

INTRODUCTION
Glenohumeral joint pain is widely prevalent in the general population and exerts a large burden on society.1,2 One reason for the high prevalence of shoulder pathology is related to its anatomical structure. The glenohumeral joint’s osseous anatomy provides little stability3,4 and it is well established that the glenohumeral joint is reliant on muscular support for dynamic stability.4–7 Specifically, the muscles of the rotator cuff (RTC), the supraspinatus, infraspinatus, teres minor, and subscapularis, are vital to collectively compress the humeral head into the glenoid for stabilization.4–9 In order for the RTC muscles to function properly, there must be adequate scapular stabilization,5,6,10,11 which is accomplished by muscular contributions from the periscapular muscles.4,12,13 Deficiencies in periscapular muscle function and scapular motion have been detected in patients with shoulder pathology.5,6,14–21 Therefore, both RTC and periscapular strengthening exercises are established interventions for patients with shoulder pathology.6,11,20,22,23 Since muscular imbalance is a potential cause for shoulder pathology, it has been suggested that exercises should aim to preferentially target the middle trapezius, lower trapezius, and posterior RTC, with lower contributions from the upper trapezius and deltoid muscles.14,16,19,24–26
Commonly performed strengthening exercises targeted at periscapular and RTC muscles include shoulder horizontal abduction27 and diagonal arm movements.6,8,28,29 These exercises are often performed with dumbbell or cable resistance; however, equipment such as dumbbells and a cable column machine may not be readily available for all individuals during home exercise. When these motions are performed with an elastic resistance band, with both hands in horizontal abduction or diagonal arm movements they are often referred to as band pull-apart exercises. Elastic band is an extremely convenient tool for exercise, as it is portable and the patient does not require any additional equipment. Although clinicians are widely aware of the utility of these band pull-apart exercises, no information regarding the extent of shoulder-girdle muscle activity during these exercises is available to guide clinical decision making.
Band pull-apart exercises can be performed with varying degrees of arm rotation. Previous authors have demonstrated that changes in glenohumeral internal and external rotation alter scapular and RTC muscle activity in a number of shoulder exercises utilizing electromyography (EMG).24–26,30–35 These exercises are frequently performed in the prone position,11,30 however, a standing position is more functional, and due to the muscular attachments on the scapula, performing strengthening exercises with hip and trunk extension may be beneficial,6,8 suggesting advantages of the resistance band pull-apart exercise. The effects of movement direction and arm rotation position on shoulder muscle activity during performance of the pull-apart exercise in standing are currently unknown. Therefore, the purpose of this study was to measure the EMG activity of shoulder-girdle muscles during the pull-apart exercise using resistance bands and to determine the effects of arm position and movement direction on shoulder-girdle muscle activity.
METHODS
Participants
A sample of convenience was recruited from the local community. Potential subjects were included if they were healthy at the time of testing and did not have any history of shoulder pathology. Before participation, each subject provided written informed consent in accordance with institutional review board regulations.
Procedures
A 16-channel BTS FREEEMG 300 system, CMRR: >110 dB at 50–60 Hz; input impedance: >10 GΩ (BTS Bioengineering, Milan, Italy) was utilized for EMG data collection during this study.
Previously described anatomical landmarks for surface EMG placement were identified for five muscles of interest: upper trapezius, posterior deltoid, infraspinatus, middle trapezius and lower trapezius.36,37 The subject’s exposed skin was prepared by shaving, cleaning, and lightly abrading. Disposable Ag/AgCl passive dual surface EMG electrodes (2.0 cm interelectrode distance; Noraxon, Scottsdale, AZ) were placed on the identified landmarks on the right shoulder of each subject (Figure 1). Muscle activity was sampled at 1000 Hz.
_upper_trapezius__(c)_posterior_deltoid__(d)_infraspinatus.png)
Once surface electrodes were attached to the subject, a maximum voluntary contraction (MVC) was performed in the previously described manual muscle testing (MMT) position for each muscle.38 A single tester, a board-certified sports physical therapist with over 20 years of clinical experience, provided MMT resistance for all subjects. One trial lasting five seconds was performed for each MMT for each muscle tested. Once peak activity from the MVC trials were calculated, it was verified that the highest peak activity for a muscle occurred during its intended MVC and not during the MVC intended for another muscle.
Subjects then determined which resistance level they would use by performing shoulder horizontal abduction with a neutral grip for five repetitions while holding a resistance band. Resistance level was standardized across subjects to self-reported moderate exertion (5/10 on Borg CR10 Scale).39 As the tension of a resistance band is affected by the amount of elongation, subjects were instructed to hold the band without slack or tension at the beginning of each exercise movement.
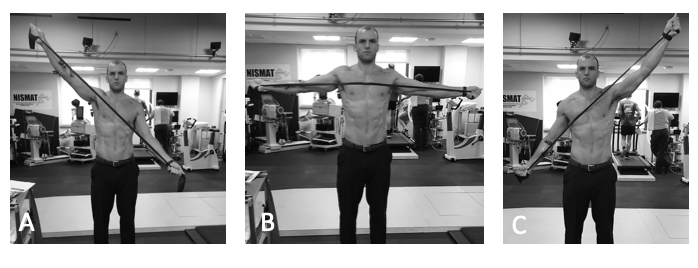
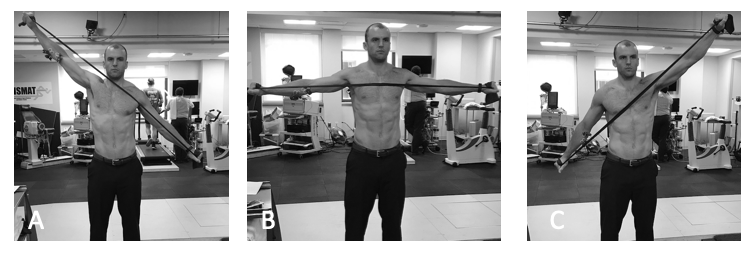
A total of nine exercise conditions existed between the variations of hand position (palm up, neutral, palm down) and movement direction (diagonal up, horizontal, diagonal down) (Figures 2-4). Order of exercise condition was randomized for each subject using a random number generator. Three repetitions of each exercise condition were performed. Pace of movement was standardized to three seconds for each phase of movement (i.e., concentric and eccentric) guided by a metronome set to 20 beats per minute.
_diagonal_up__(b)_horizontal__(c)_diagonal_down__named_by_the_do.png)
_diagonal_up__(b)_horizontal__(c)_diagonal_down.png)
_diagonal_up__(b)_horizontal__(c)_diagonal_down.png)
Data Processing
Electromyographic data were processed and analyzed using previously described methods.40 All EMG data were high-pass filtered at 10 Hz, full-wave rectified and smoothed using an RMS filter with a 100-ms window. For each muscle, the peak EMG activation level was identified during each exercise. The mean activation level of each muscle during a window from 250 milliseconds before the peak to 250 milliseconds after the peak was calculated. This was then averaged over the three repetitions for each exercise and each muscle. This mean peak EMG activity was normalized to the maximum EMG activity recorded during maximal voluntary isometric contraction (MVIC) and expressed as a percent.
Statistical Analysis
Descriptive statistics were calculated for mean normalized peak EMG activity for each muscle and each exercise condition. Shapiro-Wilk test for normal distribution of the data and Mauchly’s test for sphericity were conducted to confirm that assumptions were met for conducting a parametric test for these data. For each muscle, mean normalized peak EMG activity was compared across exercise conditions using two-way (hand position x movement direction) repeated-measures ANOVA. If a significant interaction or main effect was found with the ANOVA, post-hoc simple main effects or pairwise comparisons, respectively, was performed. Where a main effect was found for either hand position or direction, post-hoc pairwise comparisons of marginal means were performed with a Bonferroni correction, in which p values for the pairwise comparisons were adjusted by the number of pairwise comparisons performed per main effect per muscle. Familywise significance level was set at p=0.05. All statistical analyses were performed using IBM SPSS Statistics 25 (IBM Corp, Armonk, NY).
RESULTS
Ten male subjects (age 36 ± 12 years) volunteered to be included in this study. Mean normalized peak muscle activity ranged from 15.3% to 72.6% of MVC across muscles and exercise conditions (Table 1). No significant interaction effect was found between hand position and movement direction on mean normalized peak muscle activity in any of the muscles analyzed (p-value range 0.18-0.85).
There was a significant main effect of hand position on infraspinatus activity (p<0.001), where the palm up position elicited 11.1% higher activity compared to palm down (p=0.029) and 8.7% higher activity compared to neutral position (p=0.031). There was also a significant main effect of movement direction (p=0.011), however, post-hoc pairwise comparisons did not yield any significant differences.
Upper trapezius activity showed a significant main effect of hand position (p=0.004), where the palm down position elicited 6.3% higher activity compared to the neutral position (p=0.036). A significant main effect of movement direction was also found (p<0.001), where the highest activity was in the diagonal up direction (mean difference vs. diagonal down 36.4%, p=0.003; mean difference vs. horizontal 13.5%, p=0.02), followed by horizontal (mean difference vs. diagonal down 23.0%, p=0.005).
Middle trapezius activity was significantly affected by movement direction (p<0.001), where the normalized activity was 31.6% higher in the diagonal up direction (p=0.003) and 27.8% higher in the horizontal direction (p=0.017) compared to the diagonal down direction. Hand position did not have a significant effect on middle trapezius activity.
There was a significant main effect of hand position on lower trapezius activity (p<0.001), where palm up position elicited 13.3% higher activity than palm down position (p=0.001) and 10.4% higher activity than neutral position (p=0.011). Movement direction also had a significant effect on lower trapezius activity, where the highest activity was seen in the diagonal up direction (mean difference vs. diagonal down 34.9%, p=0.003; mean difference vs. horizontal 11.2%, p=0.019), followed by horizontal (mean difference vs. diagonal down 23.7%, p=0.004).
Posterior deltoid activity showed a main effect of hand position (p=0.001), where the palm down position elicited 13.5% higher activity compared to the palm up position (p=0.02) and 8.4% higher activity compared to the neutral position (p=0.002). There was also a significant main effect of movement direction (p=0.02), however, post-hoc pairwise comparisons for the effect of movement direction did not show any significant differences.
DISCUSSION
The principle finding of this research study was that the resistance band pull-apart exercise effectively recruited scapular and RTC muscles, demonstrated by mean peak muscle activity levels of 15% to 73% of MVC. The results also demonstrated that hand position and movement direction had significant effects on scapular and RTC muscle activity.
Horizontal abduction and diagonal movement patterns are common shoulder ans scapular strengthening exercises.6,8,27–29 Additionally, varying glenohumeral rotation has consistently demonstrated the ability to alter muscle activity during arm movements and exercises.24–26,30–35 The current research study adds to this body of evidence by showing that infraspinatus activity can be increased by using the palm up position over the neutral or palm down positions, and upper trapezius, middle trapezius, and lower trapezius activity can be increased by using the diagonal up direction over the horizontal or diagonal down directions. The mean difference in muscle activity between the palm up and palm down positions was 11%, which exceeded previously reported minimally detectable change for surface EMG of infraspinatus (8.2% of MVC).41 Therefore, using the palm up hand position over the palm down position during the pull-apart exercise resulted in a significant and clinically meaningful increase in infraspinatus muscle activity.
There was a significant main effect of movement direction for the infraspinatus, upper trapezius, middle trapezius, lower trapezius, and posterior deltoid. Moreover, the diagonal up direction facilitated significantly higher muscle activity than one or both of the other movement directions for the upper trapezius, middle trapezius, and lower trapezius muscles. The diagonal up movement showing the highest shoulder-girdle muscle activity is understandable as the arm is moving against gravity, resulting in higher overall load when the same level of resistance band is used as the other movement directions.
The ability to facilitate or inhibit muscle activity during the pull-apart exercises by changing hand position and/or movement direction is desirable, as this enables a clinician to adjust and prescribe appropriate exercise load by adjusting these parameters. Exercises targeting shoulder-girdle muscles often aim to minimize upper trapezius and deltoid activity, and to increase lower trapezius and RTC activity for individuals that have shoulder pathology.14,16,19,24–26 Based on the results of this research study, activation of the infraspinatus may be maximized by performing the pull-apart exercise in the palms-up hand position. This information could influence clinical decision making, as it may be useful to utilize the GH ER (palms up) grip during the pull-apart exercises, to selectively maximize the infraspinatus and lower trapezius. Additionally, the findings that RTC and periscapular muscles can be activated to a high degree with a resistance band further demonstrates the convenience of this exercise apparatus.
There is concern about the palm down hand position, especially when combined with the diagonal up movement, as this may put the shoulder in position of glenohumeral internal rotation, which has been shown to decrease subacromial space42 and is considered a risk for pathologic impingement of the RTC.43 Therefore, the palm up hand position during the diagonal up movement may offer the maximal benefit for muscle recruitment while minimizing potential adverse effects of subacromial impingement. In cases where subacromial impingement or selective muscle activation is not of concern, all hand positions and movement angles may be used to maximize activation of all periscapular and rotator cuff muscles.
This research study has several limitations. A sample of convenience was used and only data from healthy male participants were collected. As patients with shoulder symptoms demonstrate alterations in their muscular activity,6,15,16 results of this study may not be generalizable to a patient population. Surface EMG is prone to signal cross-talk from surrounding musculature and surrounding noise. The instrumentation and signal processing procedures used in this study were intended to suppress noise in the data, however, signal cross-talk cannot be completely eliminated with surface EMG. In addition, it was not possible to accurately measure supraspinatus activity via surface EMG due to the overlying upper trapezius muscle and since surface EMG signals are most impacted by motor units closest to the recording electrode.44 This was clearly a limitation of this research study as supraspinatus activity is of strong clinical interest in studying shoulder exercises. Future research could study the supraspinatus using fine-wire EMG. Finally, EMG data do not fully represent force production of the involved muscles, tension across tendons, or the training effects of the exercises. To provide a more robust support for the use of the pull-apart exercises, future studies are needed to show training effects and clinical outcomes in patients with shoulder pathology.
CONCLUSION
The findings of the current study suggest that movement direction and hand position may alter level of muscle activity in the RTC and scapular muscles. The diagonal up movement demonstrated the highest levels of muscular activity for the upper trapezius, middle trapezius, and lower trapezius muscles. Additionally, the palm up hand position demonstrated increased levels of activation of the infraspinatus and lower trapezius, and decreased activity of the upper trapezius and posterior deltoid. Thus, the diagonal up motion, with the palm up hand position, may be most beneficial to maximize desirable levels of RTC and scapular muscle activation during the pull-apart exercise.
Conflicts of Interest
The authors report no conflicts of interest related to this manuscript.