialized care.
APPLICATION OF THE 4-ELEMENT MODEL TO CLINICAL CASE EXAMPLES
The 4-Element Model provides a systematic approach to the understanding and management of movement dysfunction for common musculoskeletal conditions that are encountered regularly in sports medicine and orthopedic physical therapist practice. The four elements of the movement system model are essential to all athletic type functional tasks. In the following sections, three clinical case examples will be presented to show how the 4-Element Model and CASSS framework can be used to establish testable clinical hypotheses for observed movement impairments. The findings can then be applied to help develop patient specific treatment plans aimed at improving functional task performance, and can also be used to guide overall clinical decision making.
Case Example 1: Female Soccer Player Post-Operative ACL Reconstruction (ACLR)
Marie is a 23-year-old female college student. She ruptured her left anterior cruciate ligament (ACL) while playing soccer. She reported a non-contact injury in which her knee buckled upon attempting to change directions while playing defense. She underwent ACL reconstruction (ACLR) with a quadriceps tendon autograft approximately three weeks after the injury. Acute post-operative effects of effusion and pain, which contribute to limitations in motion and force, are readily observed as the patient enters the treatment room. These findings guide initial treatment. However, once post-operative sequelae are resolved, functional tasks with increased physiologic demand are appropriate to examine. After six weeks of post-operative treatment, motion was restored and strength training was progressed.
Task selection: As closed chain exercises progressed from bilateral to unilateral movements, a lateral step down (8-inch step) was chosen as the task to examine as it was challenging to the patient (see links in reference for video).10,11
CASSS & Key observations: In the sagittal plane, Marie demonstrated good control during the task; however, in the frontal plane, she demonstrated slightly less control of the lower extremity on the right (nonsurgical) side. When examining motion, she demonstrated the appropriate amount of motion through the lower extremity and trunk in the sagittal plane; but in the frontal plane, she demonstrated slightly greater amount of hip adduction on the right (nonsurgical) side during the task which was most apparent towards peak knee flexion. Marie demonstrated normal speed during the task. She exhibited symmetry in the sagittal plane, but in the frontal plane she appeared asymmetric in the control and amount of motion, as described prior. Marie did not report any symptoms of pain, stiffness, or instability during the task. Based on the observational targets of the CASSS, Marie demonstrated slightly greater hip adduction, or greater dynamic lower extremity valgus, in the right (non-surgical) limb compared to the left limb.
Hypotheses and Exam: Hypotheses regarding this movement alteration included: 1) force impairment, weakness in the muscles controlling hip adduction; 2) motor control impairment, perhaps lower extremity valgus decreased in the left (surgical) limb due to extensive unilateral training and feedback; and 3) motion impairment, limited ankle dorsiflexion (DF) in the right limb.12 Based on the observational targets and hypotheses our evaluation included strength testing of the hip abductors and ROM evaluation of ankle DF. Our evaluation revealed symmetrical hip abduction strength and symmetrical DF ROM. Based on the evaluation of Marie’s strength and ROM, we concluded that Marie’s asymmetric performance of the lateral step was a result of learned behavior from extensive unilateral training. Discussion with Marie confirmed this as she was provided with cues to minimize lower extremity valgus throughout post-operative rehabilitation and did not perform substantial exercises with the nonsurgical limb.
Task selection: We chose to observe Marie performing a 32 cm drop vertical jump (DVJ) (see links in reference for the video).13 The DVJ task was chosen as it may help identify athletes with a higher risk of knee re-injury or second ACL injury.14–16
CASSS & Key observations: Marie’s control of the movement was smooth and coordinated. In the sagittal plane, she demonstrated a significant amount of hip and knee flexion and a forward trunk position. In the frontal/transverse planes, the amount of motion at the hip was greater on the left (surgical) side. Marie’s speed during the task was normal. From a symmetry perspective, Marie demonstrated asymmetrical loading between the limbs. Specifically, she shifted her weight away from the left (surgical) limb. Marie did not report symptoms during the DVJ. Based on the observational targets, the most significant movement alteration was asymmetrical loading, characterized by greater weight acceptance in the right (non-surgical) lower extremity.
Hypotheses and Exam: Hypotheses regarding this movement alteration included: 1) force impairment, weakness in the surgical limb’s quadriceps muscle may be present; 2) motor control impairment, learned behavior resulting off-loading the surgical limb since the injury, after ACLR, and/or during the rehabilitation process, and 3) psychological factors including readiness to return to sport, confidence, and fear of re-injury. Our evaluation with an isokinetic dynamometer revealed a quadriceps strength index of 85% (L peak torque/body weight = .82 Nm/kg; R peak torque/body weight=.96 Nm/kg). To determine whether motor control alterations were contributing to the asymmetrical loading pattern, Marie performed the drop vertical jump after being provided with external feedback. The external feedback was reaching (with her left hand) for a cone placed to her left. Marie demonstrated more symmetrical loading with the provided external feedback. Also, Marie completed the anterior cruciate ligament return to sport after injury questionnaire (ACL-RSI), scoring a 4/100. Lower scores indicate less psychological readiness (i.e. more fear, less confidence, more concerned about future risks of knee injury). Based on the findings from the evaluation, Marie’s altered loading strategy seemed to be driven primarily by altered motor control and personal factors (i.e. poor psychological readiness). A force impairment (i.e. quadriceps weakness) was likely also contributing to the altered movement. A single assessment of the DVJ, or any other single assessment task, did not allow us to determine if there was potentially an impairment with the energy element. Subsequent testing of Marie’s movement during the DVJ or lateral step down could be evaluated after a fatigue protocol or with repetitive tests/movements. Repetitive tests appropriate for Marie would be the two-minute lateral step down test or the Tuck Jump Test.17,18
Targeted intervention: Treatment focused on motor control strategies, such as providing external cueing to promote symmetrical loading during various movement patterns following a graded exposure paradigm. Graded exposure was utilized to address low psychological readiness. Quadriceps strengthening exercises were also continued.
Case Example 2: Achilles Tendinopathy in a Runner
JP is a 37-year-old male accountant who presented with complaints of an insidious onset of right Achilles tendon pain for the past six months. He denied any significant past medical history, but reported prior right distal iliotibial band pain approximately two years ago which resolved without formal medical attention. JP denied any other symptoms other than Achilles tendon pain, with noticeable pain in the morning upon waking which increases with walking and running. His pre-injury running weekly mileage was 15 to 20 miles per week, but now currently running five to seven miles per week. JP reported pain of 0/10 at rest, and 6/10 at worst on the numeric pain rating scale; he scored a 67/80 on the Lower Extremity Functional Scale and 25/36 on the University of Wisconsin Running Injury and Recovery Index. No diagnostic imaging of the right Achilles tendon was reported. The patient reported taking ibuprofen as needed for pain management.
Task selection: His movement assessment began with examining basic bilateral (ie. squats, lunges) and unilateral lower extremity tasks (ie. lateral step down) to obtain a baseline perspective on the patient’s willingness to move and quality of movement. No major deviations were observed with these movement tasks, so a more complex activity, running, was selected. A running video analysis was conducted, given that this was the primary activity which caused the patient’s pain and for which his participation was limited.
CASSS & Key observations: We used video to record running mechanics on the treadmill in the frontal and sagittal view. Running speed was self-selected by the patient. Using the CASSS framework, for control, we visually observed relatively good trunk and lower extremity control in the sagittal and frontal plane, but cadence was low. Observing amount, we noted excessive vertical displacement in the frontal plane during running. JP demonstrated a self-selected running speed of a 7:45 min/mile running pace. Numerous deviations in symmetry were observed from the frontal plane including increased trunk lean to the right when in mid stance on the right, excessive pelvic drop when in mid stance on the right, and the right lower extremity was in an externally rotated position in stance. (Figure 2) The patient was noted to have a symmetrical rearfoot strike pattern bilaterally from the sagittal plane, but increased right hip flexion in swing. JP reported pain symptoms of 4/10 to the right Achilles tendon during the task.

Hypotheses and Exam: The hypotheses regarding the movement alterations of this patient included: 1) force impairment may be present in the proximal hip/core musculature and right ankle plantar flexors; 2) energy deficit, a possible lack of ankle plantar flexion muscular endurance may contribute to excessive right hip flexion; 3) motor control impairment, the low running cadence rate observed may be contributory to excessive strain on the musculoskeletal system19; 4) motion deficit, hip and ankle ROM could be limited contributing to the excessive external rotation of the right lower extremity in stance. Clinical examination revealed weakness of the right hip abductors (4-/5 right; 5/5 left) and hip extensors (4-/5 right; 5/5 left). In single leg ankle plantar flexion, JP could only complete eight repetitions of a heel raise on the right before not being able to continue, compared to completing 25 repetitions on the left. Achilles tendon pain was also reported during the plantar flexion strength test on the right. His cadence was 152 steps per minute which is lower than what is considered optimal (180 steps per minute),20 and a lower running cadence has been associated with increased vertical load rate,21 which in turn has been associated with lower extremity running related injuries.22,23 Hip ROM and Craig’s test did not reveal any meaningful differences between lower limbs, nor were differences found between left and right ankle ROM, therefore a motion deficit was not considered contributory to this patient case.
JP demonstrated significant tenderness and mild swelling at the mid-portion of the right Achilles tendon. A positive arc sign and Royal London Hospital test were noted on the right. While the pathoanatomic diagnosis of Achilles tendinopathy was confirmed through the clinical examination, the movement analysis findings guided the treatment beyond symptom management.
Targeted intervention: Treatment included core, hip abduction, and hip extension strength training, along with eccentric ankle plantar flexion exercises. The eccentric ankle plantar flexion strengthening is specifically designed to painfully load the Achilles tendon with the knee in an extended and flexed position24 and is supported by strong evidence.25 For the energy and motor control impairments, gait retraining to increase step rate with running were included in the treatment, as transitioning to a higher cadence has been shown to result in lower vertical loading rates during running26 which may benefit this patient.
The prognosis for this patient to achieve his goal of pain free running is good with the treatment plan noted. However, in cases which are not responding to traditional management clinicians may need to consider central sensitization27–29 as an explanation for chronic musculoskeletal pain. Although not specifically outlined in the 4-Element Model, the chronic pain symptoms were addressed directly through pain neuroscience education and via the inclusion of noxious electric stimulation in an attempt to modulate the nervous system through decreasing pain sensitivity.30,31
Case Example 3: Femoroacetabular Impingement Syndrome in a Young Active Adult
A.M. is a 30-year-old female graphic designer who presented with a two-year history of unilateral left hip pain. She reported that she was extremely active and participated in some form of exercise six days a week. Her regular forms of exercise were running, yoga, and high intensity strength training. AM reported her pain had progressively worsened over the last six months when she began training for a marathon. AM reported that she had difficulty walking a mile without hip pain, therefore, sought a consult from a primary care sports medicine physician. Radiographic evaluation of AM’s hip revealed an alpha angle of 75 degrees on the modified Dunn view, and a lateral center edge angle of 32 degrees on the anterior posterior pelvis (AP) view. AM was diagnosed with femoroacetabular impingement syndrome (FAIS) due to cam morphology and was referred to physical therapy.32
Task selection: A single-leg squat has been shown as a useful task to evaluate performance in people with FAIS.33–35 Recently, hip biomechanics and muscle strength were also found to be predictors of impaired performance of a single-leg squat in people with FAIS.36 Since AM desired to return to a high level of activity a single-leg squat task was selected to assess her movement (see link in references for the video).37,38
CASSS & Key observations: Using the CASSS, a visual observation was conducted during a single leg squat with her involved and uninvolved limbs. During the single-leg squat task AM demonstrated good control of the movement in the sagittal plane with both the involved and involved lower extremity. The movement was smooth and coordinated between the segments; however, there was a noticeable reduction in the amount of hip and knee flexion observed between the right and left hip, and slightly more contralateral pelvic drop during the left compared to right single leg squat. The speed of the squat movements between sides were similar. There was a clear asymmetry in the depth of the single leg squat between the left and right sides. She also demonstrated less forward trunk flexion when squatting on the left compared to the right. Symptoms- she reported a level of 3/10 pain when performing a left single-leg squat whereas she reported a 0/10 when performing this task on her right lower extremity.
Hypothesis and Exam: The clinical hypothesis for the movement deviations observed during the single leg squat task included: 1) a hip motion impairment that may be related to the reproduction of symptoms secondary to bony impingement at the hip; 2) knee flexion motion impairment that may be a potentially learned compensation as part of a strategy to limit the overall depth of the squat to avoid moving the hip to near end ranges; 3) motor control impairment as demonstrated by the greater amount of contralateral pelvic drop and hip adduction on the left compared to the right. Additionally, the patient may exhibit 4) force impairments of the hip abductors, extensor, and external rotator muscles that could also limit the ability to achieve equal single-leg squat depth.36,39–41
The physical therapy examination of AM revealed a C-sign pain pattern at the hip described as a deep ache with occasional sharp pain during squatting and pivoting. Range of motion assessment showed reduced hip flexion (left: 90 degrees vs. right: 105 degrees) and hip internal rotation at 90 degrees hip flexion (left: 8 degrees vs. right: 20 degrees) with pain noted at end range for both motions. Knee range of motion was not limited, and symmetrical to the uninvolved side. Hip muscle strength measured with a hand-held dynamometer revealed reduced hip strength of the left compared to right on the order of: 20% for hip flexion strength, 19% for hip external rotation, and 16% for hip abduction. Reduced hip muscle strength is a common clinical finding in patients with FAIS.39,42,43 AM also exhibited a positive anterior impingement sign, and a positive flexion abduction and external rotation test.
Targeted Interventions
The initial physical therapy treatment interventions for this patient focused on reducing symptoms and restoring pain free hip motion. Treatments in this initial phase included soft tissue mobilization techniques, dry needling, and manual joint mobilizations to help reduce pain, muscle guarding, and restore hip range of motion. Closed and open chain strengthening exercises were performed. Specific movement retraining exercises were also performed to help improve biomechanical faults such as greater contralateral pelvic drop during weight bearing function.
The patient completed 16 visits of physical therapy over 12 weeks. However, limited improvement in hip pain and functional activity occurred with PT management. The CASSS framework was used to evaluate the patient’s single-leg squat prior to discharge and there was little to no change in the observed movement deviations during the task. The patient was referred to an orthopedic hip surgeon for further evaluation, which included magnetic resonance imaging (MRI) to evaluate for additional hip soft tissue injury. In addition to confirming cam type morphology, the patient’s MRI also revealed an acetabular labral tear. The patient underwent hip arthroscopy to address the cam morphology and repair the acetabular labral tear.
In the applied case examples, the 4-Element Model was used to evaluate movement during different tasks in patients with three common clinical diagnoses. The tasks used to assess the patients’ movements were selected based on the functional demands of the patient, but also considered the type of injury and phase of healing in order to ensure safe performance of the task. The movement deviations identified were then used to guide the examination and treatment for each patient. These case examples demonstrate that the 4-Element Model can be applied to clinical conditions commonly seen in orthopedic and sports medicine practice.
SUMMARY
The process underpinning the 4-Element Model can be applied by clinicians, students, and residents to a wide variety of patients. The simplicity of the model is intuitive for master clinicians and provides the scaffolding needed for developing independent clinical reasoning in novice clinicians. Using a common framework and language across settings, patient types, and specialty programs will enhance communication between practitioners.
Conflicts of Interest
The authors report no conflicts of interest.