
INTRODUCTION
There are 80,000-250,000 anterior cruciate ligament (ACL) injuries per year, 70% of which are non-contact injures.1 Of all knee ligament injuries involving surgery in a five-year epidemiological study, 80% involved the ACL and 65% of the ACL injuries requiring surgery were the result of a sport/recreational incident.2 ACL injuries also bear a heavy economic and social burden with the cost of an ACL injury estimated at $38,121 in a lifetime, and $7.6 billion dollars across the US annually.3 Likewise, conservative treatment can cost an individual $88,583 throughout their life and $17.7 billion in the US annually.3 Also, there is a high risk for development of osteoarthritis following an ACL injury, which leads to added expenses for treatment and interventions.3 Along with direct expenses, ACL injury can have a major indirect cost to society including decreased productivity, disability, and lost wages3 and the average time off for an acute reconstruction is 56.9 days and 88.5 days for a delayed reconstruction.4
There are various reports on the incidence of ACL injuries in males and females. When observing the general population, males constitute the majority of ACL injuries but this has been attributed to males being more likely to participate in athletic tasks known to injure the ACL such as cutting, jumping and contact sports as compared to females.2 When examining ACL injuries in the perspective of the athletic population, there is a strong agreement that females are at higher risk4 with numerous studies reporting that females have approximately three to nine times greater risk of injury than males.5 Hootman et al.6 evaluated sports injuries occurring in 15 NCAA sports over a 16 year period and found 5,000 of 182,000 were ACL injuries, or 2.7%. According to their study, the three sports with the highest incidence for ACL injury were women’s’ sports, including gymnastics, soccer, and basketball.6
There are several anatomical and biomechanical risk factors associated with ACL injuries. Anatomically, a decrease in femoral notch width, a decrease in concavity depth of the medial tibial plateau, an increase in posterior-inferior-directed slope of tibial plateau, and generalized joint laxity have been noted in persons who have sustained an ACL injury.7 Biomechanically, decreased knee flexion, increased knee valgus, tibial rotation, hip adduction, and hip internal rotation during landing and/or cutting maneuvers are frequently observed during ACL injury episodes.7 Collectively, these movements are termed “dynamic knee valgus.”7 This dynamic knee valgus, along with the anatomical risk factors, is more frequently demonstrated in women and may help explain why there is a much higher rate of ACL injuries in women as compared to men.7 Compared to female soccer players, female basketball players typically have more body mass, are taller, and demonstrate larger ground reaction forces with jumping and landing activities –all of which are factors that increase the risk of an ACL injury.8,9
With an initial ACL injury comes an increased risk for re-injury of the ligament. It is reported that up to 33% of individuals who previously suffered an ACL injury sustained a second ACL injury within two years following ACL reconstruction.10 Although a second ACL tear is less common than an initial rupture, young athletes who return to sport following an initial ACL injury are at approximately 30 to 40 times greater risk of sustaining an ACL injury during sport compared to those who have not had a previous ACL injury.11 Second ACL tears can occur due to graft failure and contralateral ACL rupture, and the risk factors for these tears include young age, sex, and return to sport.10–12 Inadequate rehabilitation and participation in high-risk sports such as soccer, basketball, football, or skiing are some factors that may lead to graft failure or contralateral ACL injury.11 It is reported that 29.5% of athletes suffered a second ACL injury within two years of return to sport, with 20.5% tearing the intact contralateral ACL and 9.0% rupturing the ACL graft.10
Increased dynamic knee valgus motion during the impact phase of jumping and cutting tasks are key predictors for ACL injuries.13 Dynamic knee valgus is a combined movement of the lower extremity during an activity which includes hip adduction and internal rotation, knee abduction and tibia internal rotation14 or the medial displacement of the knee.15 Therefore, biomechanical pre-injury screenings can be performed to identify individuals who may be at risk for ACL injuries. Currently, one of the most common screening tools is assessing lower extremity mechanics during the drop vertical jump (DVJ) assessment, which requires a high level of dynamic neuromuscular control.13 While the DVJ test demonstrates high reliability (ICC greater than 0.93), this movement doesn’t accurately represent the more common mechanisms of injury for ACL tears—which includes cutting, landing and/or pivoting in the frontal plane.13
Another common screening test is the single leg (SL) squat assessment. This activity objectively shows changes in lower extremity alignment in athletes as they progress toward return to jumping or cutting sports.16 The amount of dynamic knee valgus displayed during a SL squat is reflective of the individual’s associated hip strength and neuromuscular control. Although the SL squat test may identify hip weakness that predisposes an athlete to an ACL injury,16 the SL squat does adequately mimic jumping or cutting as seen in high-risk sports such as basketball and soccer where the majority of ACL injures occur during landing and change of direction movements, respectively.8 For this reason, there needs to be a stronger emphasis on a frontal plane dynamic activity, rather than the DVJ and SL squat, to effectively screen athletes for potential ACL injury.
During return to sport decision-making there are several different factors that need to be assessed—such as range of motion, strength, pain, self-reported questionnaires and functional performance.17 Currently, functional tests commonly used include the single leg hop, triple hop, crossover hop and 6-m hop for time.17 With all functional performance tests, the examiner is observing quality of movement, signs of patient apprehension, and most importantly limb symmetry. While these tests should be included in a return to sport assessment, the evidence on their ability to accurately indicate if the athlete is able to return safely is lacking.17 Furthermore, the functional tests listed only assess movement in the frontal plane. Therefore, there is a need for dynamic tests which assess neuromuscular control in the frontal plane which may assist in determining if an athlete is ready to return to sport with minimal risk of re-injury.
One functional test that does utilize frontal plane movements is the medial and lateral triple hop test for distance. This test is used for both ACL prevention and return to sport assessment in athletes and mimics the original triple hop test, but hopping is performed in the frontal plane rather than the sagittal.8,18 The most limiting aspect of this test, however, is that a single-leg hop is rarely a movement performed in sport. Basketball players specifically, are more involved in movement such as lateral shuffling and cutting.8 While these motions do require single-leg movement, they involve transition of single leg stance on one leg to single leg stance on the contralateral leg, unlike hopping.19
ACL injuries are a growing issue, as they occur commonly in the athletic population and the consequences can be both costly and timely. A test is needed which incorporates dynamic movement in a frontal plane functionally similar to shuffling and cutting. Therefore, the purpose of this study was to determine the reliability of and examine differences between sexes in the performance of the Lateral Bound Test (LBT). It was hypothesized that the LBT will be reliable and females will demonstrate increased dynamic knee valgus and decreased knee flexion at both initial contact and maximal depth.
METHODS
Participants
Thirty subjects, healthy, non-athletes were recruited. Participants were excluded if they participated in any sport at the collegiate level or if they had sustained an injury in the prior three months that required medical attention and/or resulted in a decrease in activity for greater than three days. Informed verbal and written consent as well as participant demographics and injury history were taken prior to testing. This study was approved by the University of South Alabama’s Institutional Review Board.
Procedure
The participants performed a five-minute warm-up which included walking or jogging at their own preferred pace. Markers were then placed at the greater trochanter, lateral joint line of the knee, lateral malleolus, the anterior thigh midway between the anterior superior iliac spine (ASIS) and mid patella, anterior joint line of the knee and at the anterior ankle between the tibia and fibula. To normalize bounding distance, each participant’s leg length was measured using the distance between the ASIS and the medial malleolus. Then a target "X’ was place on the landing surface which was a force plate, however, kinetics were not assessed in this study. Static knee valgus posture was assessed by having the participant stand on a single leg before they performed the LBT. The participant was then instructed to jump from the starting position on one leg, over a 10-inch (25.4 cm) hurdle which was placed approximately 2 to 6 inches (5.08 to 15.2 cm) from the starting leg and land on the target with the opposite leg. The target was placed laterally of the starting leg to limit movement in the anterior and posterior directions and a hurdle was used to ensure the participant attained a significant amount of vertical movement. Two practice trials and three testing trials were performed for each leg with the landing leg being considered the tested leg. Rather than classifying limb as right or left, dominant/non-dominant extremity was used with the dominant lower extremity determined by the extremity selected by the participant when asked “what leg they would select to kick a soccer ball as hard as they could.”
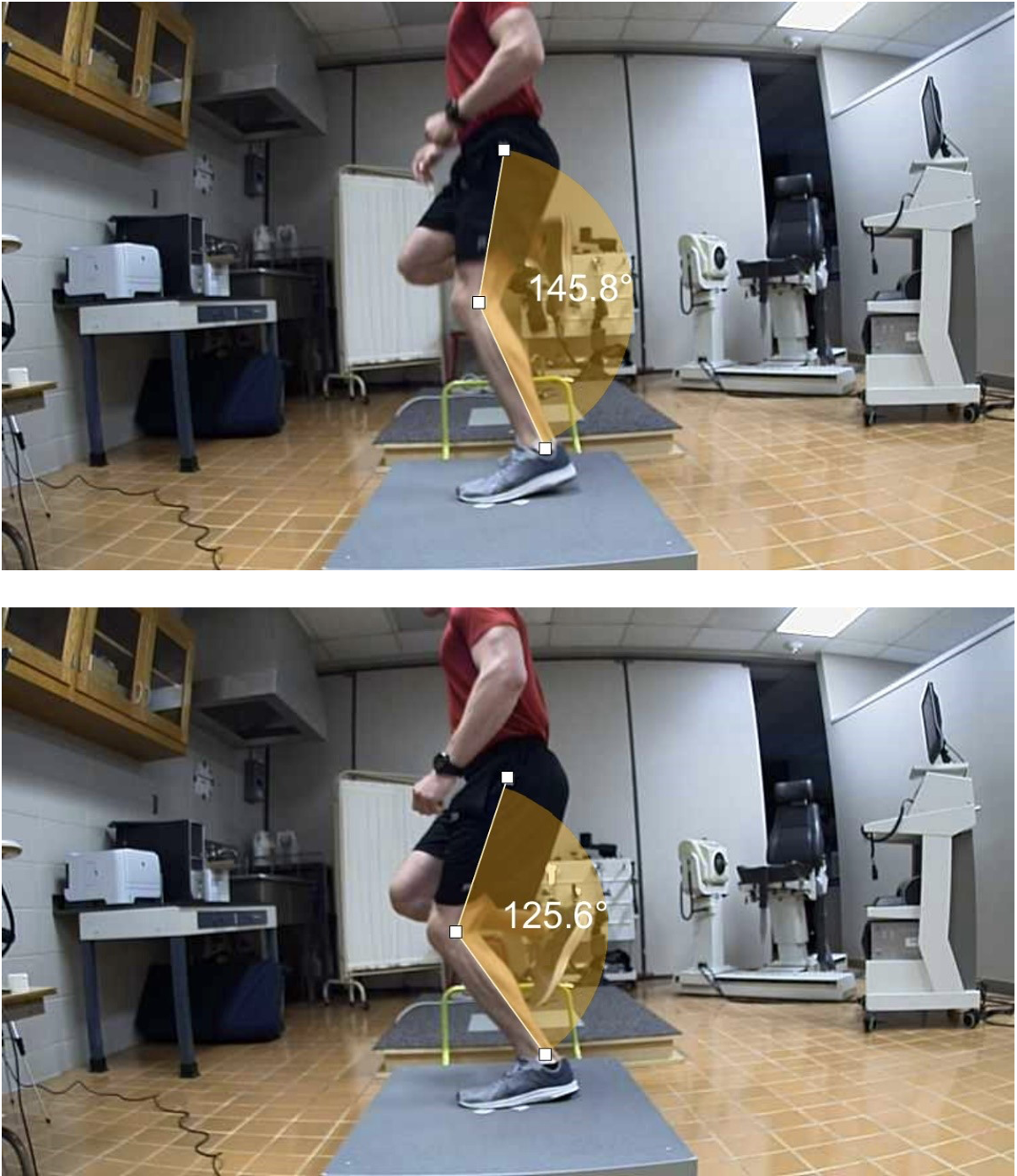
The average of the three trials was used for data analysis. Two 60 Hz video cameras, one anterior and one lateral of the participant, were placed 6 ft (1.82 m) from the landing target at a height of 18 inches (45.7 cm) from the ground. The camera placed lateral to the participant camera was used to assess initial and maximum knee flexion angle during the landing, while the camera placed anterior to the participant was used to assess knee valgus angle. Video software (Dartfish Motion Analysis Software) was used to determine initial (Figure 1a) and maximum knee flexion angle (Figure 1b) and dynamic knee valgus via the Frontal Plane Projection Angle (FPPA) (Figure 2). For true dynamic knee valgus, the static FPPA was subtracted from the FPPA obtained during landing from the lateral bound. Only knee kinematics were used in this study to minimize time needed for data processing, therefore results could be obtained quickly in a clinical setting. Twelve of the participants were randomly selected and asked to return for a retest a week after of the initial trial. One trial for ten participants were randomly selected for intra-rater reliability with the primary investigator performing video analysis on two occasions, seven days apart.


Statistical Analysis
To determine the intra-rater and test-retest reliability of the Lateral Bound Test, Intraclass Correlation Coefficients (ICC) were performed while independent t-tests were used to compare differences between sexes in dynamic knee valgus and knee flexion angles. A p-value of 0.05 was used for all statistical analyses.
RESULTS
Sixteen males and 14 females above the age of 18 participated in this study (males 23.6 ± 1.58, females 22.9 ± 1.22 years of age). Descriptive statistics from both sessions and all participants were used to determine intra-rater and test-retest reliability for each of the six variables as well as ICC values (Table 1). Intra-rater reliability was determined to be excellent for all variables with ICC values all greater than 0.96. In contrast, the test-retest reliability had greater disparity. Dominant knee flexion at initial contact exhibited poor reliability (ICC = 0.47), two measurements had fair reliability, maximum non-dominant knee valgus (ICC = 0.74 and ICC = 0.71, respectively), maximum non-dominant knee flexion, (ICC = 0.88) was found to have good reliability and two tests, maximum dominant knee valgus (ICC = 0.92) and maximum dominant knee flexion (ICC = 0.90) were shown to have excellent reliability.
Means and standard deviations as well as sex-related differences are displayed in Table 2. Significant differences between sexes were noted for height, weight and bilateral maximum dynamic knee valgus. Males were significantly taller, weighed more, and exhibited greater dynamic knee valgus on both the dominant and non-dominant lower extremity upon landing from the lateral bound, while on average females landed with a slightly knee varus posture on both extremities. There were no significant differences with the degrees of knee flexion on initial contact or maximum knee flexion on either leg when comparing between sexes.
DISCUSSION
The purpose of this study was to determine the reliability and differences in performance between sexes of a new test, the LBT, which assesses the quality of landing mechanics in the frontal plane. The hypothesis was partially supported by the results as the lateral bound test was found to be reliable but sex differences in landing mechanics were not accurately predicted. The lateral bound test was found to have excellent intra-rater reliability, but test-retest reliability ranged from poor to excellent. Males surprisingly displayed significantly greater landing knee valgus than females although the difference may not be clinically relevant since the findings were less than 4˚.
Compared to other studies of similar tests, the LBT had better intra-rater reliability statistics in the current research. McKeown et al. reported moderate intra-rater reliability when screening with a similar test where female semi-professional football players performed a maximum lateral bound and a qualitative scoring system was used to assess performance.20 These lower reliability measures could be due to the subjectivity of their study, as the scoring criteria relied on categorical observations opposed to objective numerical data. Hip/knee/ankle alignment, depth, balance/control, and power positioning in landing were assessed and scored from one to three - one being poor execution of the task and three being perfect execution of the task.20
There are several other studies on examining the reliability of functional screens with similar results. Herrington et al. reported good intra-rater reliability when performing 2D assessment of dynamic knee valgus during a single leg squat screen and a single leg hop landing screen on active and healthy individuals.21 Redler et al. assessed ACL injury risk in young athletes via the drop vertical jump based on normalized knee separation distance, reporting it to have moderate reliability.1 The LBT demonstrated excellent intra-rater reliability most likely due to the highly objective nature of the study as well as the rater’s experience with the software.
Several other studies examined the test-retest reliability of other functional screens and they had comparable results when assessing dynamic knee valgus angles.21,22 Herrington et al. reported the single leg squat and single leg hop screening tests to have good reliability (ICC= 0.79-0.87) between sessions as well.21 Werner et al. demonstrated good to excellent test-retest reliability when assessing frontal plane projection angles during the single leg squat (ICC=0.84), single leg hop (ICC=0.82), and drop jump (ICC=0.96) using 2D video analysis.22 It is possible that some of these tests demonstrated a greater test-retest reliability due to the fact that the components of the tests, such as single leg squat, were movements with which the subjects were more familiar, or had more practice performing since they may be included in an exercise program.
While the intra-rater reliability of this test was found to be excellent, due to high variability within subjects, the test-retest reliability for some measurements were less consistent. This may be due to participants not landing on the target for every attempt which may be due to many factors such as length of the target or poor athletic performance since the participants were not competitive athletes. The researchers in the current study observed that when a subject landed past the target, they exhibited increased knee valgus. This could have contributed to the participant having difficulty controlling their pelvis and having excessive lateral movement when landing past the target. Furthermore, the average knee valgus (FPPA) decreased in in session two, indicating that there may have been a learning effect in which the subjects became more familiar with the task and were able to improve their landing mechanics in session two by concentrating more on the mechanics.
As expected, there were significant differences by sex noted for height and weight. Males landed with more dynamic knee valgus (bilaterally) which is not a common finding in functional screens performed in the sagittal plane. In a study using the drop vertical jump, female high school basketball players demonstrated significantly increased dynamic knee valgus as compared to males.23 Furthermore, females demonstrate greater knee valgus angles during a single leg squat test, as well as higher rectus femoris muscle activation, both of which can add to the stress on the ACL during jumping, landing, and cutting activities.24 Pappas et al. reported that regardless of bilateral or unilateral landings, females tend to land with greater knee valgus as compared to males.25 Since females often display greater quadriceps activation during jumping and landing activities in the sagittal plane, this greater quadriceps activation may increase knee stability and actually be beneficial in controlling knee valgus motion while performing the LBT in the frontal plane.24,26 Therefore, males potentially have greater control on knee dynamic valgus in the sagittal plane with an increase in proximal hip stabilizing muscle activation, whereas females have greater control in the frontal plane with an increase in quadriceps muscle activation.24,26 Another explanation is that in the current study the initial static knee valgus measurement was subtracted from the maximum knee valgus measurement in order to determine the participants dynamic knee valgus during landing during the LBT The greater dynamic knee valgus shown by males, as compared to other studies, could be reflective of other studies not taking account of an initial static knee valgus measurement to determine the amount of knee valgus displayed dynamically during landings.
One limitation of this study was the inability to analyze inter-rater reliability as there was only one person who was trained to perform the video analysis. A second limitation was the inability to move the hurdle, therefore, shorter subjects were closer to the hurdle than taller subjects, but all participants stated they were able to perform the bound comfortably and aberrant techniques were not observed. The height of the hurdle remained constant and was not standardized to the height of each participant making it another limitation to the study. Having an adjustable hurdle and a more dynamic testing location would allow for standardization of the hurdle height and location in reference to the participant. Finally, the cameras used to record the trials captured 60 frames per second. However, a camera capable of capturing greater number of frames per second could have allowed the recording of more accurate measurements, specifically at knee flexion during initial contact.
Future studies of the LBT should include comparisons of athletes and non-athletes, athletes of different sports, athletes of different competitive levels, and athletes with and without previous lower extremity injury such as those recovering from ACL reconstruction. These future studies would help provide normative data and determine if the LBT could be used as a predictor of lower extremity injury or as a return to sport assessment. Last, different landing lengths, shorter and greater than the leg length or maximal distance bounded should be examined in order to determine if using the participants’ leg length is truly the best distance to observe dynamic knee control in the LBT. This this may be more specific to athletes where bounding the distance of their leg length may not be challenging enough to identify impaired landing mechanics.
CONCLUSION
The results of this study indicate that the LBT has excellent intra-rater reliability and varying test-retest reliability when used in healthy non-athletes. Additional research should be performed to determine validity. Unlike other tests assessing dynamic knee valgus in the sagittal plane, the current results indicate that males had statistically greater dynamic knee valgus compared to females during landing and no statistically significant difference in knee flexion angles.
Conflict of Interest
All authors declare no conflict of interest related to this manuscript.