
INTRODUCTION
Greater trochanteric pain syndrome (GTPS) refers to pain in the lateral hip and thigh and can encompass multiple diagnoses including external snapping hip (coxa saltans), also known as proximal iliotibial band syndrome, trochanteric bursitis, and gluteus medius (GMed) or gluteus minimus (GMin) tendinopathy or tearing.1,2 Although the symptoms associated with GTPS were previously thought to be primarily the result of trochanteric bursitis, multiple histologic and imaging studies have identified gluteal tendinopathy with or without bursitis as the primary source of pain and dysfunction.3–5 GTPS presents clinicians with a diagnostic challenge as no cluster of special test exists to identify the specific pathoanatomical structure involved or the severity of its involvement. Therefore, there is a need for an impairment-based classification system for GTPS to allow for tailored conservative treatment interventions and improved patient outcomes.
The use of the term GTPS is non-specific to pathology and refers to the many sources of pain in the lateral hip. This is similar to the use of the term “non-specific low back pain”, which encompasses many different pathologies including but not limited to muscular strains, spinal stenosis, and intervertebral disc degeneration.2 Instead of using special tests to identify the specific anatomical structure involved, which is common practice for many peripheral joints, examination procedures for the low back focus on the identification of impairments that lead to the development of pain.6 It has been suggested that identifying the specific anatomical structure involved in the onset of low back pain is not necessary to achieve successful resolution of pain.7–9 As a result, an impairment-based treatment classification approach is recommended in an attempt to tailor treatments to a particular subgroup depending on subjective and objective findings. GTPS presents clinicians with a similar diagnostic challenge as non-specific low back pain with special tests being unable to identify the specific pathoanatomical structure involved and do little to guide the clinician in prescription of treatment interventions. Like the low back, the development of GTPS has been linked to movement systems abnormalities during functional activities. The primary movements system finding is the loss of pelvic control in the frontal plane secondary to hip abductor weakness and/or pain.10,11 Therefore, conservative interventions should focus on the correction of these impairments to reduce pain and improve movement control in individuals with GTPS.
The purpose of this clinical commentary is to present an impairment-based classification system for GTPS to allow for tailored treatment interventions. Grimaldi & Fearon12 presented a graded exercise program for the treatment of GTPS. Because the focus of their work was based solely on gluteal tendinopathy, further classification based on tissue irritability is warranted.12 We propose a classification system based on findings identified during a standard physical examination coupled with findings from a movement system assessment. By addressing identified impairments, treatment will focus on correcting the faulty mechanics that lead to the development of GTPS rather than treatment being aimed towards a single anatomical structure.
GREATER TROCHANTERIC PAIN SYNDROME
GTPS has an incidence of 1.8 out of 1000 patients in the primary care setting, mainly affecting females in the 4th-6th decades of life.13–17 Multiple studies have demonstrated a higher incidence of GTPS with concomitant low back pain, hip osteoarthritis (OA), iliotibial band tenderness, and knee pain.18,19 While the majority of GTPS is observed in middle aged females, at a much lower rate runners, football players, and dancers have also shown to be affected due to high hip adduction moments during performance of their respective sport.s17,20–22 In general, abnormal forces across the hip secondary to faulty biomechanics are hypothesized to lead to GTPS. Specifically, weakness or pain in the hip abductors results in a loss of pelvic control in the frontal plane, presenting as a Trendelenburg or compensated Trendelenburg position during tasks performed on a single leg. Pelvic obliquity increases the compressive forces through the lateral hip leading to degeneration of the GMed and GMin tendons and/or inflammation of the trochanteric bursae and proximal iliotibial band.23
Individuals suffering from GTPS complain of pain at the lateral hip, with symptoms potentially radiating distally to the level of the buttock and lateral thigh. Pain generally worsens with single limb weight bearing activities and laying on the affected side. The greatest degree of tenderness should specifically be located on the lateral or posterior aspect of the greater trochanter.3,15,24,25 Activities that exacerbate symptoms include walking and ascending stairs, as well as other single leg activities, such as putting on pants or getting in/out of the bathtub. Due to the high likelihood of overlapping pathologies, particularly hip joint osteoarthritis and low back pain, it is important to first assess for the presence of intra-articular hip and/or lumbar spine pathology. It is also important to rule out the presence of a femoral stress fracture or avascular necrosis of the hip which would require a physician referral.19 Individuals complaining of radiating pain below the knee, pain in the low back that increases with sitting or walking, and pain specifically associated with movement of the lumbar spine should undergo a comprehensive lower quarter screen. This examination should assess for myotome related weakness, decreased sensation in dermatomal pattern, abnormal findings during lower extremity reflex testing, and lumbar range of motion.
For those with groin pain and morning stiffness hip osteoarthritis should be considered.26 Intra-articular hip joint pathology should be considered with the reproduction of groin pain during a Flexion-Abduction-External Rotation (FABER) test and/or Scour test, decreased range of motion in a capsular pattern, and demonstration of an antalgic gait pattern.27 With subjective findings including a rapid increase in weightbearing activities or excessive steroid or alcohol use, a femoral stress fracture or avascular necrosis of the hip, respectively, should be considered. If the objective examination is consistent with either of these diagnoses and an immediate referral to a physician is warranted. A summary of differential diagnoses can be found in Table 1.
While special tests are frequently utilized in the clinical setting to identify GTPS, there is currently no test or cluster of tests utilized to identify which specific pathoanatomical structures are involved or the severity to which they are involved. Some frequently utilized special tests include resisted hip abduction and external rotation, FABER, the resisted external de-rotational, and Trendelenburg tests. Ganderton et al.28 found the FABER, resisted hip abduction, and the resisted external de-rotational tests to have the highest diagnostic test accuracy in confirming GTPS. Previous research on the Trendelenburg test and the resisted external rotation test has reported sensitivity and specificity values in individuals with GTPS of 73% and 77% and 88% and 97.3%, respectively.4,29 Multiple authors have also identified palpation of the greater trochanter and trochanteric bursae to be a useful tool in confirming the presence of GTPS.5,17,28 It should be noted, however, that no studies report sensitivity and specificity values for these palpatory tests in identifying the specific pathoanatomical structure involved. Therefore, it should be emphasized that these tests have minimal utility beyond confirming the presence or absence of GTPS and offer little to the clinician in prescribing appropriate treatment interventions.
Given the limited clinical utility of special tests, clinicians should focus on examination procedures that identify the impairments responsible for the development and persistence of GTPS. Previous research has established hip abductor weakness, loss of pelvic control in the frontal plane, and iliotibial band tightness and thickening as factors increasing compressive forces through the bursae and GMed and GMin tendons.10,11 Identifying impairments in hip flexibility and strength will assist with identifying individuals who will benefit from stretching and strengthening exercises and/or manual interventions. Along with standard range of motion, strength, and flexibility screens, a thorough analysis of the movement system should be performed. Movement system assessments are evaluations of biomechanics during functional activities providing insight into faulty movement patterns allowing clinicians to tailor treatment interventions to address identified impairments.30
IMPAIRMENT BASED TREATMENT CLASSIFICATION
Since the mechanism for developing GTPS has been identified as strength and biomechanical deficits of and around the hip, an impairment-based treatment classification, similar to those described for the low back, may be useful to help appropriately tailor treatment interventions.10,11 We recommend classifying patients presenting with GTPS into two categories, contractile and/or non-contractile, and then further sub-classifying based on irritability.
Contractile
A patient with a contractile presentation would report a reproduction of pain with resisted hip abduction, lengthening or stretching of the hip abductors, palpation of the gluteal muscles and/or tendons, and would demonstrate faulty mechanics during functional activities. Any of these findings would suggest the gluteal muscles, proximal iliotibial band, and/or tensor fascia latae are involved. However, it does not indicate which specific structure or the severity of involvement. Therefore, we recommend identifying the irritability of muscular involvement as high or low before prescribing interventions. Treatment for a contractile presentation should focus on muscle and tendon healing through soft tissue mobilization (STM) and graded loading exercises. In patients demonstrating severe pain, profound weakness, and a significant limited ability to walk without an assistive device, a physician referral is warranted to rule out a compete tear of the hip abductors.
High Irritability
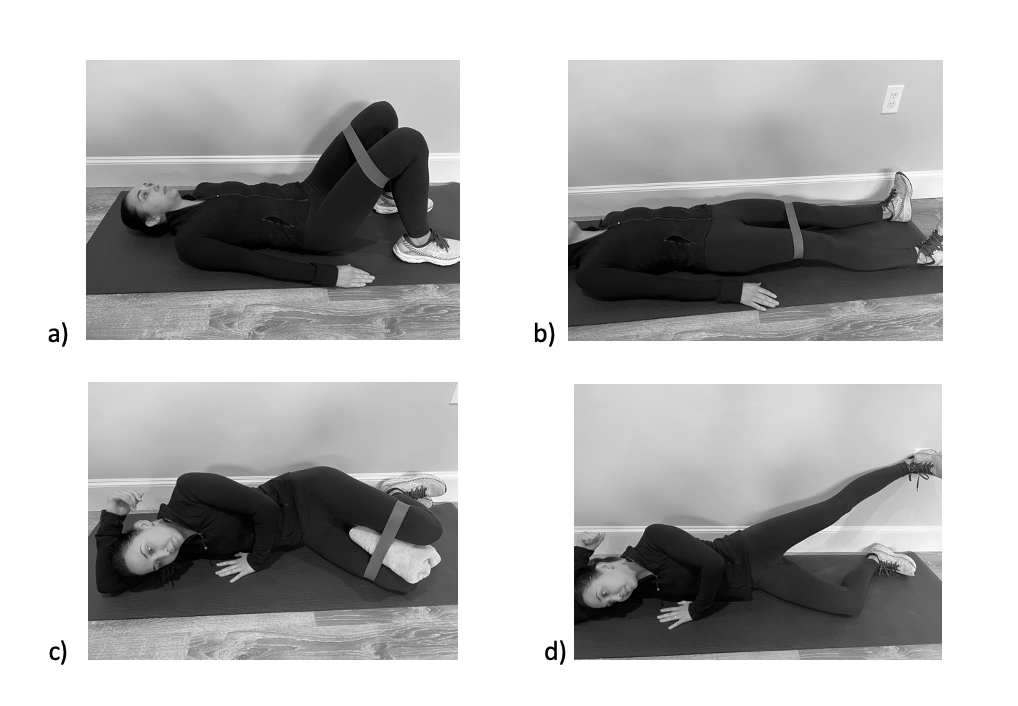
Highly irritable individuals in the contractile classification will be unable to abduct their hip against gravity and report moderate to severe reproduction of pain. The patient may also report severe difficulty with functional tasks involving single leg stance (SLS) and exhibit an antalgic gait. During this phase, STM to the gluteal muscle bellies, tensor fascia lata (TFL), and/or iliotibial band (ITB) are recommended to facilitate healing. STM of the gluteal tendons and trochanteric bursae should be avoided to limit further tissue irritation. GMed and GMin strengthening should be initiated through isometric contractions in gravity eliminated positions progressing to against gravity positions as tolerated. Low intensity isometrics have been shown to induce analgesic effects in individuals with patellar tendinopathy, however, these results are variable across populations.31 We therefore recommend a graded exercise program progressing from isometric contractions in the high irritability phase progressing to isotonic contractions in the low irritability phase. Core exercise should be initiated in supine and quadruped with a focus on proper activation of the lower abdominals. During this phase, all activities should be pain-free. Examples of gluteal and core exercise progressions for the high irritability phase can be found in Figures 1 and 2.
_in_a)_short_lever_arm__g.png)
_alternating_upper_extremity_movement__b)_.png)
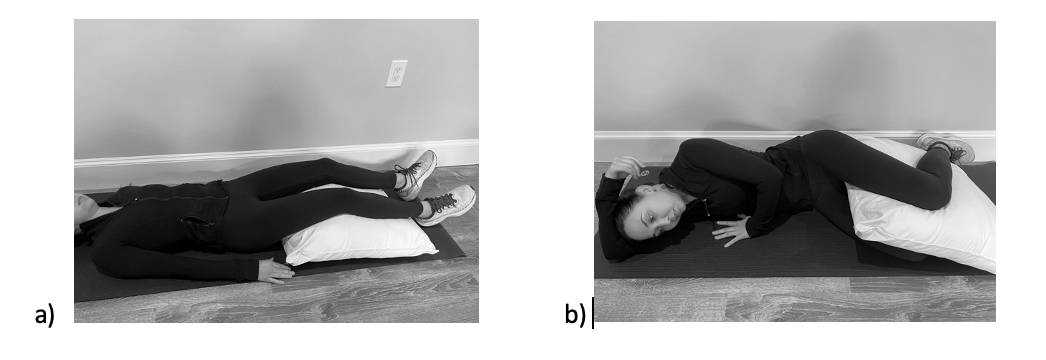
Along with a tailored exercise program, extensive education should be provided regarding activity and postural modifications with the goal of reducing load and compression through the lateral hip. Strategies should be given to help minimize time spent on a single leg during activities of daily living, such as sitting rather than standing to put on pants thereby reducing tensile load through the gluteal muscles. The importance of avoiding hip adduction should be stressed for sitting, standing, and sleeping to limit excessive compression through the lateral hip.12 For example, education should be provided to avoid crossing legs in both sitting and standing and to sleep in supine with a pillow under their knees or in sidelying with a pillow between their legs (Figure 3).
_supine_and_b)_sidelying.png)
Low Irritability
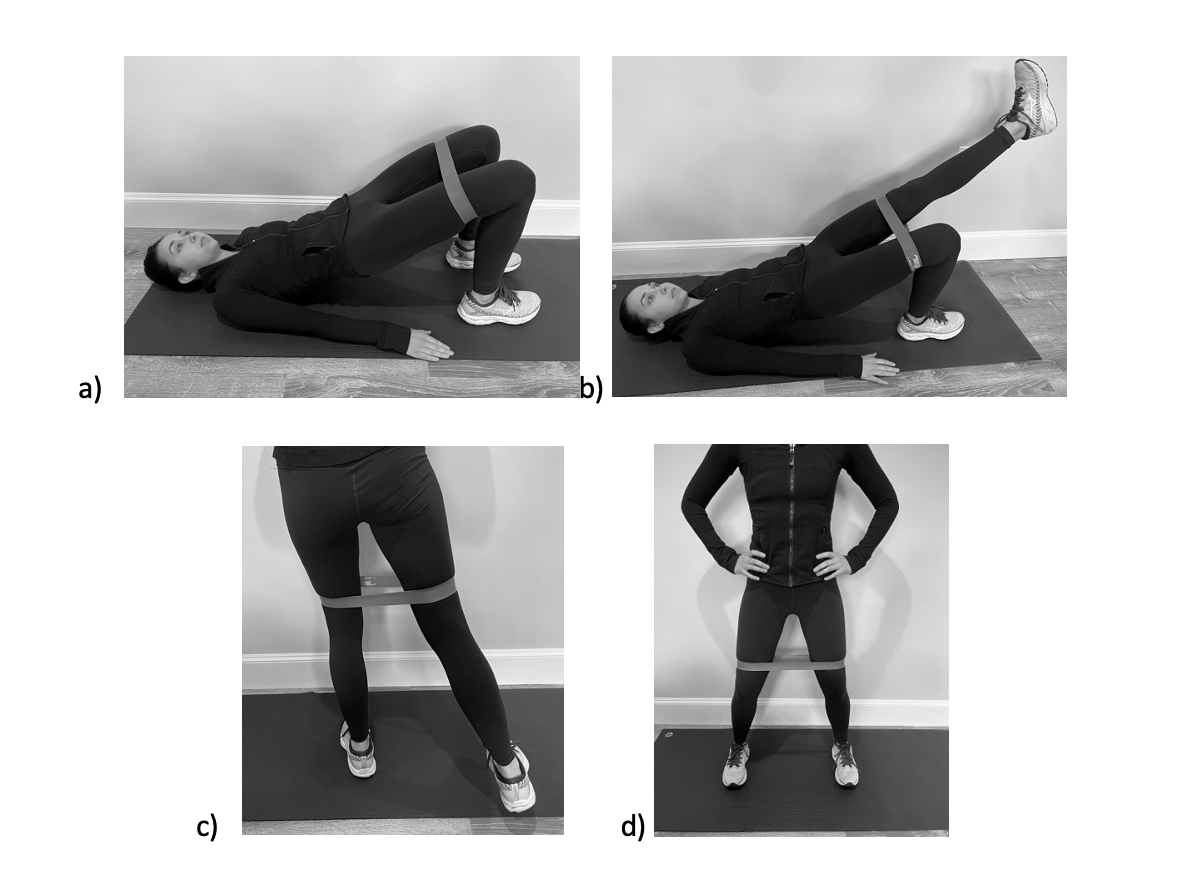
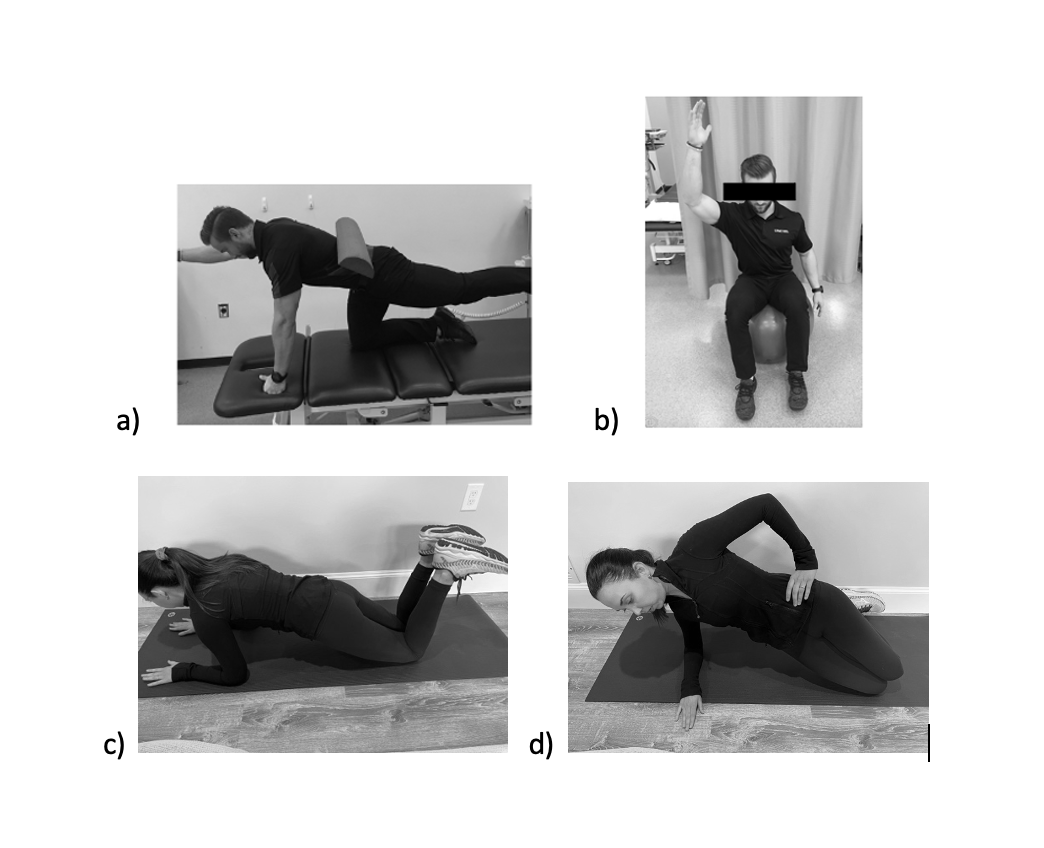
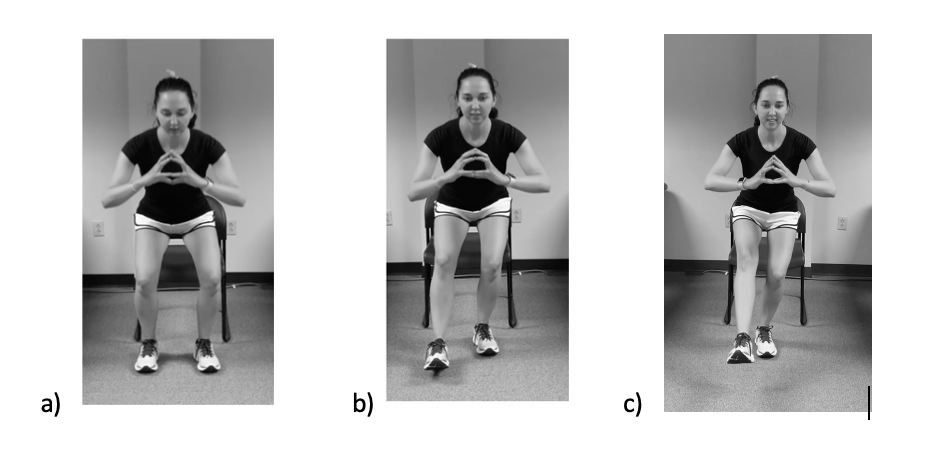
Those with low irritability of the lateral hip musculature will be able to abduct their hip against gravity, but continue to complain of mild to moderate reproduction of pain. Treatment recommendations for this phase include initiation of pain-free stretching of the hip abductors, concentric and eccentric hip abductor strengthening, functional training focusing on single leg activities, and progression of core strengthening. STM should continue to be utilized in conjunction with pain-free stretching if tightness was identified through muscle length testing, such as an Ober’s test. It should be noted that soft-tissue mobilization should be directed at the gluteal muscle bellies, TFL, and/or ITB, not at the trochanteric bursae or gluteal tendon insertions, to avoid further tissue irritation.19 GMed and GMin strengthening should be progressed to include isotonic contractions in the low irritability phase as the focus shifts from pain control and healing to restoration of function. Heavy slow resistance exercise has been shown to improve tendon quality and compared to eccentric exercise, heavy slow resistance exercise yielded similar clinical outcomes.32–34 We therefore recommend a combination of concentric and eccentric exercise as per pain tolerance. A large focus should be given to weight bearing hip abductor strengthening as weight bearing abductor exercises demonstrate significantly greater EMG activity than all non-weight bearing exercise, except sidelying hip abduction.35 If tolerated, a resistance band should be incorporated to increase hip abductor activation and challenge lower extremity neuromuscular control. A GMed and GMin strengthening progression for the low irritability phase can be found in Figure 4. Core exercises should be progressed to incorporate a plank progression as well as weight bearing functional tasks. Careful attention should be paid to frontal plane control of the pelvis during all weight bearing strengthening exercises.
_for_the_low_irri.png)
_bird_dog__b)_transverse_abdominis_a.png)
The main goal of this phase is to restore appropriate pelvic control during functional tasks. Similar to the strengthening progression, functional training should begin in double leg stance progressing to the transition from double to SLS and finally to training on a single leg. In order to challenge neuromuscular control, dynamic functional training should be incorporated once the patient demonstrates mastery of static tasks. We recommend beginning the return to activity and sport progression with a walking program to incorporate progressive loading of the gluteal muscles as well as to improve cardiovascular endurance. Once the patient can ambulate 15-minutes with minimal pain and appropriate pelvic control, progression to sport-specific activities including running, jumping, hopping, and cutting should be initiated, if necessary. Progression should be dictated by pain and frontal plane control of the pelvis.
_bilateral_stance__b).png)
Non-Contractile
Individuals exhibiting pain during palpation of or around the greater trochanter, decreased strength of the hip abductors without reproduction of pain during resisted testing, and/or faulty mechanics during movement system evaluations would suggest a non-contractile source of GTPS. It should be emphasized that while these individuals may demonstrate weakness and functional deficiency of the hip abductors, these activities will not elicit pain. Clinicians should also evaluate for any cardinal signs of inflammation, including rubor, erthythema, edema, and tenderness, which indicate involvement of the trochanteric bursae.36,37 Different from a contractile presentation, which focuses muscle and tendon healing through loading exercise, primary interventions for a non-contractile presentation are aimed at reducing compressive forces over the greater trochanter and alleviating bursal irritation and overload of the lateral structures of the hip. Treatment should focus on decreasing inflammation, restoring flexibility of the lateral hip, particularly of the iliotibial band, improving strength of the hip abductors, and improving of functional movement patterns. We again recommend classifying the patient into either high or low irritability to better tailor treatment interventions.
High Irritability
A patient with a highly irritable, non-contractile source of GTPS will exhibit severe signs inflammation. Modalities to decrease inflammation, including heat, ice, ultrasound, low-level laser therapy, shockwave therapy, and electrical stimulation can be utilized.38,39 Gentle soft-tissue mobilization of the structures surrounding the greater trochanter is useful in improving flexibility of the lateral hip. Clinicians should avoid any STM of or in close proximity to the trochanteric bursae as this would increase bursal irritation. Much like the highly irritable contractile presentation, hip abductor strengthening should begin with isometric exercise progressing to concentric exercise only as tolerated by pain. To progressively load the hip abductors and endure proper control of the pelvis, we recommend beginning abductor strengthening, core strengthening, and functional training in a non-weight bearing position and progressing to weight bearing as strength and movement patterns improve.
Low Irritability
A patient with low-irritability and a non-contractile presentation will exhibit mild signs of inflammation, however, they may continue to report reproduction of pain with palpation of the greater trochanter and trochanteric bursae. Treatment principles should mirror those described for the low irritability, contractile presentation. Eccentric strengthening of the abductors, high-level core strengthening, and functional training including sport-specific tasks should be prescribed with the goal of returning the patient to their previous level of functioning.
ABNORMAL FRONTAL PLANE MOVEMENT SYSTEM DYSFUCNTION DURING SINGLE LEG TASKS
Development of GTPS is thought to result from faulty mechanics during functional activities, mainly the loss of pelvic control in the frontal place secondary to hip abductor weakness or pain with hip abductor activation.10,11 The GMed and GMin are responsible for maintaining pelvic control in the frontal plane during single leg weight bearing activities and are the tendons most implicated in GTPS.40 From the bottom up, these hip abductors also control the hip adduction moment resulting from the external ground reaction force medial to the hip.41 Any deviation in frontal plane control, due to either pain or weakness, increases the compressive forces of the GMed and GMin tendons on the greater trochanter and trochanteric bursae as well as increases the tension through the iliotibial band. Individuals with GTPS frequently complain of pain and difficulty while completing tasks requiring single leg support as these tasks stress the hip abductors. Given the large role faulty biomechanics plays in the development of GTPS, clinicians must thoroughly evaluate movement patterns through movement system dysfunction assessments. Movement system dysfunction assessments allow for identification of biomechanical deviations during functional activities. In the setting of GTPS, clinicians should evaluate pelvic control during a 30-second SLS, stair ascent, and the stance phase of the gait cycle.
Single Leg Stance
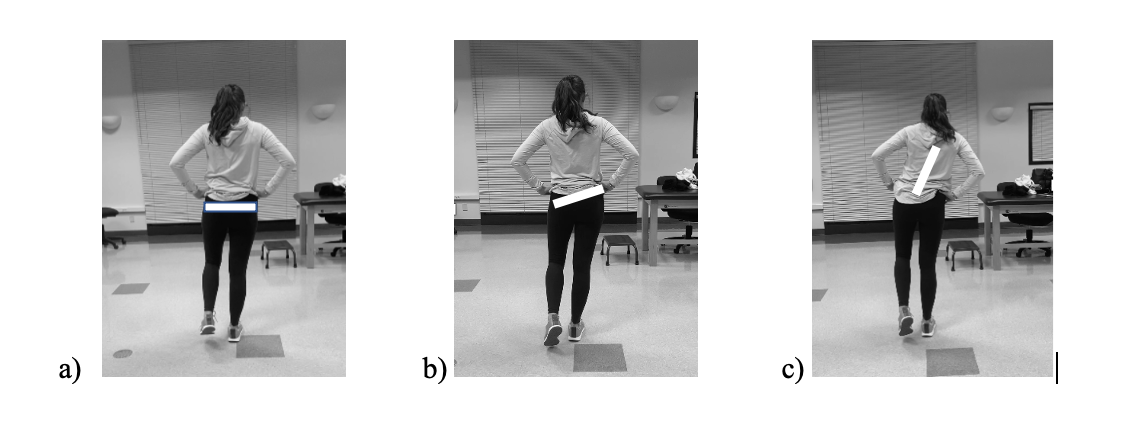
Assessing pelvic control during a 30-second SLS provides information on the function of the GMed and GMin as they are responsible for maintaining a level pelvis during single leg activities.28,40,41 The SLS task should be broken down into the transition phase, going from double to SLS, and the stance phase, when only one foot is on the ground. The transition phase requires hip abductor activation to assist with the lateral translation of the pelvic girdle while stance phase requires the hip abductors to control pelvic tilt.42 In the setting of hip abductor weakness or pain with activation of the hip abductors, an individual may exhibit a Trendelenburg sign, meaning the contralateral hip will drop towards the floor, or a compensated Trendelenburg, meaning the patients trunk leans ipsilaterally to the stance leg (Figure 7).43,44 Allison et al.42 found individuals with gluteal tendinopathy exhibit greater hip adduction and ipsilateral pelvic shift in preparation for leg lift and greater hip adduction and less control over the pelvis during the stance phase. Other signs of hip abductor dysfunction include the need for upper or lower extremity support during the SLS task. To get a complete picture of SLS performance, a contralateral SLS should be assessed to highlight side-to-side differences in pelvic control.
_normal_frontal_plane_mechanics__(b)_a_trendelenburg__and_(c)_a_c.png)
Stair Ascent
The ability to negotiate stairs is critical for maintaining independence and is required to complete many activities of daily living. Compared to walking on level ground, the strength required to negotiate stairs is significantly higher.45–47 Individuals with GTPS frequently complain of pain during stair ascent or the inability to complete the stair task, greatly reducing their quality of life. During stair ascent, the hip abductors are responsible for maintaining a level pelvis as the body moves vertically to reach the next stair.45 When compared to level ground walking, stair ascent requires greater hip flexion, hip adduction, and knee internal rotation moments which in turn increases the tension through the iliotibial band. Additionally, stair ascent requires activation of the tensor fascia lata, gluteus maximus, and the vastus lateralis, all which have attachments to the iliotibial band.48–50 This increase in tension on the iliotibial band leads to even greater compression over the greater trochanter.45,46 Allison et al.51 reported individuals with gluteal tendinopathy were 4.5 times more likely to exhibit a large hip adduction moment and greater pelvic translation at heel strike during stair ascent than healthy controls.51 Additionally, the presence of a contralateral trunk lean was observed in those with gluteal tendinopathy.51 When assessing the movement system during stair assent, clinicians should evaluate the frontal plane mechanics during the stance phase, meaning when the lower extremity being assessed is on the ground. Poor performance of the hip abductors during stair ascent can manifest through a pelvic drop, pelvic translation, and/or trunk lean. The individual may also exhibit a step to gait pattern or excessive use of upper extremity support on a handrail.
Gait
SLS comprises 40% of the gait cycle, potentially aggravating the symptoms of GTPS as there is a higher load through the hip abductor tendons compared to the swing phase.19,30 Compared to healthy controls, those with gluteal tendinopathy were found to have a greater hip adduction moment during the stance phase.52 A Trendelenburg gait pattern, with or without the complaint of pain, may be an indication of gluteal dysfunction. In the case of a mild gait deviation, a 30-second SLS test should also be performed in order to better assess the functional performance and endurance of the abductors. With severe gluteal dysfunction, a compensatory trunk lean to balance out the center of gravity may be observed.53
In order to appropriately tailor treatment interventions, findings of the physical examination and movement assessments should be utilized to appropriately categorize the patient into a contractile or non-contractile presentation. Impairment-based treatment can then be utilized based on irritability to address muscle strength, flexibility deficits, and motor control impairments during functional activities. The goal of treatment is to improve motor patterns to reduce the compression of the gluteal tendons on the trochanteric bursae and greater trochanter and ultimately reduce pain and improve function. A summary of the recommended treatment algorithm for GTPS can be found in Table 2.
CONCLUSION
GTPS is a term utilized to describe pain in the lateral hip and can include external snapping hip (coxa saltans), trochanteric bursitis, and gluteal tearing and tendinopathy.1,2 Individuals suffering from GTPS complain of lateral hip, thigh or buttock pain that worsens with single leg activities and lying on the affected side. Currently, there are no tests or cluster of tests to identify the involved pathoanatomical structure or the severity of dysfunction. Therefore, an impairment-based treatment classification system is recommended, delineating patients into two categories: contractile or non-contractile. Once the patient is categorized into contractile or non-contractile based on physical examination findings and assessments of the movement system, impairment-based treatments can be utilized to appropriately tailor interventions to improve functional outcomes. Treatment of contractile sources of GTPS should focus on muscle and tendon healing through STM and loading exercises whereas treatment of non-contractile sources of GTPS should focus on reducing compressive forces over the greater trochanter and alleviating bursal irritation and overload of the lateral structures of the hip.