PSYCHOLOGY IN REHABILITATION
Best practice guidelines for musculoskeletal injury rehabilitation include recommendations to address psychological factors.1 A recent return to sport consensus statement has emphasized a biopsychosocial perspective in regards to preparing injured athletes for return to play, in which aspects including satisfaction and confidence in performance are taken into account.2 However, physical therapists’ knowledge of practical application is lacking,3 and athletes still experience negative psychological outcomes upon completing rehabilitation.4 Interventions directly assessing this tend to focus on psychology as something separate and “other,” creating a gap which physical therapists are unable to effectively fill. The important question to ask is, therefore, whether this can be addressed by physical therapists in the clinic?
SIMPLE AND EFFECTIVE PSYCHOLOGICAL SKILLS TRAINING
Injured athletes often refer to lack of fun and desire for more activity-specific rehabilitation,5 and express lower physical activity motivation and sport self-confidence.4 The most appropriate tools to address these are simpler than one might think. Effective goal setting and shared decision-making according to Self-Determination Theory6 can be an easily implemented method of addressing psychological factors. The patient knows their sport and pre-injury skills. Therefore, involving the patient in whether and how they will return, and basing strategies on individual skills and desires, such as sport-specific jumping and cutting, for example, can create a sense of meaning and ‘ownership’ in rehabilitation. Person-centered discussions about strategies can boost motivation and self-confidence by addressing patients’ lack of rehabilitation knowledge and highlight progress in reference to smaller process goals. It also provides a ‘friend’ in rehabilitation, as the physical therapist shows that they care about the individual, and not only the knee.
Communication and goal-setting can emphasize individually meaningful tasks, making it easier to focus externally on real-world connections, such as understanding how an exercise is related to jumping up for a ball. From a psychological standpoint, external focus does not only mean an external stimulus; it should include re-creating situations from an individually-relevant context. Typically, external focus may include watching oneself in a mirror or reaching towards a point on the wall to establish ‘desirable’ movement patterns. However, letting athletes simulate part or all of a sport-specific and meaningful situation may help connect them to their own reality, leading to motivated and natural movement patterns. Physical therapists can and should monitor for safety, but allowing the patient to solve their own puzzles is an effective tool in motor learning. The OPTIMAL theory of motor learning states that self-determined, challenging, and successfully executed meaningful movements can aid in developing more automatic and realistic movement patterns.7
PSYCHOLOGICAL SKILLS TRAINING IN REHABILITATION
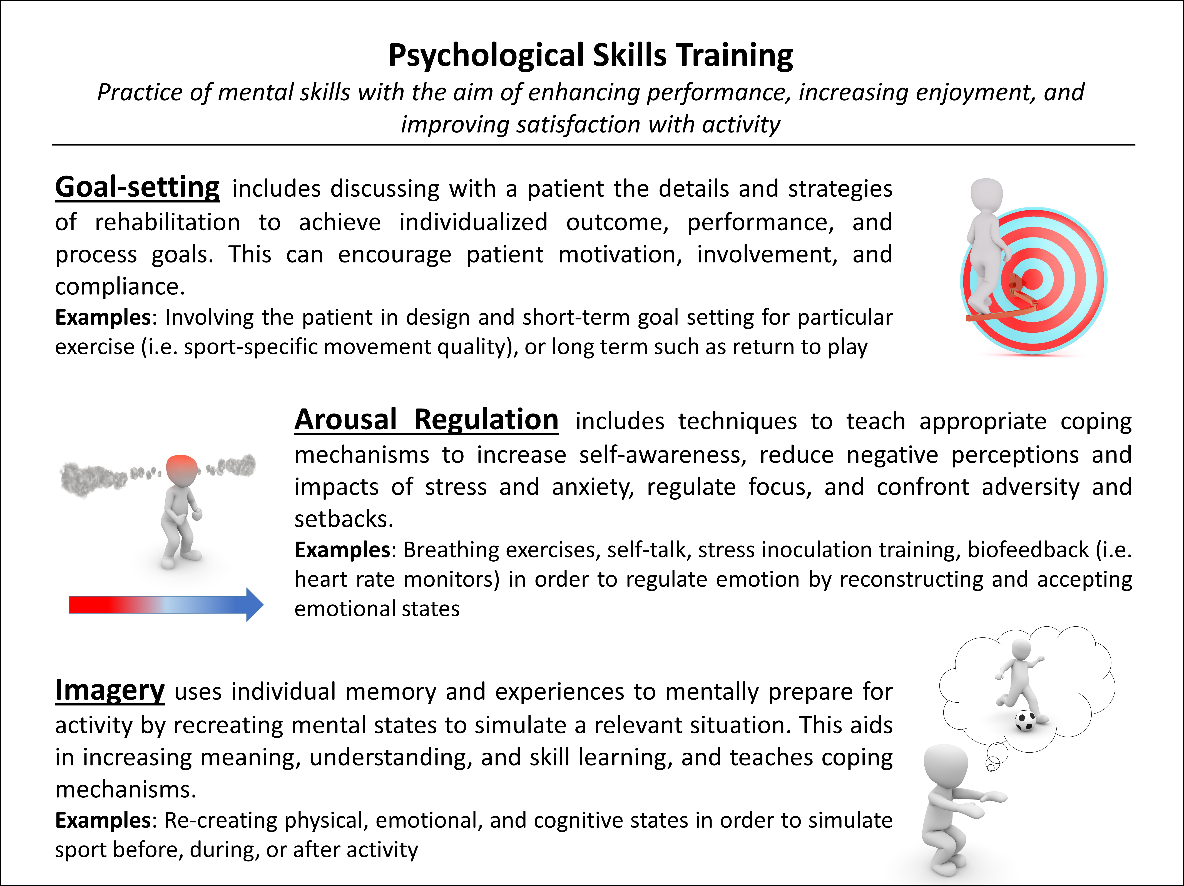
Common Psychological Skills Training interventions include goal-setting, arousal regulation, and imagery (Figure 1). Dynamic motor imagery is done by creating mental images of relevant and meaningful situations based on previous experiences, while simultaneously physically simulating the movement. We have reported that exercises commonly used in rehabilitation training with integrated dynamic motor imagery, known as Motor Imagery to Facilitate Sensorimotor Re-Learning (MOTIFS), may improve enjoyment and feelings of control in uninjured athletes, without sacrificing movement quality.8 It takes longer to implement, but positive psychological reactions may be worth the time investment. The MOTIFS training model is currently being evaluated with knee-injured people.9
Integrating externally focused sport-specific dynamic motor imagery in the clinic is distinctive due to reality- and experience-based re-creation of individually relevant and meaningful situations. This does not simply mean pushing them off balance, reaching towards an external object, or putting a ball in their hands; it means striving for total immersion. Upon receiving instructions, a basketball player may interpret a toe- or shoulder-raise movement as a lay-up, for example. Realism is achieved by imaging sport-specific physical execution, environments (sights, sounds, smells), timing, speed, and relevant emotional experiences. Practically, this includes other players, time left in the game, and where to pass the ball. This translates into realistic physical execution which simulates sport experience. The situation-specific rehabilitation exercise may then be applied by taking an approach step with a basketball in their hands, performing the exercise, and following through with a shot. This training can create self-determined (i.e. based on autonomy, competence, and relatedness), meaningful and enjoyable external focus, and relates directly to patient and physical therapist goals, ensuring physical and psychological relevance to returning to activity.
Application of psychology in rehabilitation has received increasing attention in the literature.2 Physical therapists can implement psychological training using self-reflection and discussion with colleagues by asking questions such as: How involved is the patient in rehabilitation goals and exercise design? Are prescribed exercises in line with patient goals? Is the main goal to rehabilitate the knee, or to prepare for return to sport? How can I implement sport-specific equipment, timing, environment, and/or meaningful obstacles into exercises to increase realism? Awareness and active incorporation of these aspects stimulates psychological training which clinicians can implement in the clinical environment.
