INTRODUCTION
Preseason screening for body composition, bone health, range of motion, flexibility, balance, and multidimensional hip strength have become common practice in several professional and collegiate sport settings.1 Athletic injuries and the long-term sequalae that emerge as a result remain a primary concern in athletics for coaches, trainers, physical therapists, and physicians. In particular, soccer athletes often present with higher rates of injury relative to other team based sports.2 When observing NCAA sports teams, both women’s and men’s soccer are among the highest reported rates of ankle sprains as well as quadriceps and hamstring strains.3,4 Anterior cruciate ligament tears are also common, and have a four to six times higher incidence in female soccer players compared to males.3,4 Imbalances in strength, flexibility, movement, and neuromuscular control all pose as risks for athletic injuries which may adversely affect both athletes and their teams through time lost from playing, suboptimal team performance, and difficulties returning to preinjury performance level. As a result, many professional and collegiate sports teams have adopted the practice of preseason movement and balance screening for the purpose of injury prevention.5,6
The Y-balance Test (YBT) and Functional Movement Screen (FMS™) are two common measures performed to evaluate dynamic flexibility and stability.1 The YBT can be used for evaluation of both the upper extremity and lower extremity. The lower quarter YBT (LQYBT), was derived from the Star Excursion Balance Test (SBET) used to evaluate lower extremity balance and stability with multidirectional reaches.7 The FMS™ seeks to identify functional limitations or asymmetries through the evaluation of movement patterns that together measure range of motion, stability, and balance.4,8–11 During the FMS™, athletes perform a series of seven tasks (deep squat, hurdle step, in-line lunge, shoulder mobility, rotary stability, active straight leg raise, trunk stability pushup) and are scored on a criterion-based Likert scale based on their performance for each task.9,10 These scores are used to derive a composite score. Both assessments have been designed to provide athletic trainers, coaches, and physicians with baseline metrics for tracking player mobility and function throughout a sport season and during rehabilitation from injury.
The YBT and FMS™ have generally been utilized as one-size–fits-all assessments. While numerous studies have examined the utility of YBT and FMS™ as injury prediction tools, conclusions of these studies remain inconsistent.1,12,13 This inconsistency may be in part due the homogeneity of many of the study populations, often only including participants of a single sport, sex, or profession without taking into account other potential variables that may influence scoring. With regard to sex, body composition, and skeletal dimensions (bone length, pelvic width, etc.) little is known about how these variables may impact the conclusions of these assessments. Such information may help refine current testing protocols and increase the clinical relevance of screening in assessment of baseline performance and injury risk. Therefore, the primary aim of this investigation was to determine the relationship between demographic and anthropometric factors such as sex, body composition, and skeletal dimension and scoring on YBT and FMS™ in male and female professional soccer athletes. The authors hypothesized that YBT and FMS™ scores would differ between male and female professional soccer athletes and that variables such as body composition and skeletal dimensions would correlate with test scoring and interpretation.
METHODS
Study Design
This study was a single timepoint cross sectional design and the following protocol was approved by the Houston Methodist Institutional Review Board for research involving human subjects. All participants provided informed consent prior to participation.
Participants
Professional soccer athletes (Major League Soccer, MLS®; National Women’s Soccer League, NWSL®) from two separate clubs were recruited to participate in this investigation during each team’s preseason evaluations and screening. Both professional organizations were local to the research team. All active roster athletes without ongoing injury (lower extremity injury resulting in activity limitation < six months prior) or other limitations were offered participation to which none declined consent. These athletes were to undergo other preseason multidisciplinary screening measures on the same day, independent of this investigation. All screening took place in the same location using the same licensed physical therapy team during all evaluations.
Procedures
On the morning of the study, all subjects underwent body composition and skeletal analysis assessed with a DEXAscans (Lunar iDXA, GE®, Boston MA) scan. Full body scans were obtained. Imaging software (ImageJ, Version 1.8.0-172, NIH) was later used (in a similar manner to Stanelle et al.14) with full body DEXA scan images to quantify trunk length, pelvic width, femur length, tibia length, shoulder width, humerus length, and radius length. Bilateral measurements of the extremities were averaged and demonstrated interclass correlation coefficients of >0.95 for all measures. All measures were performed and recorded by the same team of three trained laboratory technicians. Lower body balance and stability were assessed using standard YBT and FMS™ protocols.9,15
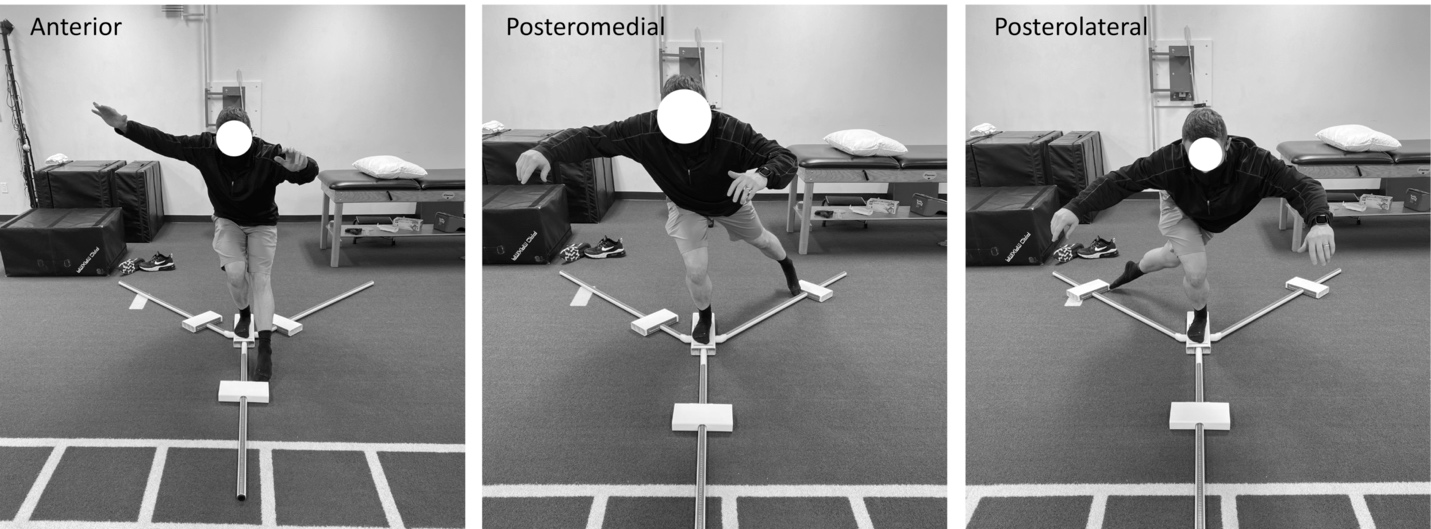
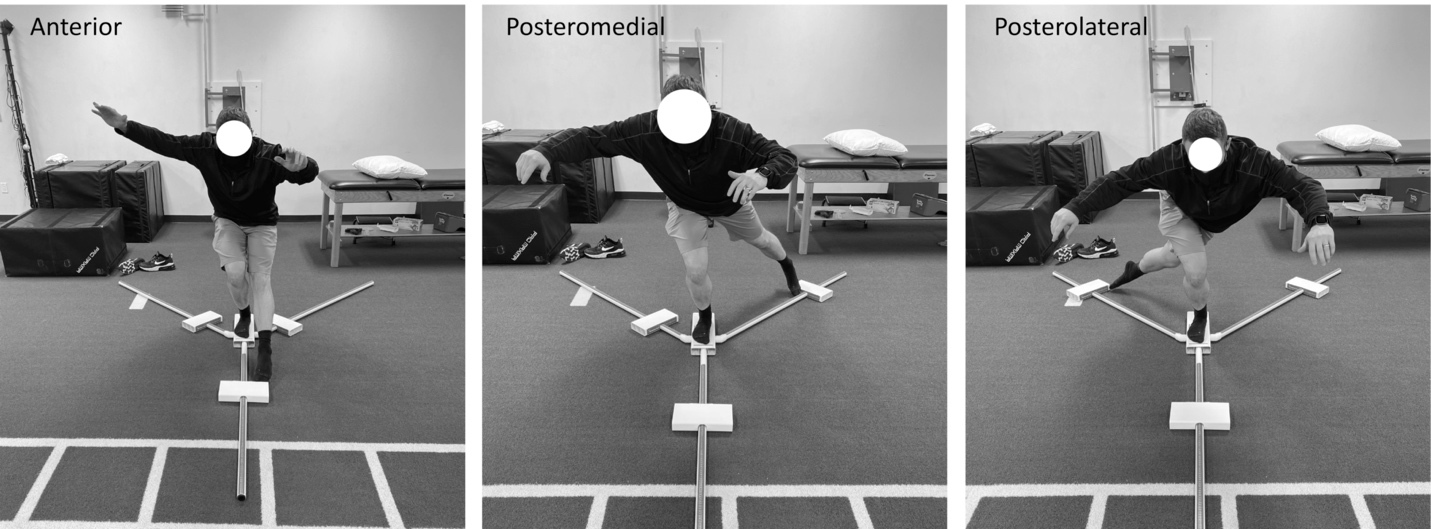
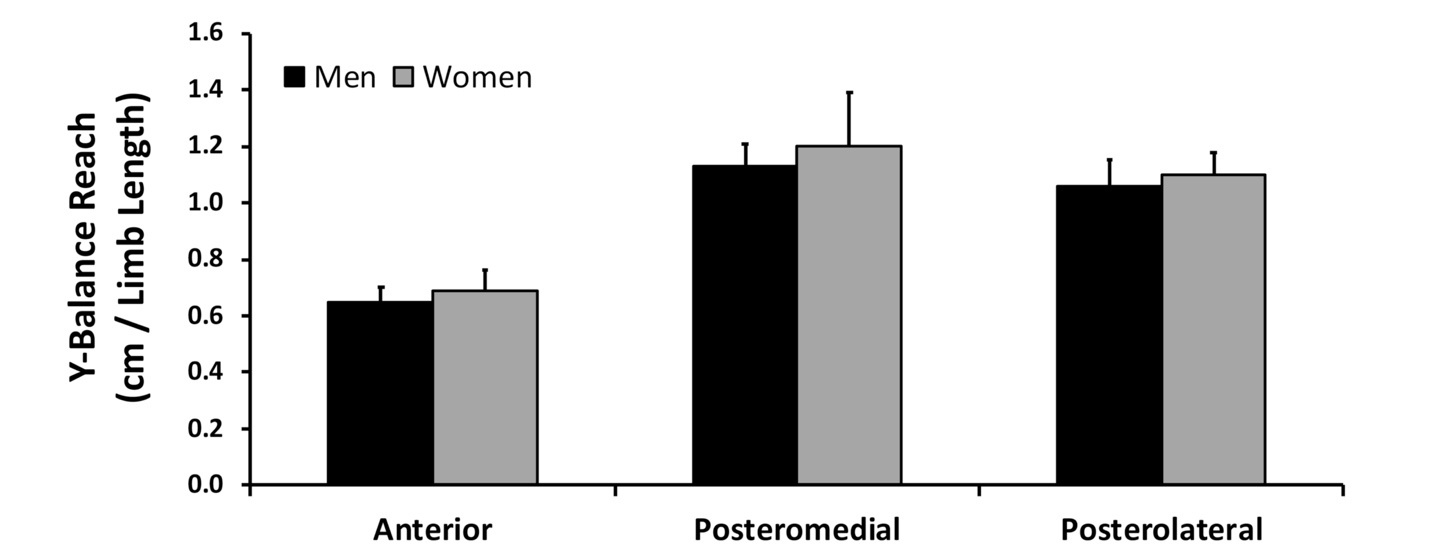
Dynamic balance was measured using the YBT (Figure 1) using the Y-Balance Test Kit™ (Functional Movement Systems, Chatham, VA). Athletes were instructed to balance on one leg while simultaneously reaching as far as possible in three different directions: anterior, posteromedial, and posterolateral. This was performed bilaterally, and distance reached in each direction was recorded. A sum of the total reach distance was done for each leg and normalized to the respective limb length to form a composite score.
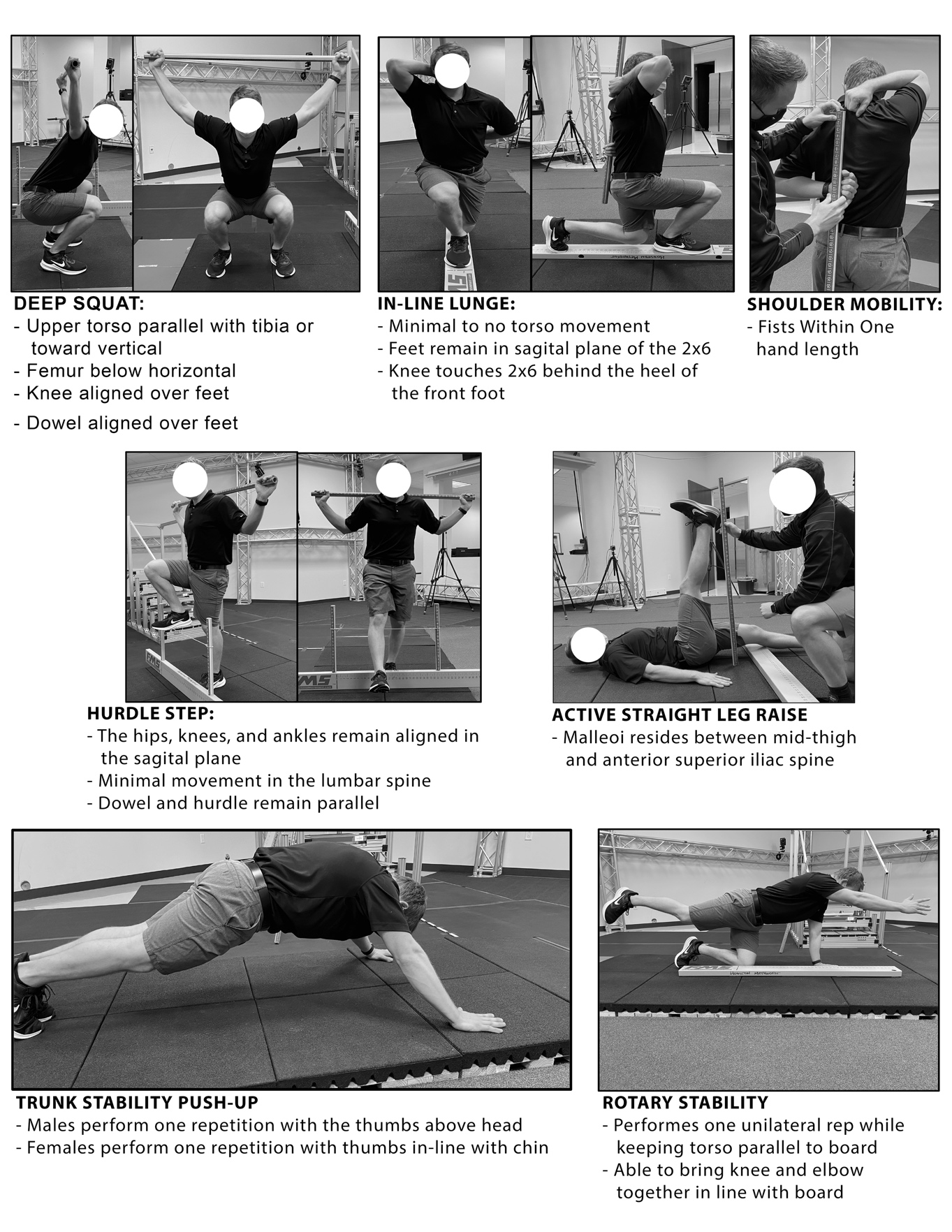
The FMS™ was then conducted with the athletes. The seven tasks were scored individually on a scale of 0 (worst) – 3 (best) depending on athlete performance quality for each screening movement (Figure 2). Specific criteria for each movement have been previously published.9 A score of 3 indicates that the athlete was able to perform the movement as directed without compensation. A score of 2 indicates that the athlete performed the movement but with compensation or imperfection. A score of 1 indicates that the athlete was unable to perform the movement. A score of 0 was used if the athlete experienced any pain during the movement regardless of the quality.

Statistical Analysis
Independent samples two-tailed t-tests were used to compare body composition, YBT score, bone length, bone width, and trunk length between sexes. Chi-square analysis was used for comparison of FMS™ test scores between sexes. In instances where significant pair-wise comparisons were observed, effect sizes were calculated using either a Cohen’s d statistic (t-test) or a Phi Statistic (Chi-square) whereby effect sizes (ES) were interpreted as follows: 0.0-0.1, Negligible (N); 0.1-0.3, Small (S); 0.3-0.5, Moderate (M); 0.5-0.7, Large (L); >0.7, Very Large (VL).16 Pearson’s correlation analysis was used to determine if body composition and bone length was correlated with Y-balance scores. Spearman’s Rank Order correlation was used for the same analysis of ordinal FMS™ scores. Statistically significant correlational strength was defined as weak (r < 0.4), moderate (r = 0.4-0.7), and strong (r > 0.7). Type I error for all analyses was set at α=0.05. Using a minimum detectable difference of 10% in YBT scores and 30% in FMS™ classification frequency between sexes as well as a minimum overall correlation strength of 0.3 for mobility measures at a power of 0.80, it was determined a minimum sample size of 15 athletes would be required per group.
RESULTS
Twenty-four male (27±5 y; 181.6 ± 8.1cm; 79.7 ± 8.8kg) and sixteen female (25±3 y; 168.1 ± 5.8cm; 63.0 ± 4.4kg) subjects participated. Baseline demographics are shown in Table 1 where differences between sexes were observed for all demographic variables (p<0.001) with the exception of BMI.
Skeletal Dimensions
Comparison of skeletal dimensions between male and female athletes are shown in Table 2 where significant differences between sexes were observed for trunk length, humerus length, shoulder width, radius length, pelvic width below femoral head, femur length and tibia length (p<0.05). No differences were observed between sexes for greatest pelvic width.
Functional Movement Screen
Variables of skeletal dimensions were observed to be significantly correlated with FMS™ scoring for the deep squat, in-line lunge, and straight leg raise (p<0.05). Moderate negative correlations were found between the deep squat score and total lean mass (r = -0.43), trunk lean mass (r = -0.40), and height (r = -0.40) (p<0.05). Moderate and strong negative correlations were observed between the in-line lunge score and height (r = -0.63), total lean mass (r = -0.77), trunk lean mass (r = -0.73), and leg lean mass (r = -0.70). A moderate positive correlation was observed between pelvic width and the deep squat (r = 0.40), in-line lunge (r = 0.60), and active straight leg raise (r = 0.45) scores (p<0.05). For each of the exercises mentioned (deep squat, in-line lunge, and straight leg raise), the female athletes were observed to score higher than the males (p<0.05). (Table 3).
Y-Balance Screen
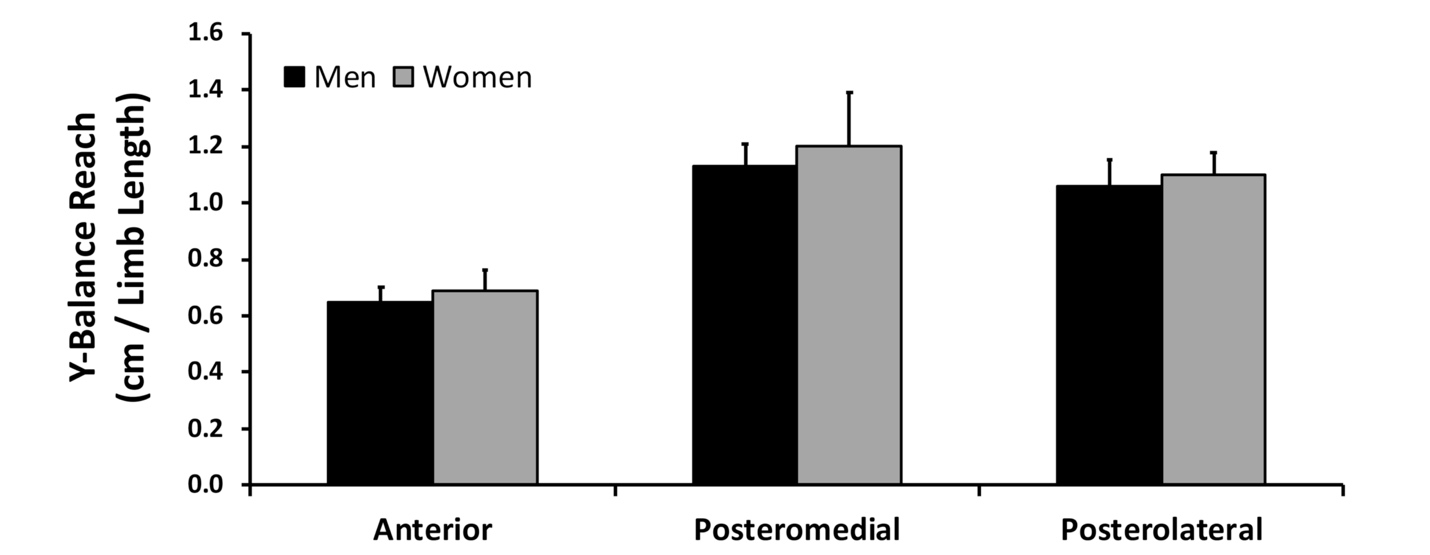
Results for the YBT are shown in Figure 3. YBT measurements were taken for reach in the anterior, posteromedial, and posterolateral directions. No differences in Y-balance measures were observed between sexes after normalizing to individuals’ limb-length as is common in clinical assessment. Weak negative correlations were found between anterior reach and height, total lean mass (r = -0.36), leg lean mass (r = -0.39), and trunk lean mass (r = -0.39) (all p<0.05). Moderate positive correlations were found between posterolateral reach and pelvic width below the femoral head (r = 0.42), femur length (r = 0.44), and tibia length (r = 0.051) (all p<0.05).
DISCUSSION
The YBT and FMS™ are frequently used measures that have been suggested for use in predicting athletic injury risk often used in a one–size-fits-all manner. The primary aim of this investigation was to determine the relationship between demographic and anthropometric factors such as sex, body composition, and skeletal dimension and scoring on the YBT and FMS™ in male and female professional soccer athletes. Consistent with the hypothesis, several of these factors were observed to be significantly correlated with test performance. The findings of these study highlight possible sources of bias that may influence test scoring. Although further study remains needed, the findings from this investigation provide potential target variables that may be further explored and potentially incorporated into the development of future screening tools.
Sex, Body Composition, Skeletal Dimensions, and FMS™ Scoring
In this investigation, significant differences were found between male and female athletes for the FMS™ test with a greater percentage of female athletes scoring in a higher classification than male athletes for deep squat, in line lunge, and straight leg raise (Table 3). While female athletes may be scoring more favorably than their male counterparts in these screens of fundamental movements, the literature has several reports of higher rates of injury among female athletes in comparison to male athletes.4,17–20 Agel et. al21 reported that women sustain ACL injuries at higher rates than their male counterparts in soccer, basketball, and lacrosse. While the cause of such injuries seems to be multi-factorial, the Q-angle, or the angle of the femur to the tibia, has been loosely described as a potential contributing factor to knee injuries. As observed in this study, females tend to have greater pelvic width, resulting in greater Q-angle. Although this metric may contribute to higher scores in lower body mobility tests, it may also contribute to risk of knee injury, though the causal aspect of this relationship has yet to be confirmed.22 This indicates that other factors likely impact scoring performance on these generalized assessments which in turn may explain the reduced utility of assessments such as FMS™ and YBT to reliably predict injury risk or compare injury risk among athletes with differing musculoskeletal builds. Based on the results of this investigation, the authors hypothesize that biomechanical features that contribute to a lower center of gravity with a wider base of support and lower mass represent a key source of FMS™ testing bias.20,23
Expectedly, differences were observed in body composition and musculoskeletal dimensions between sexes in this study. Overall, the female professional soccer athletes had reduced height, lower body mass, lower lean mass, wider pelvic width, shorter femur length, and shorter tibia length than the male professional soccer athletes. Based on the given results, these factors likely contributed to a potential anatomical advantage that resulted in greater FMS™ test performance for the lower body. However, female soccer athlete injury rates still remain different compared to male athletes with non-contact injuries being more likely to occur in females and contact based injuries being more frequent in males.3,21 Male athletes are also more likely to sustain quadriceps strains while female athletes are more likely to sustain hamstring strains.3,4,18,19 Lastly, sex-based differences in muscle activation patterns during activity have been previously observed.23 Padua et al.23 found that across two-legged-hopping conditions the women demonstrated 46% more quadriceps muscle activity than men. Increase in quadricep activation could lead to increasing levels of fatigue, therefore putting women at a greater risk for injury. Therefore, regarding the present results, rather than being at reduced risk of injury, there may be a scoring bias in the FMS™ screen that benefits female athletes due to certain inherent anatomical features such as pelvic width, height, and lean mass.
Anatomical Factors Associated with Y-Balance Performance
Similar to the FMS™, the YBT measures were correlated with anatomical factors (lean mass and skeletal dimensions) whereby less lean mass but greater pelvic widths produced higher measures (despite test measures being normalized to limb length). In contrast to the FMS™ screen, skeletal dimensions are somewhat incorporated into the YBT (limb length).24,25 The authors hypothesize that this likely accounts for the lack of difference in YBT measures between men and women (Figure 3). However, the results still indicate that generalizing measures between those with different musculoskeletal builds will likely result in testing bias that cannot be accounted for by sex alone. In a recent systematic review, Plisky et al.24 echo these findings when assessing anterior reach and composite scores among multiple studies.43 However, a large variability in each sex, sport, and age/competition level was present in their included studies, lending to the possibility in composite score variance depending on the sex, sport, and competition level when considered as a whole.24 These authors suggest normative data be established based on a multitude of these factors, and future research should be performed using a wide variety of populations.24
Future Directions
Cumulatively, the findings of the present investigation suggest that it may be of benefit for anatomical features not typically considered in the FMS™ or the YBT to be incorporated, or considered in tandem with the respective tools. Such factors may also be considered when tailoring exercises to address mobility deficiencies as is common for FMS™ screening.5 Notably, data are currently conflicting on whether or not FMS™ scoring are predictive of future injury frequency.5,26–28 For example, Moran et al.27 recently performed a meta-analysis of 24 investigations and reported that present data suggest that the use of FMS™ for injury prevention in soccer athletes was ineffective and that its efficacy was conflicting among in the literature among other sports (American football, basketball, ice hockey, running, and first responders such as police and firefighters). Therefore, it is possible that the anatomical scoring bias observed here may have contributed to some of the lack of predictive utility observed in other investigations. Future research will need to determine how any additional metrics may be best incorporated into algorithms to reduce scoring bias in these types of athletic populations and whether or not eliminating such bias will improve clinical utility for injury risk assessment.
Limitations & Conclusions
This investigation is not without limitations. Data collection and access to professional athletes is often limited and, although powered appropriately for comparisons in this investigation, participants were included from only two individual clubs which may limit generalizability across the studied populations. Participants in this study ranged in age from 22 to 32 years of age. This is a limited age range, and the authors acknowledge that there may be developmental differences in younger and older athletes that may also be associated with performance in the measures observed here. Although several factors were identified to be associated with testing bias, it is not yet clear how or whether these metrics should be incorporated into current scoring systems for FMS™ and YBT and whether or not doing so would significantly the value of these assessments for injury risk screening. Therefore, further study will be required to examine which factors identified here may best be incorporated into FMS™ and YBT to reduce scoring bias and better predict injury risk. For example, evaluating the collinearity between some of the measures (possibly due, in part, to differences between sexes) reported on here in a larger study cohort may help to reduce total number of additional factors needed to reduce scoring bias. Lastly, while data exists in previous literature regarding injury frequency norms in male and female soccer athletes, the investigators in this study were not able to access injury history information on this group of athletes. Such information may have assisted in determining whether FMS™ or YBT scores were correlated with injury history across sports seasons.
Conclusion
In summary, the results of this study indicate that sex-based differences observed between sexes for lower body components of the FMS™ and YBT measures may be attributed to anatomical variables such as height, lean mass, and skeletal dimensions that impact both FMS™ and YBT scoring, respectively. While the YBT and FMS™ were designed to evaluate dynamic joint mobility and fundamental movement competency, their use for potential risk for injury based on a one-size-fits-all generalized criteria is questioned. These assessments are likely better suited for use on a more individualized basis rather than comparing across groups of athletes. Further research is needed to determine if, and to what degree, sex, body composition, skeletal dimensions, and dynamic motion analysis might be incorporated in to scoring criteria or predictive modeling to enhance the use of these clinical assessments for predicting risk of injury.
Conflicts of Interest
The authors have no conflicts of interest to disclose and no funding support was provided for the work presented in this manuscript.