INTRODUCTION
Anterior cruciate ligament reconstruction (ACLR) is the primary surgical procedure for restoring anatomic knee stability after an anterior cruciate ligament injury. Despite improvements in ACLR indications, techniques, and postoperative rehabilitation,1–3 a large proportion of patients continue to report long-term reductions in physical function.4 Stronger and more symmetrical quadriceps strength has consistently been associated with better surgical outcomes.5–12 Prior ACLR studies have highlighted a positive correlation between higher quadriceps strength and improved knee function within the surgical limb, as well as a reduced risk of recurrent knee injuries.12–15 In reference to long-term joint health after ACLR, poor postoperative quadriceps function may be an intervening risk factor in the development of post-traumatic osteoarthritis within the knee.16,17
There are a number of considerations for ACLR graft harvest selection with each option having advantages and disadvantages, but research is limited on graft specific objective performance outcomes. Bone-patellar tendon-bone autograft (BPTB) has been reported as the superior graft choice for athletes,18,19 but carries an increased risk of patellar fracture,20 kneeling difficulty,21 and anterior knee pain.19,22–24 Compared to the BPTB, the hamstring tendon (HT) autograft may produce fewer graft harvest site complications,25 but yield an increase prevalence of joint laxity and delayed graft maturation.26–28 More recently, outcomes for the quadriceps tendon (QT) autograft have been reported to be comparable to the BPTB and HT autograft,22,24,29 but the QT produces significantly less initial quadriceps weakness than the BPTB autograft.23 Current evidence suggests no significant difference in graft failure rates between BPTB, HT and QT autografts, 19,24 but studies have suggested graft-specific impairments in muscle function after ACLR, to which the recovery of postoperative quadriceps strength is partially dictated by graft selection itself.30–32 Specifically, ACLR with a BPTB may produce larger reductions in quadriceps function, require more time to recover quadriceps strength, and be slower to achieve rehabilitation milestones compared to the HT autograft or an allograft procedure.33
The above observations are paralleled by research highlighting persistent impairments in quadriceps function at longer-term follow up, independent of graft type.17,34–37 Regardless of graft selection for ACLR, higher postoperative quadriceps strength at mid-term follow-up has been consistently correlated with better knee function at longer-term follow up.38–40 Although greater quadriceps strength may facilitate a better ACLR outcome10,11, the majority of these studies have reported the between-limb, level of quadriceps strength-symmetry as the outcome of interest rather than the actual quadriceps strength relative to the participants’ body weight.41 The quadriceps limb symmetry index (Q-LSI) approach to quantifying muscle strength assumes the non-surgical limb’s strength-value is an adequate benchmark from which to compare the reconstructed knee’s muscles. Most of the recent literature has reported that athletes achieve a Q-LSI anywhere between 73% and 95% at their time of return to activities, which has been measured both isometrically and isokinetically.5,11,13,41–43
However, data published by Chung et al37 has highlighted the fact unilateral ACL injury can produce reductions in muscle strength within the uninjured limb, and suboptimal muscle function is still present at the time of return to sport. For this reason, the use of Q-LSI without consideration of the individual’s relative strength levels when assessing functional status should be questioned. To the authors’ knowledge, two studies to date have investigated the ability of Q-LSI and relative strength values to predict patient-reported knee function.44,45 Kuenze et al44 suggest an isometric relative quadriceps strength value ≥ 3.00 newton-meters/kilogram (Nm/kg) is an acceptable indicator of good patient-reported knee function 2.5 years after ACLR, whereas a Q-LSI ≥ 84.7% is less indicative of higher outcome scores. With similar methods, Pietrosimone et al45 established an isokinetic relative quadriceps strength value of >3.10 Nm/kg as a good indicator of higher patient reported outcome at three years post ACLR.
The potential for inconsistency in quadriceps strength and muscle recovery exists after ACLR, necessitates more detailed reporting of strength outcomes which are specific to the ACLR procedure. Few studies comment on the progression of quadriceps strength relative to the participant’s body weight,46–50 but these studies are limited to only reporting isokinetic data and lack procedure-specific comparisons. Specifically, no study has presented the progression of isometric quadriceps strength within a population of BPTB, HT, and QT autografts at 3, 6, and 9 months after ACLR. Studies with this level of procedure-specific detail can help better define the normal recovery of quadriceps strength after ACLR. Therefore, the purpose of this study was to describe postoperative recovery of quadriceps strength following ACLR related to autograft selection, meniscal status, and sex.
MATERIALS AND METHODS
Between September 2018 and May 2020, 125 competitive and recreational athletes who underwent an ACLR procedure were included in this study; 85% of the participants were involved in either Level I or II cutting, pivoting, jumping, and lateral movement.51 Participants were included if they had undergone ACLR with either a HT, BPTB or QT autograft. Patients who underwent ACLR with a concomitant meniscal repair or meniscectomy were also included. Those with meniscectomies were included in the non-meniscus group for analysis due to lack of weight bearing and range of motion restrictions. Exclusion criteria included those having undergone a contralateral ACLR, a revision ACLR; having a multi-ligament knee injury or graft harvest from the contralateral limb; or any previous knee surgeries on either limb. The study was conducted under institutional review board approval (Advarra, 08.19.2019 NS_HAUS). All testing procedures were explained to each participant and an informed consent document was signed prior to testing. Parental consent and youth assent were obtained for all participants under the age of 18 years. All data was collected at the Training HAUS Sports Science Lab at Twin Cities Orthopedics (Eagan, MN).
All participants underwent quadriceps strength testing between three and nine months after ACLR. Participants completed testing at three separate time points within 1.5 months of their 3, 6 and 9-month postoperative date. For three month testing, no participants were tested earlier than 2.4 months after ACLR. Isometric quadriceps strength tests were all performed using an isokinetic dynamometer (Biodex Medical Systems, Inc., Shirley, NY). Due to the varying postoperative precautions present during the early stages of recovery after an ACLR, isometric contractions at 90-degrees where utilized to test quadriceps strength instead of an isokinetic protocol.20,27,45,52,53
Before testing, participants were taken through a dynamic warm-up led by a physical therapist, athletic trainer or sports performance coach. For strength testing, participants were seated with the knee positioned so that the lateral femoral epicondyle aligned with the dynamometer’s axis of rotation. Thigh, waist, and two chest straps were used to secure the participant to the chair. The dynamometer’s force-arm was secured superior to the lateral malleolus of the ankle. Each participant completed a warm-up protocol on the dynamometer consisting of four, isokinetic knee extensions through a self-selected range of motion. For isometric testing, the knee was positioned at 90-degrees of flexion and all participants were asked to apply as much force as possible against the fixed arm of the dynamometer throughout the duration of the test. One maximal voluntary isometric contraction (MVIC) torque for the quadriceps, recorded in Nm, was completed against the arm of the dynamometer; this was done to practice the subsequent isometric strength test. Three, MVICs were completed for five-seconds in duration, with a 30-second rest interval in between each repetition. For all participants, testing was completed on the non-surgical limb first, followed by testing of the surgical limb. The average of the three peak torque values was calculated (Q-AvgPKT) and normalized to body mass in kilograms (Q-RPKT). Q-LSI was calculated at each time point utilizing Q-AvgPKT with the following equation: (Q-AvgPKT surgical limb/ Q-AvgPKT non-surgical limb) x 100. The variables used in analysis were Q-RPKT and Q-LSI.
An a priori power analysis was completed for three independent groups, a medium effect size and a power of 0.80. For the data set to be adequately powered, a total sample size of 115 patients would be needed with a minimum of 15 patients within each group. Kolmogorov-Smirnov and Shapiro-Wilk tests were used to confirm normality within the collected data set for this study. When applicable, one-way ANOVAs, as well as independent samples t-tests and chi-square tests were used to determine mean differences between the three groups. Statistical analyses were performed with SPSS version 24 (IBM Corp., Armonk, NY, USA), and significance was set at p < 0.05.
RESULTS
Patient demographics are presented in Table 1. Procedure-specific quadriceps strength variables, organized by postoperative time point, are presented in Table 2. The testing protocol used in this study did not result in any surgical complications when implemented as early as three months after ACLR, suggesting an isometric testing protocol on an isokinetic dynamometer is a safe and clinically reasonable way to assess quadriceps strength during the early stages of rehabilitation after ACLR. At postoperative months 3, 6 and 9, quadriceps Q-LSI was found to be significantly higher in patients who had undergone ACLR with the HT autograft than with the BPTB and QT (p< .001). At three months after ACLR, Q-RPKT was found to be significantly higher in those with the HT compared to the QT (p<.05). There were no significant differences in Q-RPKT between graft types at six and nine months after ACLR. At all three postoperative time points, males had significantly greater Q-RPKT than females (p<.01) but no differences in Q-LSI was observed between sexes. Compared to those who received an isolated ACLR procedure, no significant difference in Q-LSI or Q-RPKT was found in those with a concomitant meniscal procedure at the time of ACLR.
DISCUSSION
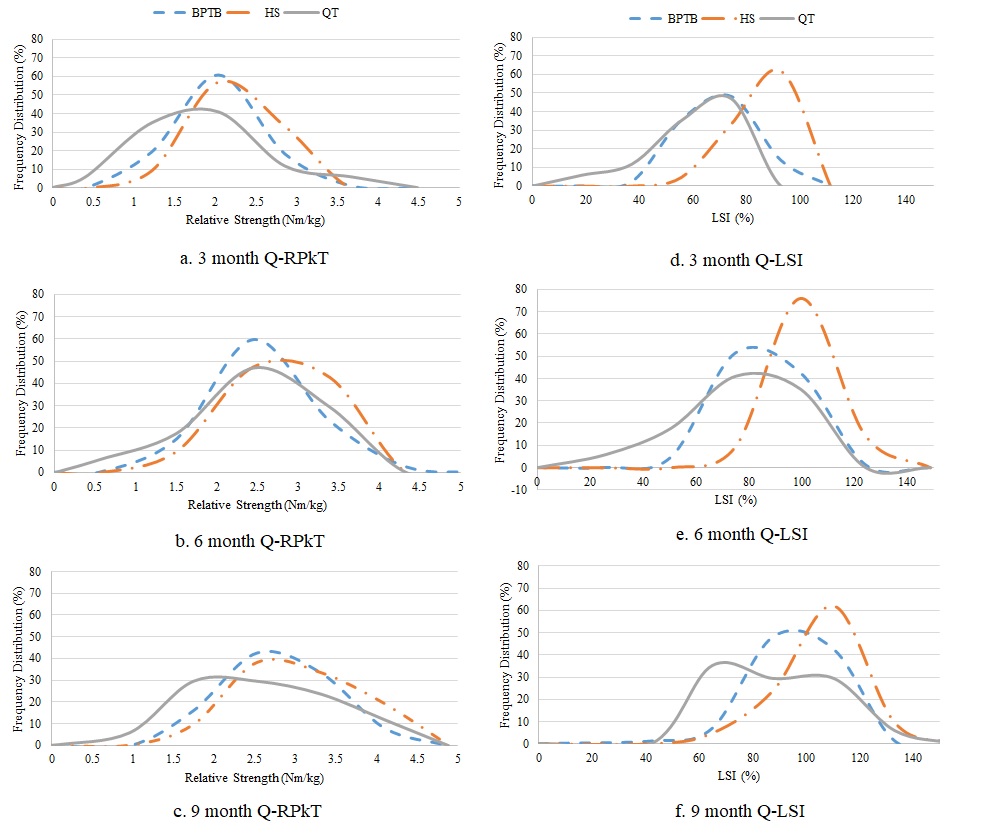
The purpose of this study was to describe the postoperative recovery of quadriceps strength after ACLR. Before determining the clinical significance of any findings, the reader must first acknowledge the observed distribution of quadriceps strength within the cohort. At all three testing points, those receiving the BPTB and QT autografts for ACLR presented with a wider distribution of Q-LSI values than was observed in the HT group (Figure 1. d-f).
Additionally, those receiving the BPTB autograft tended to have a more consistent improvement in Q-LSI throughout the postoperative testing period, which is reflected in the higher absolute BPTB frequency-distribution percentages compared to the QT autograft at the six and nine month testing points. Collectively, these observations suggest that at three months after ACLR, a larger distribution in Q-LSI may be expected in those receiving the BPTB or QT for ACLR, compared to the HT autograft.
This study’s findings also suggest individuals receiving the HT autograft for ACLR may exhibit a greater Q-LSI throughout the postoperative rehabilitation period, compared to those receiving the BPTB and QT autografts. This finding is not a novel contribution to the ACLR literature, as prior studies have reported graft-specific reductions in muscle strength after ACLR. Fischer et al54 reported a difference in muscle strength between the HT and the QT autografts used for ACLR, to which a similarly higher level of Q-LSI was observed in those with the HT compared to the QT. Considering this, this study’s findings further suggest that graft harvest site is a relevant functional consideration for Q-LSI after ACLR, as graft specific impairments in quadriceps symmetry between limbs may be expected with the BPTB and QT autografts, compared to the HT.
At three months after ACLR, this study suggests individuals receiving the HT may expect a statistically greater level of Q-RPKT than those receiving the QT autograft. BPTB Q-RPKT was less than HT and greater than QT, but these differences were not statistically different. These decreased Q-RPKT values in QT and BTB may be present due to graft harvest from the knee extensor mechanics resulting in decreased tendon capacity. At postoperative months six and nine, no between-graft differences in Q-RPKT were found between any of the three autograft types (Table 2). Prior research has suggested any between-graft differences in quadriceps strength may only be clinically distinguishable during the early phases of rehabilitation after ACLR;55 a notion which these findings support. These findings may support the idea that factors other than graft harvest site are responsible for relative strength values not reaching previously reported values for higher outcomes by nine months.44,45 Further research is needed to assess the relevance and relationship of Q-RPKT to the timing of return-to-sport (RTS) and graft rupture rates.
The statistically lower Q-LSI values observed after ACLR with the BPTB and QT, compared to the HT autograft, may be partially explained by the body’s protective response to donor site morbidity. Previously published biomechanical research has highlighted a 25% and 34% relative reduction in the absolute tensile strength of the patellar and quadriceps tendons after autograft harvest, respectively.56 It also appears having a concomitant meniscal procedure at the time of ACLR does not impact Q-RPKT or Q-LSI levels, and although males presented with a greater Q-RPKT than females, sex did not significantly impact Q-LSI levels. Collectively, these findings may suggest the low Q-LSI observed with the BPTB and QT, and Q-RPKT with the QT autograft at three months, is partially due to trauma to the extensor mechanism during graft harvest rather than any additional meniscal procedure at the time of ACLR.

When discussing RTS after ACLR, recent authors have shown that only 65% of athletes return to their pre-injury level of sports participation.57 An improved understanding of the contextual factors associated with RTS has shown a greater subjective report of knee function is positively correlated with an improving likelihood of an athlete returning to their pre-injury level of sport.58 Prior research has highlighted a positive relationship between greater Q-LSI and patient reported knee function, but fewer studies have investigated the relationship between Q-RPKT and subjective knee function. Kuenze et al44 reported an isometric relative strength cut-off value of ≥ 3.00 Nm/kg may be a more sensitive predictor of good patient-reported knee function in recreational athletes than Q-LSI. This however, was collected in recreational individuals beyond traditional time points of returning to sport. The majority of this current study’s population participated in Level I/II sports with 52% of HT, 22% of BPTB and 35% of QT achieving the previously mentioned Q-RPKT ≥ 3.00Nm/kg by the nine month post-surgery time point (Figure 1. a-c). These findings suggest that at nine months after ACLR, a relatively low proportion of this cohort achieved the level of Q-RPKT that may be assumed to present with a high self-report of knee function.
Smith et al33 have previously highlighted a discrepancy between subjective reporting of knee function and objective functional status within a cohort of athletes after ACLR. Athletes who had an ACLR with the BPTB were slower to achieve rehabilitation milestones and functional criteria than those with the HT or allograft, but no statistical, between-graft differences were observed in the subjective reporting of knee function. However, it is important to note that Smith et al33 used Q-LSI, rather than Q-RPKT, to quantify quadriceps function, and therefore, inferences from their study on the relationship between Q-RPKT and subjective knee function within this cohort is not directly comparable.
Q-LSI is commonly used as an objective outcome within the RTS decision-making process. Considering this, HT autografts consistently had more individuals testing ≥ 90% Q-LSI at all three testing points, with less variability in strength testing scores than the BPTB and QT autografts. This finding, alone, may be useful to clinicians when implementing criteria-based rehabilitation for an athlete. For instance, a medical team may elect to more closely monitor the progression of quadriceps strength throughout the postoperative rehabilitation period for athletes undergoing ACLR with the BPTB or QT compared to the HT, as well as implement a longer and more specific quadriceps strengthening program. Lastly, the procedure-specific Q-LSI and Q-RPKT values within this study may be used as normative data for clinicians to cross-reference when implementing criteria-based rehabilitation after ACLR for those returning to Level I and II sports, as well as recreational athletes returning to activity.
Strengths of this study include the standardization of data collection; testing of participants at multiple testing periods; and the direct comparison of quadriceps strength between the HT, BPTB, and QT autografts for ACLR. However, this study has several limitations worth mentioning. (1) This study was a retrospective analysis of prospectively collected data, and therefore, subject to the innate limitations of a retrospective study design. (2) Wide age-range within this cohort may make it difficult to extrapolate the normative data to more specific populations, such as young athletes returning to sport. (3) Participants were recruited from a single metropolitan city, making the possibility of a regional bias reflected within the study’s outcomes. (4) ACLR procedures were completed by 36 different surgeons; specific postoperative rehabilitation protocols, number of therapy visits, quality of rehabilitation, variance in surgical techniques and supplemental training was not standardized or described. (5) Weight bearing status was not taken into account for the meniscus repair group. (6) Lastly, a relatively low number of ACLR procedures with the QT and HT, compared to the BPTB, were completed within this cohort.
CONCLUSION
The results of this study outline isometric quadriceps strength progression specific to graft type, sex and meniscal involvement. Q-LSI was significantly greater in HT compared to BPTB and QT graft types at all three time points. Q-RPKT for QT was significantly lower than HT at 3-months, postoperatively. At all time points, males presented with significantly greater Q-RPKT than females, but sex did not significantly impact Q-LSI. Lastly, receiving a concomitant meniscal procedure at the time of ACLR did not statistically impact Q-RPKT or Q-LSI. The strength data found within this paper can be used to better understand the recovery of quadriceps strength after ACLR, as well as be used to optimize the rehabilitation plan of care based on surgical procedure. Future analysis on this population from subsequent testing sessions at later time points and evaluation of self-reported function will further provide additional insight into isometric quadriceps strength progression following ACLR.
CONFLICTS OF INTEREST
The authors report no conflicts of interest.
ACKNOWLEDGEMENTS
We thank the Twin Cities Orthopedics surgeons and physical therapists who referred their patients to be participants in this study. We also acknowledge Becky Stone McGaver for her contribution to this work.