INTRODUCTION
Anterior cruciate ligament (ACL) injury is common in adolescents and young adults with over 200,000 ACL injuries reported in the United States each year.1 It has been reported that greater than 75% of all young athletes who suffer an ACL tear undergo ACL reconstruction (ACLR).2 Deficits in quadriceps strength and muscle atrophy are common both early in rehabilitation and long-term after ACLR.3 Quadriceps weakness after ACLR has been associated with altered gait,4 altered biomechanics,5 and osteoarthritis.6 Prior reports of return to sport (RTS) rates have been reported to be as low as 33% twelve months after ACLR.7 Even more concerning is the rate of a second ACL injury, reported to be as high as 35% for young athletes.8,9 While these issues are likely multifactorial, one significant reason for these RTS rates and re-injury rates may be the failure to obtain sufficient lower extremity function and muscle strength.10
One of the most common and effective methods for increasing muscle strength and mass is through heavy-load resistance training (HL-RT).11 The American College of Sports Medicine recommends performing resistance exercise at an intensity greater than 70% of maximum strength in healthy adults in order to achieve muscle adaptations in both size and strength.12 In the first 12 weeks after ACLR, the use of HL-RT is not feasible, as high levels of musculoskeletal loading may be contraindicated in post-surgical individuals. Low load resistance training (LL-RT) is often indicated during early stages of rehabilitation, but is often insufficient to invoke adequate muscular adaptations. There is mounting evidence that performing LL-RT with blood flow restriction to the exercising muscles provides a potent stimulus for increasing muscle strength and mass after ACLR in adults.13,14
Blood flow restriction training (BFRT) is a technique increasingly used in physical therapy and rehabilitation settings as an alternative to HL-RT. BFRT consist of exercising using a surgical grade pneumatic cuff or tourniquet that partially restricts arterial inflow, and fully restricts venous outflow from the working musculature during exercise.15,16 The clinical value of BFRT that has been suggested in the literature is that it allows increased muscle adaptation and hypertrophy with LL-RT,17 making BFRT a potentially advantageous tool to implement in the early post-operative population. The utilization of BFRT in conjunction with current rehabilitation standards of care has shown potential with respect to muscle adaptations and performance. A meta-analysis comparing BFRT on musculoskeletal rehabilitation versus traditional LL-RT, reported low load BFRT training to be more effective in helping patients regain strength than traditional LL-RT.17
A common point of discussion regarding BFRT is the potential safety risk, specifically in the post-surgical population. Possible concerns include the effects of BFRT on the cardiovascular system such as blood pressure responses, potential thrombolytic events and damage to the vascular system.16 Despite these concerns, there have been several extensive reviews published demonstrating that the side effects are minimal,18,19 and BFRT when compared with traditional methods of strength training shows no greater risk in adults.20 Hughes et al. described BFRT to be as effective at improving strength and more effective at improving function, pain, and swelling compared to HL-RT in ACLR patients,13 as well as more comfortable for patients during the early phases of post-surgery rehabilitation.21 The ability to improve strength and function with BFRT with mild patient discomfort makes for an appealing tool during the early post-surgical phases of rehabilitation.
While the effectiveness and safety of BFRT has been explored in the healthy adult population, there is limited information about the tolerance and side effects of BFRT in the adolescent population post ACLR. Given that a large proportion of ACLR occur in the adolescent population and also recognizing that young22 and active patients are the most at risk for re-injury, BFRT has significant potential to aid in rehabilitation of these individuals after ACLR. Therefore, the purpose of this study was to investigate and record patient reported/observed side effects and tolerance to BFRT during post-surgical ACL rehabilitation in adolescents. It was hypothesized that adverse events and patient tolerance to BFRT will be consistent with previously published literature.
MATERIALS AND METHODS
Ethical Approval
Ethical approval was granted from an Institutional Review Board.
Study Design
Prospective Cohort Study
Consent
All potential patients that were scheduled to undergo ACL reconstruction at Connecticut Children’s were approached for participation for the study. Patients were pre-screened based on inclusion and exclusion criteria. Once identified as a potential candidate, the study purpose and protocol were explained and a brief summary of the study was provided to the patient/parent. Once patient/parent agreed to participate in the study, all patient guardians and patients provided signed informed consent/assent at the pre-operative visit.
Participants
Participants in this study were those between 12 and 18 years of age already enrolled in an ongoing IRB approved registered clinical trial investigating the impact of BFRT after primary ACLR at Connecticut Children’s from January 2020 to present. All study participants underwent ACL reconstruction using quadriceps tendon autograft by two sports fellowship trained orthopedic surgeons. All participants had no known history of central or peripheral neurological impairment and were free of any cardiac, pulmonary or metabolic conditions. Other exclusion criteria included: previous surgical intervention either on the ipsilateral or contralateral knee, history of deep vein thrombosis, multi-ligament rupture or trauma, chondral pathology and any additional lower extremity injury at time of knee injury requiring treatment. Additionally, meniscal root and complex tears requiring weight bearing restrictions greater than two weeks after surgery were also excluded.
Postoperative Rehabilitation
All patients initiated formal physical therapy within one week of surgery. All participants were instructed in a standardized postoperative rehabilitation protocol adapted from Adams et al.23 The early rehabilitation phase (up to 12 weeks from surgery) consisted of acute symptom management, restoring range of motion and normalizing gait. In addition to the rehabilitation protocol, all patients followed a standardized BFRT exercise protocol over the 12-week early rehabilitation phases (Table 1). This included three exercises per session as part of their physical therapy session twice per week.
Blood Flow Restriction
All patients utilized a personalized tourniquet system (Delfi Medical), which has been shown to calculate limb occlusion pressure (LOP) reliably and accurately. LOP is defined as the minimum pressure required for full arterial occlusion.24 This device automatically increases cuff pressure in stepwise increments by analyzing arterial pressure pulsations at each cuff pressure increment, and then uses these values to determine LOP. Variable contour cuffs,25 either 24 or 34 inches in length and 4.5" wide, were utilized based on thigh circumference with a protective barrier between the skin and cuff.26 Prior to exercise, the cuff was placed on the most proximal portion of the involved lower limb. Measurement of LOP can help minimize tourniquet pressures and pressure gradients.25 LOP was calculated for each limb individually in the supine position at the beginning of every training session and BFR pressure was set at 80% of the patient’s LOP for exercise completion. LOP at 80% provides high levels of fast twitch fiber recruitment and maximize muscle adaptation.27 Patients were provided instruction that they were allowed to request reduction of LOP during exercise based on their tolerance.
Exercise Progression and Patient Tolerance
To determine the appropriate resistance for each exercise, patients performed the exercise with a weight they could comfortably lift for several repetitions. The patient’s perceived exertion of a one rep maximum (RM) was estimated using the modified OMNI-RES scale and starting load for each exercise was 20-30% of their 1RM.28 Bodyweight resistance was used when loading was not feasible. The standard repetition scheme used in this study was a set of 30 repetitions followed by a 30 second rest followed by three more sets of 15 with 30 second rests in between.29 Patients had eight minutes to complete the target of 75 repetitions for each of the three exercises per session. The BFRT cuff remained inflated for the entire time until all 75 repetitions were completed, or until the eight minutes elapsed. At the conclusion of each exercise, the cuff was deflated for one minute, and the patient’s rating of perceived exertion (RPE) was recorded prior to initiating the next exercise. Patients were instructed to report any side effects or adverse events during or immediately after exercise completion. For the purposes of this study, monitoring for the following side effects included: subcutaneous hemorrhage (SubQ), deep vein thrombosis (DVT), fainting, dizziness, lower extremity paresthesia, and itching as previously described by Yasuda et al.17 To monitor and record patient tolerance, it was documented if patients requested a reduction of LOP or were unable to finish the exercise. The inability to finish an exercise was defined as voluntary stoppage of exercise by the patient, or the inability to complete all 75 repetitions in eight minutes.
Analysis
Results were analyzed using Microsoft Excel. Descriptive statistics were used to calculate the means and standard deviations for height, weight, BMI, age, and average number of BFRT sessions per patient. Adverse event occurrences were tallied for weeks one to four, five to eight, nine to twelve, and cumulatively over the 12-week period. Percentage of occurrences were found by dividing total number of reported occurrences by total number of BFRT sessions. Because of the descriptive nature of this research, no other comparisons were made.
RESULTS
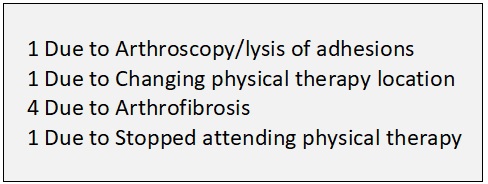
Twenty-nine patients between the ages of 12 and 18 years (15.39±1.62 years of age) at the time of surgery were included in the study. Seven participants were unable to complete the intended 12 weeks of BFRT for various reasons after surgery (Figure 1).

Additional demographic information can be found in Table 2. Five hundred and thirty-five total BFRT sessions were completed between all patients, with each patient completing an average of 18.45±6.47 sessions over 12 weeks. There were zero reports of deep vein thrombosis (DVT), subcutaneous hemorrhage (SubQ hemorrhage), and fainting across all patients (Table 3), considered as major adverse events. Reported minor side effects to BFRT included itchiness of the occluded limb (7.85%), lower extremity paresthesia (2.81%), and dizziness (0.75%) (Table 4). 10.47% of BFR treatment sessions were unable to be finished due to tolerance, and 3.55% of sessions required a reduction in LOP (Table 5).
DISCUSSION
In this study, out of 535 sessions of BFRT, there were no reported major adverse events (DVT, SubQ hemorrhage, and fainting), and minor reported side effects to BFRT were reported a total of 11.41% of the time. BFRT in adolescents appears to be well tolerated, as patients were able to finish the prescribed exercise 89.53% of the time and reduction of limb occlusion pressure occurred 3.55% of the time.
BFRT pressure, duration of inflation, and cuff width are three modifiable variables that may influence the likelihood of reported adverse events with BFRT. Variable contour cuffs that are 4.5 inches in width with a protective barrier between the skin and cuff were used for each patient. Due to the tapered shape of limbs, variable-contour cuffs have been shown to enhance patient comfort and further decrease the risk of mechanical shearing, as well as allow for occlusion at lower pressures.20 Prior authors have reported on adverse events after BFRT with the use of narrow diameter cuffs (∼3 cm) and with high pressures (160 to 200 mm Hg).16 A higher rate of adverse side effects were reported utilizing a narrow diameter cuff and high pressures, consistent with Estebe et al. who concluded that a 14 cm cuff needed significantly less pressure to occlude blood flow compared to a 7 cm cuff that caused significantly more pain after reaching arterial occlusion.30
Additionally, LOP was calculated for each limb individually at every training session. The personalized tourniquet pressure for each patient plays a role in patient comfort. Lower pressures are needed to stop venous outflow, compared to the amount of pressure needed to stop arterial inflow. If the occlusion pressure is too high, blood supply to the exercising limb can be eliminated. If the pressure is too low, there may be too much arterial inflow causing venous congestion in the limb, which can be very painful for patients.20 While a small percentage reported the need to reduce LOP, the majority of patients in this study tolerated 80% LOP. There is some evidence to suggest that lower occlusion pressures may produce similar adaptations31, but 80% LOP appears to be the optimal pressure to induce the greatest muscular adaptation.27,32
In this study, there were no reports of major adverse events of DVT or subcutaneous hemorrhage. The perception that short duration tourniquet use poses significant thrombus risk appears to be unsupported. While there is risk of DVT after post-operative orthopedic extremity surgery, there is evidence to suggest that the use of a tourniquet is not an independent risk factor for DVT and is correlated with anti-thrombolytic factors in the surgical population.33 It has been well established that short duration tourniquet use has fibrinolytic potential, and does not seem to pose an increased thrombus risk. Additionally, several studies have found no increase in markers for thrombus formation after BFR with exercise.34,35 Survey studies have also reported very low or no occurrences of thrombolytic complications (0.055%),18,36 and Nakajima et al reported that 13% of adults experienced subQ hemorrhage which is in contrast to the current findings. These reports of occurrences were often in an adult population, as well as without the use of standardized limb occlusion pressure, or variable contour cuffs.
In 7.85% of sessions, patients in this study reported transient itching, but it is important to note that all patients were able to complete exercises. Of the 29 patients in the study, two patients accounted for all reported events of itchiness. Prior research regarding patient tolerance to BFRT has not reported on the sensation of itching. The pathophysiology of itch is not well understood, but it has been categorized into four clinical categories: psychogenic, neurogenic, neuropathic, and pruritoceptive.37 It is unknown if itch after BFR follows the same physiology. There is also some evidence to suggest that itch after BFRT is related to the histamine release that occurs during exercise.38 Exercise will result in the activation of histamine receptors in the exercised muscle and triggers vasodilation, as well as a broad range of responses to exercise.
Previous reports of other adverse events such as fainting/dizziness, and lower extremity paresthesias after BFRT have varied. In this study, there were no reports of fainting, and very low occurrences of paresthesias. Tourniquet compression may cause paresthesias due to ischemia or altered nerve conduction, however all reports of paresthesias in this study were transient and normal sensation was restored immediately following cuff deflation. Patterson et al reported fainting and dizziness in 14.6% of subjects, however, this included a wide range of ages, several different types of tourniquets or hand held pumps, and non-standardized occlusion pressures.36 Careful monitoring and feedback from patients, as well as subtle adjustments of tourniquet placement on the proximal limb may help minimize these side effects. It is possible that as this study continues and the number of enrollees grows, fainting may be encountered. Based on the findings in this preliminary report, it appears this will be an infrequent occurrence and will likely not be a contraindication to BFRT for adolescents after ACLR
LIMITATIONS
The relatively small sample size of only 29 participants is the principal limitation in this study, and this report should only be interpreted as a preliminary report. Further, while patients between the ages of 12 and 18 were recruited for this study, most patients were on the upper end of this age scale so the younger adolescent population was not equally represented. This is expected in the ACLR population as most of these injuries occur after the onset of puberty, but it represents a limitation nonetheless. Additionally, by defining “inability to finish” as voluntary stoppage of exercise by the patient or the inability to complete all 75 repetitions in eight minutes, patient intolerance may have been overestimated. Load progressions in this study were based on the patient’s ability to successfully complete 75 repetitions. Therefore, it is unknown whether the inability to finish was a result of adequate loading or voluntary stoppage because of intolerance. Future studies will better define these differences. Lastly, because of the focus on immediate side effects/responses to BFRT, there may have been a failure to capture long term side effects like delayed onset muscle soreness (DOMS).
CONCLUSION
This preliminary report shows a very low and minor side effect profile as well as generally good tolerance to BFRT in the adolescent population after ACLR. Major reported side effects to BFRT such as a DVT, SubQ hemorrhage, and fainting were not seen in this study, and minor side effects of BFRT including paresthesias and itching of the occluded limb were infrequent. As always, all populations should be assessed for possible risks and contraindications before performing BFRT. Further data is needed for a definitive determination of the safety of this intervention in this population, however, the early results are promising.
Conflicts of Interest
JP, DR, NG, AL and AW have no conflicts of interest to disclose. AC has a leadership role for Pro Papa Missions America, Pediatric Orthopedic Society of North America, and Pediatric Research in Sports Medicine. JLP receives consulting fees and grants from Arthrex, JRF Ortho, and the American Orthopedic Society for Sports Medicine.