INTRODUCTION
Female athletes have a higher incidence of anterior cruciate ligament (ACL) injury in both high school and collegiate levels of sports participation.1 This injury incidence is increasing at a faster rate when compared to males.2 ACL reconstruction (ACLR) is often the treatment of choice following ACL injury, and short-term goals following ACLR include return to sport and improved self-reported function.3 Females have significantly worse outcomes for both of these short-term goals: they are less likely to return to competitive sport,4 and they report significantly worse knee-related function5 compared to males. Thus, it is important to understand possible factors that may influence the inferior outcomes observed in female athletes following ACLR.
A safe return to sport following ACLR is defined as the ability to return to sport without sustaining a secondary ACL injury, whether to the ACL graft or the contralateral ACL. Secondary ACLR results in a significantly lower rate of return to sport and inferior functional outcomes compared to primary ACLR,6–10 which has implications for short- and long-term knee-related quality of life. Approximately 20-25% of young athletes who return to sport after ACLR have a second ACL injury,11,12 and females after ACLR are approximately five times more likely to sustain an ACL injury compared to females without a history of ACL injury.13 Furthermore, female gender, young age, and return to high activity level all increase the odds of sustaining a second ACL injury.14 Due to the elevated injury incidence, inferior functional outcomes, and high rate of secondary ACL injury, female athletes after ACL injury represent a significant public health challenge. Efforts should be focused on understanding possible modifiable factors associated with the elevated risk of secondary injury and inferior functional outcomes observed in young female athletes who return to a high level of sport, such a Division I collegiate athletics, after ACLR.
Double limb jump-landing tasks have been utilized previously both as a screening tool for ACL injury risk15 as well as a portion of a return to sport test battery following ACLR.16 During the landing phase of the task, which is often defined as the period from initial contact to maximum flexion, there are altered lower extremity biomechanics after ACLR in both limbs.17 Additionally, between limb asymmetries are more often observed following ACLR in kinetic as opposed to kinematic variables during this task, including a decrease in the peak vertical ground reaction force (vGRF) of the involved limb.18,19 The Landing Error Scoring System (LESS) is a valid and reliable composite measure of kinematics during this jump-landing-rebound task20,21 that can be combined with the Kinect camera for automated scoring.22 The LESS identifies high-risk movement patterns (“errors”) at both initial contact and maximum flexion, and generates a cumulative score of errors, whereby a higher score (number of errors) is indicative of poorer movement quality. Prior research has shown that individuals previously cleared to return to recreational sports after ACLR have worse composite scores compared to matched control subjects.23,24 However, these recreational athletes may not have the same kinematic profile of female athletes participating at a higher level of competition after ACLR.
Given that ACL injuries occur within the first 50 milliseconds after ground contact,25,26 the analysis of the landing phase temporally aligns with the occurrence of these injuries. Additional insight may be gained from examining the propulsion phase, which occurs as the athlete generates higher vGRF to propel their body into the air following maximum flexion. Analyzing the propulsion phase of this vertical jump may be of interest given that the knee performs a higher percentage of the work relative to the other lower extremity joints when compared to a horizontal jump,27 making this task functionally relevant to athletes who may have deficits in knee function after ACLR.
In summary, prior research has demonstrated that following ACLR, individuals report lower function and demonstrate both kinetic asymmetry and poorer movement quality during landing tasks. However, prior research has not specifically investigated elite female athletes who have returned to sport. Given the high risk of future ACL injury within this cohort, a better understanding of those athletes who safely return to elite sport without subsequent injury, particularly in the context of their teammates, may provide insights into return to sport testing criteria and secondary injury prevention efforts.
Therefore, the purpose of this study was to compare elite collegiate female athletes who were able to successfully return to sport for at least one season following ACLR to their teammates with no history of ACLR with regard to self-reported knee function, kinetics and kinematics during a double limb jump-landing task. It was hypothesized that in comparison to their teammates, athletes post-ACLR would report worse knee-related function, demonstrate decreased peak vGRF on their involved limb during landing and propulsion, and have a higher composite LESS score, indicative of poorer movement quality.
METHODS
Participants
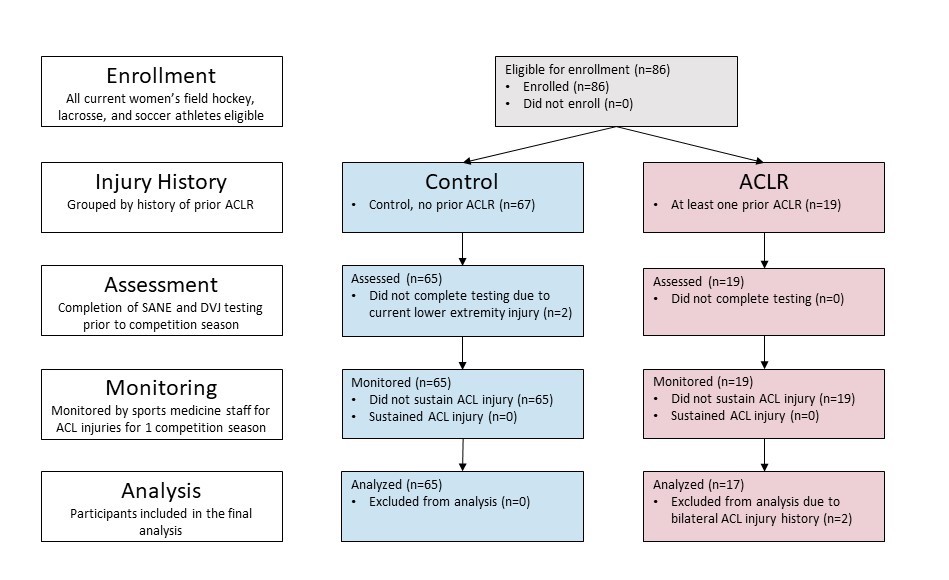
All members (n=86) of the women’s field hockey, lacrosse, and soccer varsity teams at one Division I university were eligible for enrollment and were recruited to participate prior to their competitive athletic season during an academic year. These sports were selected as they represent the women’s field sports at this university. Additionally, all three teams have won at least one national championship in the decade prior to study enrollment, suggesting these teams represent elite collegiate athletes. Athletes were classified according to self-reported injury history: ACLR (at least one prior ACLR reported, n=19), and control (no prior ACLR reported, n=67). Any athlete who had a current lower extremity injury that limited their ability to perform a jump-landing task was excused from the movement assessment described below. Following assessment, all athletes were monitored by the sports medicine staff for ACL injury for one competitive season. A successful return to sport for at least one season was operationally defined as participation in the index sport without a secondary ACL injury during a six-month monitoring period, which coincided with the competitive season, following baseline data collection. A flow diagram of participants is depicted in Figure 1. The university’s Institutional Review Board approved the study, and written informed consent was obtained from all participants.

Procedures
Demographic and anthropometric information were collected, including age, height, and weight. Participants were given a detailed knee injury history questionnaire. They were asked to report if and when they sustained any ACL injuries, including the limb that was involved and any concomitant injuries. They were asked to report the year they underwent ACLR. They also reported a knee-specific single assessment numeric evaluation (SANE), rated based on the statement: “On a scale of 0-100, how would you rate your involved knee today, with 100 being normal?” The knee-specific SANE is positively correlated with the International Knee Documentation Committee (IKDC) subjective knee survey in individuals following ACLR28 and was selected in this study due to its time-efficiency.
All participants completed three trials of a double-limb jump-landing movement assessment as previously described.20,22 For the assessment, participants jumped from a 30 cm tall box to side-by-side force plates in front of the box, the center of which was 90 cm from the front edge of the box. They were instructed to complete a maximal vertical jump immediately after landing. A trial was deemed successful if the participant (1) jumped off the box with both feet leaving the box at the same time; (2) jumped forward, not vertically, to reach the force plates; (3) landed with one foot on each force plate; (4) jumped vertically, and not forward, during the maximal jump; and (5) completed the trials in a fluid motion.
Jump-landing trials were recorded by the Kinect camera located 335 cm in front of the front edge of the box (Kinect sensor, version 2, Microsoft Corp, Redmond, WA). The depth-sensing camera was controlled by a standard laptop computer. Concurrently, ground reaction forces were collected at a sampling rate of 1000 Hz from two embedded force plates (FP406020, Bertec Corp), collected through Nexus software (Vicon, Nexus, Oxford, UK).
Data Reduction
In the ACLR group, 17 participants reported one or more prior ACL injuries on one limb only, and the involved limb was defined as the previously injured limb. Two participants in the ACLR group reported ACL injuries on both limbs, and these participants were excluded from analysis given that both limbs were involved. In the control group, the involved limb was randomly assigned as right or left for comparison to the ACLR group as healthy females do not have differences in peak vGRF between limbs based on limb dominance.29
Athletic Movement Assessment software (PhysiMax Technologies Ltd, Tel Aviv, Israel) was used to evaluate the Kinect camera data to score the LESS. This method of automated scoring has been validated against expert raters.22 The LESS was scored based on the scoring criteria described by Mauntel,22 evaluating the frames of initial contact and maximum knee flexion for common kinematic “errors,” such as asymmetry. Scores were averaged across the three trials for each participant. Higher scores indicated more errors, with a minimum score of 0 errors and a maximum score of 24 errors.
A custom MATLAB (MATLAB version R2019a, The MathWorks Inc, Natick, MA) script was used to extract kinetic variables of interest from the ground reaction force data during the ground contact separately for each limb on each trial. Ground contact was defined as the period during which the vertical component of the ground reaction force (vGRF) exceeded 20 Newtons (N).30,31 Two phases of ground contact were defined: impact phase and propulsion phase. The impact phase was the first 200 milliseconds (ms) of ground contact for each limb. The time frame of the impact phase was selected as it captured all peak vGRF values. The impact phase likely represents a subset of the landing phase, as there was not kinematic data available to indicate when maximum flexion occurred. The propulsion phase was the second half of ground contact. The peak vGRF values during the impact and propulsion phases were extracted for each limb during each trial. vGRF data were normalized to body weight (BW) in N for each subject and reported in multiples of BW. The limb symmetry index (LSI) for each variable was calculated as: (involved limb / uninvolved limb) x 100. Values were averaged across three trials for each participant for each limb (involved and uninvolved).
Statistical Analysis
An alpha level was set a priori at α ≤ 0.05. Independent samples t-tests were used to assess differences in knee SANE and LESS composite scores between groups (ACLR vs. control). In addition, Cohen d effect sizes and associated 95% confidence interval were calculated.32 Effect size estimates were classified as small (0.2), moderate (0.5), and large (0.8).32 Separate two-way mixed model analyses of variance (ANOVA) with group (ACLR vs. control) as the between-subjects factor and limb (involved vs. uninvolved) as the within-subjects factor were conducted to determine differences in kinetic variables (peak vGRF during the impact and propulsion phases). If findings were significant, four planned pairwise comparisons (between group and limb) were conducted with a Bonferroni-corrected α level of 0.0125. If parametric assumptions were not met, the Wilcoxon signed-rank test was used for within group comparisons and Mann-Whitney U test was used for between group comparisons. All statistical analyses were performed in jamovi (version 1.6.1.0, The jamovi project).
RESULTS
Descriptive Data
The final analyses included 17 athletes in the ACLR group and 65 athletes in the control group. Participant descriptive data are presented in Table 1. All participants in the ACLR group were at least one-year post-ACLR. The mean time from ACLR to testing was 2.4 ± 1.3 years. Participants in the ACLR group were significantly older and taller than the control group. There were no significant differences in body mass between groups (p>0.05).
SANE and LESS
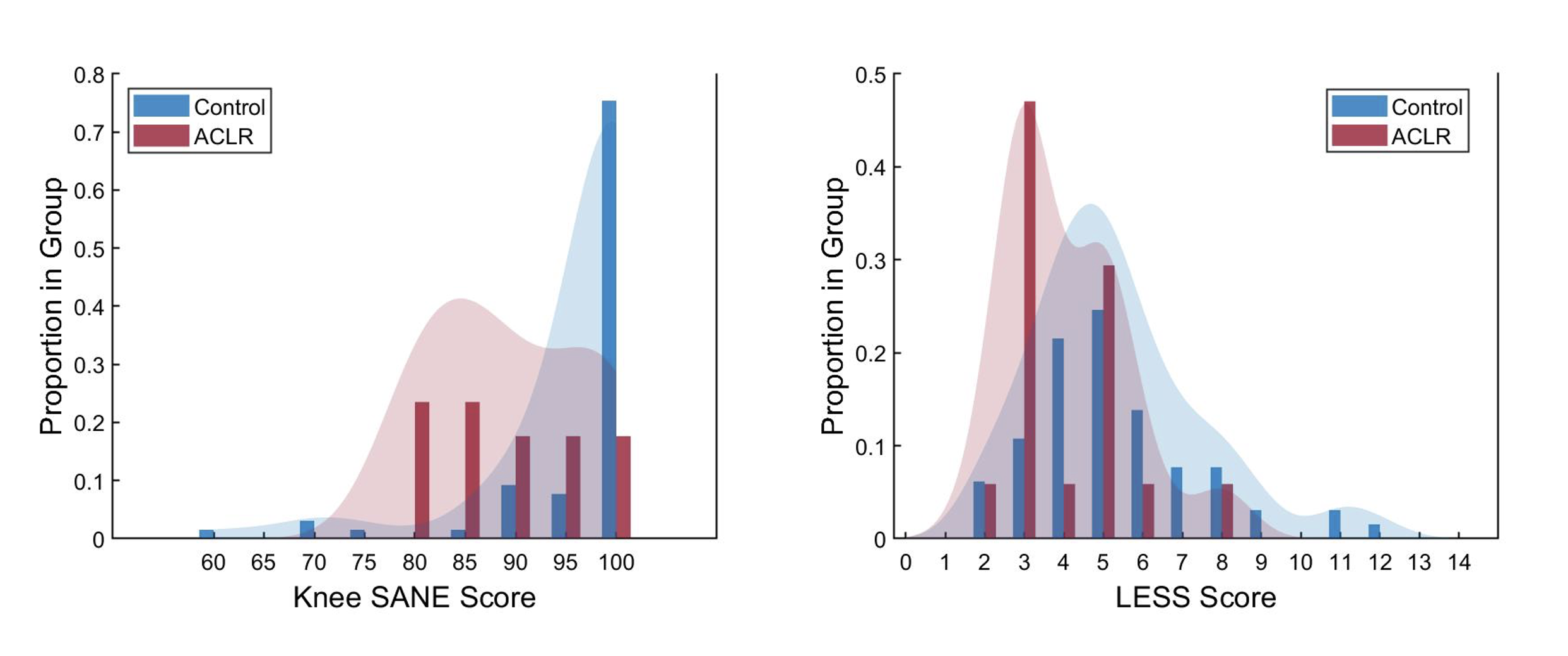
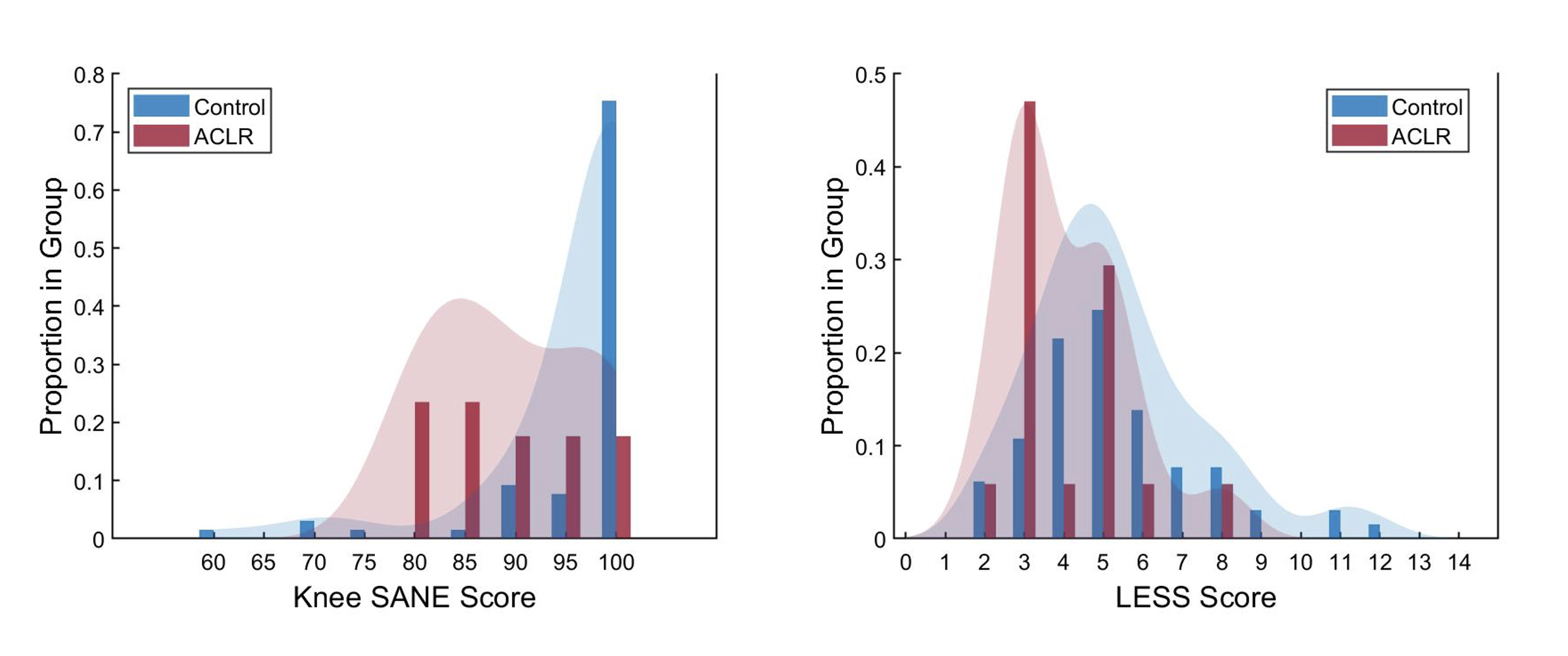
The knee SANE score was significantly lower in the ACLR group compared to the control group (p=0.002), suggestive of worse self-reported function in the ACLR group, as displayed in Figure 2a. The LESS score was significantly lower in the ACLR group compared to the control group (p=0.026), indicating the ACLR group demonstrated better movement quality compared to the control group, as displayed in Figure 2b. Knee SANE and LESS summary statistics are displayed in Table 2.
vGRF-Impact Phase
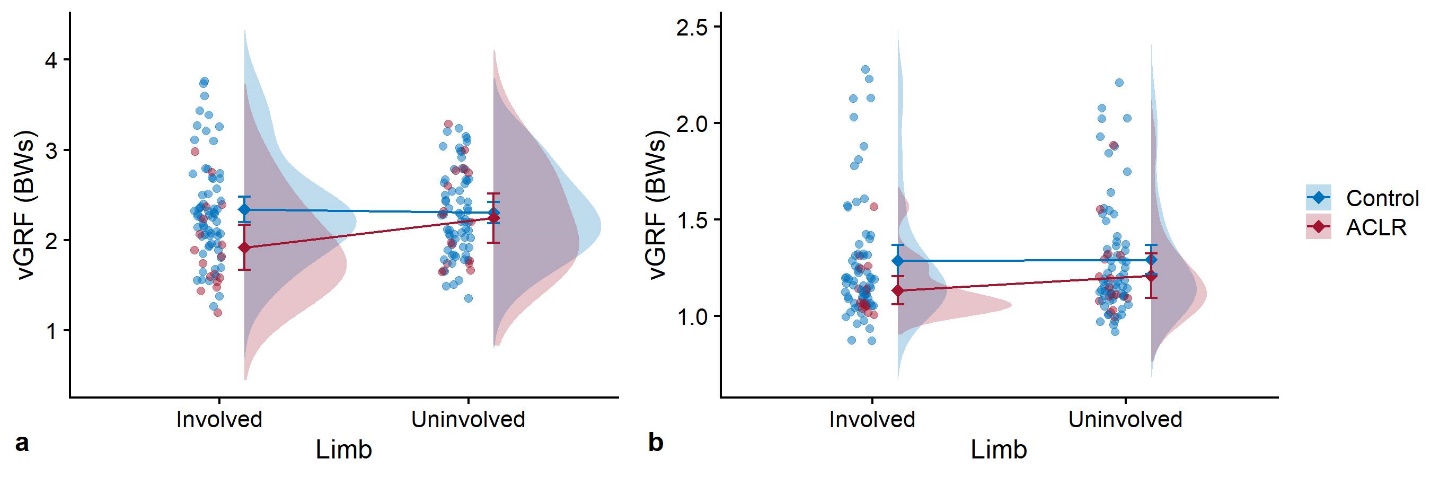
Individual participant means and distribution by group for the impact phase and propulsion phase are displayed in raincloud plots33 in Figure 3. During the impact phase, there was a significant interaction effect (F(1,80)=6.37, p=0.013) and a significant main effect for limb (p=0.048), but no significant main effect for injury history (p=0.51). Based on planned pairwise comparisons, the ACLR involved limb (1.92 ± 0.49 BW) differed from the control involved limb (2.34 ± 0.57 BW), p=0.003, indicative of underloading in the ACLR group compared to the control group. No other significant differences were observed (p>0.05). Group means and standard deviations are reported in Table 3.
vGRF-Propulsion Phase
Levene’s test was significant for the involved limb (p=0.015), suggesting a violation of the assumption of equal variance. Four non-parametric pairwise comparisons were conducted, utilizing Wilcoxon signed-rank test for within group comparisons (Limb: involved, uninvolved) and Mann-Whitney U test for between group comparisons (Group: ACLR, control). All p-values were adjusted using Bonferroni correction based on four planned comparisons. The ACLR involved limb differed from the ACLR uninvolved limb (p=0.012), indicative of asymmetrical loading in the ACLR group. No other significant differences were observed (p>0.05). Group medians and interquartile ranges (IQRs) are reported in Table 3.

DISCUSSION
The purpose of this study was to describe the functional profile of elite collegiate female athletes who were able to successfully return to play for at least one season following ACLR compared to their teammates with no history of ACLR with regard to self-reported knee function, kinetics, and kinematics. Findings suggest that relative to their teammates, elite female athletes averaging 2.4 years after ACLR report worse knee-related function and demonstrate kinetic differences during a jump landing task, including underloading of their involved limb during the impact phase and asymmetrical loading during the propulsion phase. Despite these findings, athletes after ACLR also have lower risk kinematic movement patterns during the same landing task. Additionally, no athletes sustained an ACL injury during the competition season following assessment, suggesting that the functional profile observed was safe for short-term return to participation.
Self-reported knee function
To assess self-reported knee function, this study used the knee-specific SANE, as it is recommended for use due to simplicity of application and direct patient relevance.3 The knee-specific SANE has moderate to strong correlations with the IKDC in populations including young, active females with knee and ACL injuries,28,34,35 and thus provides a reasonable, time-efficient alternative. In support of this study’s hypothesis, there was decreased self-reported knee function in elite collegiate female athletes after ACLR compared to their teammates. Prior research has shown self-reported knee function is worse in females compared to males following ACLR,5 and that higher self-reported knee function is associated with passing return to sport batteries.4
The findings of this study are also consistent with prior research in young females one to two years post-ACLR, who continued to report significantly worse function than their uninjured peers in spite of similar levels of moderate and vigorous physical activity.36 The athletes in this study averaged 2.4 years post-ACLR, suggesting that this impairment in self-reported function persists several years even amongst those who return to the same level of sports participation.
A score of 90% on the knee-specific SANE is the threshold to identify successful outcomes following ACLR.3 The mean score in the ACLR group was an 89.4, with eight of the 17 athletes (47%) rating themselves lower than 90%, and three athletes (18%) rating themselves at 90%. Despite approximately half of the athletes after ACLR in this cohort rating themselves below the 90% threshold for successful outcomes, these athletes were still able to participate at an elite level of sport without sustaining a secondary ACL injury the season following assessment.
Kinetics
In support of this study’s hypothesis, those with ACLR had lower vGRF in the involved limb during the impact phase of landing compared to controls, suggestive of underloading of the involved limb. The athletes in this study were at least 1 year post-ACLR and averaged 2.4 years post-ACLR. Interestingly, the findings of this study are consistent with athletes who are within 12 months post-ACLR,19 but contradict previous findings on individuals greater than 12 months post-ACLR.37,38 Paterno et. al. examined a cohort of recreationally active females two years following ACLR compared to a control group of female collegiate athletes. They found an increased vGRF during impact phase in the uninvolved limb of the ACLR group, while the involved limb was not different than the control limbs.37 Decker utilized a higher (60 cm box) landing task in recreational athletes at least 12 months from ACLR and found no differences in peak vGRF during impact phase between the involved limb of the ACLR group and a matched control limb, though this peak had a temporal delay in the ACLR group.38 The differences observed in this study relative to previous research may be due to the level of athletic participation: this study examined elite, collegiate athletes, in contrast to the recreational athletes utilized by both Paterno and Decker. Additionally, this control group was matched to the ACLR group given that it utilized the teammates of the ACLR group. These findings suggest that alterations in landing kinetics, suggestive of both underloading relative to teammates and asymmetrical loading between limbs, are still present in elite female athletes who successfully return to sport without subsequent injury.
Kinematics/LESS
In contrast to this study’s hypothesis, those with ACLR had lower LESS scores, indicative of fewer movement errors, compared to their teammates. Previous research has shown that LESS composite scores are worse in both healthy females20 as well as females after ACLR39 when compared to male counterparts, suggestive of poorer movement quality across females overall. The assessment of landing kinematics following ACLR often takes place during the return to sport window,18,19 with only a few studies limited to recreationally active cohorts assessing later time points. These studies have shown worse LESS composite scores compared to matched control subjects.23,24 Bell found a mean LESS scores of 6.7 in an ACLR cohort compared to 5.6 in a healthy cohort.23 Accordingly, Kuenze found a mean LESS score of 6.0 in an ACLR cohort compared to 2.8 in a healthy cohort.24 The mean LESS score of 4.1 in this ACLR cohort was observationally lower than the means in previous research, and statistically lower than the mean of 5.3 observed in control subjects. Hence, this ACLR cohort of elite female athletes had better movement quality than what has been previously reported in recreational athletes following ACLR. This difference may be due, in part, to the level of athlete observed.
With regard to ACL injury risk, prior research has determined soccer athletes with LESS scores of five or higher are at heightened risk of sustaining primary ACL injuries.15 This study’s ACLR group had a mean LESS score of 4.1, with 59% of the group scoring a four or lower, suggestive of good movement quality and lower risk of ACL injury. Accordingly, no athletes in this cohort sustained a subsequent ACL injury the following season.
Combined Findings
In combination, findings suggest that elite female athletes after ACLR have fewer kinematic errors than their teammates, despite lower self-reported function and kinetic underloading and asymmetry. All athletes were able to participate in sport the following season without subsequent ACL injury, suggesting that they were able to attain a safe short-term return to sport, despite the deficits observed. This is particularly important given that a high proportion of secondary ACL injuries occur within the first year following return to sport.40,41
One interpretation of these findings is that elite athletes are able to learn good movement patterns following ACLR during the extensive rehabilitation process. The differences observed between this elite athlete cohort and recreational athletes23,24 may be due, in part, to differences in level of athletic participation and skill. Elite athletes attain good movement quality despite worse self-reported function and kinetic loading patterns. Given that no athletes in this cohort sustained a second ACL injury the following season, this suggests good movement quality, indicated by a lower LESS score, may be a short-term mediator of the high-risk kinetic loading patterns observed in this cohort. The divergent kinetic and kinematic findings are supported by a recent meta-analysis that found asymmetry was more often identified in kinetics compared to kinematics during double limb landing tasks post-ACLR.19 This highlights the potential utility of including both measures as a part of an athlete’s functional assessment.
Potential Study Limitations
One limitation of this study is the lack of comparable data on these athletes at the time of return to sport. Both biomechanical42 and psychological43 variables at the time of return to sport are predictive of second ACL injury after return to sport in young athletes, and thus an athlete’s profile at this time provides insight to their future injury risk. It is unknown if the profile observed in these athletes upon successful reintegration to elite sport was similar to their profile at the time of return to sport. Further longitudinal research is recommended to examine if and how an athlete’s profile changes during this time period and if changes observed relate to secondary injury risk. Despite lacking serial assessments, there were no primary or secondary ACL injuries observed during the competition season following assessment.
The monitoring period of the study specifically tracked ACL injuries, as this was the primary variable of interest. Athletes may have sustained other time-loss injuries, but these were not accounted for in the present study. Additional research could incorporate monitoring all lower extremity time-loss injuries. Additionally, exposure was not tracked during this period. While all athletes participated in sport without restriction, it is unknown how many total minutes of participation each athlete had during competition. If athletes in the ACLR group had limited playing time during competition, this may have significantly lowered their risk for a second ACL injury, especially given that these injuries may be more common in competition compared to practice.44 Additionally, longer-term implications beyond one competition season cannot be inferred. Further research is warranted to better understand how the attainment of good kinematics despite altered kinetic loading influences longer term risk of secondary ACL injury and additional long-term sequalae following ACLR.
Random assignment of the “involved” limb in the control group was utilized in order to assess both limbs for comparison, meaning that there was no account for a potential influence of limb dominance on magnitude of peak vGRF between limbs. Peak vGRF does not differ in landings in healthy female athletes between the dominant and non-dominant limb.29 However, recent work has shown that limb dominance influences intra-limb energy absorption both during a single limb landing task in healthy individuals45 and during a double limb landing task post-ACLR,46 though neither study reported the peak vGRF. Future research should incorporate matching based on limb dominance to control for its potential influence on kinetic symmetry.
In an effort to create a time-efficient screening assessment of these athletes, there was no three-dimensional motion capture data to allow the calculation of knee-specific loading, calling into question how the values of peak vGRF in the present study may relate to the knee in particular. Prior research has shown that six months post-ACLR, vGRF asymmetry predicts knee sagittal plane kinetic asymmetries in both double and single limb landing tasks.47 Accordingly, a meta-analysis identified that ACLR has a large effect on asymmetry in peak vGRF and peak knee extension moment symmetry during double limb landing tasks.19 Given previous findings, it is reasonable to infer that the asymmetry of vGRF observed in the ACLR group in this study would likely correspond to an asymmetrical knee-specific load as well. While motion capture could further detail loading across the knee, in the absence of this measurement, there is still clinical utility in the assessment of peak vGRF.
CONCLUSIONS
This study examined elite collegiate female athletes, a population which is under-represented in current research despite a high risk of injury. The results suggest that elite female athletes after ACLR continue to report decreased knee-related function and demonstrate kinetic differences suggestive of both asymmetrical loading and underloading relative to teammates during double limb landing tasks despite successful return to sport without secondary ACL injury. In contrast, these athletes demonstrate fewer kinematic errors relative to their teammates. These conflicting findings suggest that incorporation of both kinetic and kinematic measurements may be important to fully understand an athlete’s functional profile. Given that these athletes did not sustain a secondary ACL injury for the monitoring period following assessment, the good movement quality observed may be protective against the functional deficits reported and kinetic differences observed. Further longitudinal research is warranted to understand how functional profiles relate to longer-term outcomes following ACLR and return to elite sport in female athletes.
Conflicts of Interest
The authors report no conflicts of interest.