






Introduction
In the last two decades, sport-related concussion (SRC) has received growing attention within the sporting world. High SRC incidence rates have been reported for contact team sports such as rugby, American football and ice hockey, whereas men’s football (soccer) is associated with the lowest concussion incidence.1 Furthermore, higher rates of SRC were found in female football and ice hockey players during competition and training.
Since 2017, the Concussion in Sport Group (CISG) consensus statement has set the benchmark for physicians, athletic trainers, sports physical therapists and other healthcare providers involved in athlete care at any level of sport.2 Sport-related concussion is defined as a subset of mild traumatic brain injury without structural anomalies on conventional neuroimaging. Headache and dizziness are the most common acute symptoms of SRC that usually resolve after 7 to 10 days, although 10% to 15% of symptoms may persist for a longer period. The CISG statement describes 11 “Rs” of clinical SRC management: recognize, remove, re-evaluate, rest, rehabilitation, refer, recover, return to sport, reconsider, residual effects and sequelae, and risk reduction.2 After an initial period of 24 to 48 hours of physical and cognitive rest, a gradual return to sport (RTS) strategy is recommended.
Feddermann-Demont et al.3 recently presented a systematic approach for the initial examination, diagnosis, and management after SRC for high-level football (soccer) players, which includes a detailed RTS program. To date, this procedure is the only example of a sport-specific comprehensive strategy available for team physicians and healthcare personnel to treat SRC athletes.
In elite ice hockey, concussion protocols of the National Hockey League (NHL)4 and International Ice Hockey Federation (IIHF)5 exist and are consistent with the CISG consensus and RTS guidelines. While the CISG-RTS guideline entails generic activity descriptions (Table 1), the NHL protocol provides an example of a graded return to play progression for ice hockey players after SRC.
This clinical commentary presents a detailed RTS program for high-level ice hockey, which is based on the most recent recommendations as well as clinical and practical experience. The proposed comprehensive protocol specifically aims to optimize performance in elite male and female ice hockey players after SRC.
Return to sport
While the team physician (or designee) supervises the RTS protocol,2,3 sports physical therapists, athletic trainers, and conditioning coaches closely cooperate to monitor the injured player throughout the various RTS stages.
Based on CISG guidelines, SRC players are progressively exposed to training activities (known as graduated RTS progression) that do not provoke or worsen symptoms (Table 1). There should be a period of at least 24 hours (or longer) for each progression step. If any symptoms worsen during exercise, the athlete should return to the previous stage.2 The process from one phase to the next should be individualized based on the current signs and symptoms, and on the unique characteristics (i.e. age, experience and skills) of each player.
The 2016 consensus statement on RTS defines three elements of the “RTS continuum”: return to participation, return to sport and return to performance.6 While the ultimate aim of returning to pre-injury performance level is ideally reached after complying with the consensus RTS process, the goal of the supporting staff is to safely and optimally guide the athlete through the “training to perform” regimen. In a recent editorial, Reinhold7 highlighted that sports physical therapy should aim to optimize performance: the key concept (or the “performance spectrum continuum”) not only involves helping the athlete to restore their baseline function(s), but also requires working with them to improve, enhance and optimize performance.
Optimizing return to performance
From a sports physical therapy and athletic trainer perspective, there is a need to be more actively involved in the RTS process rather than passively guiding the athlete.
While it is paramount to closely monitor SRC symptoms (i.e. before/during/after exercising), the inclusion of additional individual-adapted training activities can help the athlete in their “training to perform” at the different stages of the RTS program (Table 2). Table 2 outlines an example of a suitable RTS program for elite ice hockey players with SRC: the athlete should not only progress through the RTS stages, but also work on any deficits linked directly (i.e. balance abilities) and/or indirectly (i.e. reactive capacities) with the SRC.
In Stages 2 and 3 of the recommended program, the player is often supervised by the sports physical therapist or athletic trainer: while the focus is set on aerobic exercise (initially using a stationary bike or elliptical trainer to avoid neck/head impact) and initiating light resistance training, further elements can be added to facilitate player recovery.8–10 In the gym, the player may use skates and a stick for balance and coordination drills, and the slide board for (controlled) agility drills (Figures 1, 2, 3). While the player is still far away from the ice, the additional neuromuscular training—which should be role-specific depending on whether the affected athlete is a player or goalkeeper—enhances sport-specific reactive stabilization strategies and promotes a positive psychological attitude within the overall training regimen.


_(d.jpeg)
If symptoms persist for more than 10 to 14 days, the athlete should be referred to a healthcare professional with concussion management expertise.2,11 In particular, this is the case for players dealing with vestibular and/or oculomotor deficits (the topic of which is beyond the scope of this commentary), who often require comprehensive and targeted management.11–13
Deficient (or insufficient) activation of the deep cervical muscles is a common clinical observation in athletes after SRC,14 and it is therefore recommended to implement a neck stabilization/strengthening scheme in the RTS program usually during Stage 3 when SRC symptoms gradually resolve (Figure 4, 5). Despite the controversy surrounding this aspect of cervical involvement, a stable and stronger neck may contribute to a lower risk of further injury in athletes post-SRC.15–19
_against_a_swiss_ball_(duration_sets_to_be_a.jpeg)

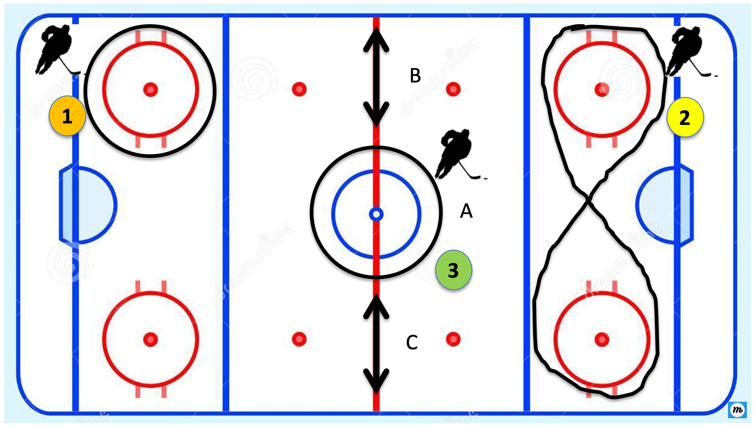
Within Stage 3, SRC players can begin with easy skating (while respecting the sub-symptom threshold) and before engaging in non-contact training (Stage 4.1), a basic set of on-ice drills is recommended (Stage 3.2). The assumption that a symptom-free player in the gym will remain symptom-free on the ice should be avoided; for example, if dizziness caused by head and/or body rotations has resolved with specific vestibular exercises,20 turning and pivoting on the ice may invoke renewed symptoms of head pressure or dizziness. Therefore, by allowing the player to proceed through a set of simple drills, where linear and circular/rotational moves (forward and backward) with simple and dual tasks (i.e. adding puck control, focusing on a fixed/moving target) are performed, the player is then able to feel (and the coaches can observe) whether they are experiencing symptoms during these movements on the ice or not (Figure 6). The ability to master these drills on the ice without symptoms improves the player’s confidence and raises the chances that they will be able to resume non-contact team practice efficiently.
_bully_circle__skating_one_other_directions__20-30_sec_per.png)
Ice hockey is a fast-paced, contact team sport that requires high levels of reaction time and decision making, and athletes after SRC need to master motor and cognitive skills concurrently. Affected players usually experience difficulties with quickness and reactivity drills, which confirms recent findings on impaired reaction times during sports-related movement tasks.21,22 The inclusion of cognitive reactive agility drills with dual or multitasks (e.g. visuomotor reaction time training with the FITLIGHT® system) is therefore an important element in the “training to perform” part of Stage 4 and beyond (both in the gym and on ice).23,24 (Figure 7, 8) In addition to strength and conditioning training, these cognitive reactive agility drills are also necessary to minimize subsequent injury risk.25,26
._t.jpeg)

At Stage 5 of our proposed RTS strategy, the player needs, on average, 4 to 5 full team training practice sessions (including unrestricted contact) before they can be considered completely mentally and physically ready for participation in competition games. As previously mentioned, this process is highly individual and should be based on both the athlete’s response and staff judgement of the athlete’s performance during training. The psychological readiness for competition is crucial, and the use of the Injury-Psychological Readiness to Return to Sport (I-PRSS) tool is helpful to assess the player’s confidence in performing at the last stages of the RTS scheme.27,28 Neurocognitive testing (not discussed here) should also be used as part of the RTS decision-making process.11 Depending on the position, role and importance of the player within the team, the coaching staff often plan a number of games with increasing ice time (usually with the farm team) to allow the progressive return of the player to competition. With appropriate monitoring of the player’s training progression and close interaction with the player, the medical and technical staff can best support the athlete in the “training to perform” stage of the RTS program, which should ideally be a shared decision-making process among these stakeholders.6 Ultimately, RTS after SRC should only occur with medical clearance from a licensed healthcare provider who is trained in the evaluation and management of concussion.13
Conclusion
Sport-related concussion is a severe and complex type of injury requiring specific rehabilitation management and a RTS protocol following the CISG guidelines. While respecting these principles, the supporting team comprising a sports physical therapist and athletic trainer should work with the athlete to restore function as well as optimize and enhance their performance. The athlete is constantly supervised by the medical team during this process. Elite ice hockey players post-SRC should not only be symptom-free and able to participate in unrestricted practice and games, they should also be optimally ready at both physical and mental levels to perform with minimal re-injury risk. This clinical commentary has described a comprehensive RTS ice hockey program, which can help injured elite players in reaching this goal.
Acknowledgements
The author would like to acknowledge Nik Hess (athletic trainer at SCL Tigers, Langnau, Switzerland), Steven Lingenhag (athletic trainer at Hockey Club Davos, Davos, Switzerland) and Gilles Neuenschwander (physical therapist and athletic trainer at Hockey Club Ambrì Piotta, Quinto, Switzerland) for their invaluable cooperation over the years and assistance in the development of this proposed RTS protocol. Melissa Wilhelmi, PhD (medical writer at Schulthess Clinic, Zurich, Switzerland) participated in the copyediting and final proofreading of this manuscript.