INTRODUCTION
Quadriceps strength and mass deficits are common after anterior cruciate ligament (ACL) reconstruction.1–6 Approximately 30% of patients have quadriceps strength deficits 12 months after ACL surgery.1,3 Quadriceps mass deficits can be as high as 30% and can persist for many years after ACL reconstruction.5 Furthermore, quadriceps mass deficits can negatively affect quadriceps strength.7–9 This is of importance as quadriceps strength after ACL reconstruction is associated with patient reported outcome measurements, functional performance, return to sport and ACL re-injury.1,10–16 Therefore, interventions to address quadriceps strength and mass deficits after ACL reconstruction are imperative.
Heavy load resistance (HLR) training using external loads >60% of one repetition maximum (1RM) is recommended to increase quadriceps strength and mass.17 However, after ACL reconstruction, training with external loads >60% 1RM can have detrimental effects on knee joint pain and ACL graft laxity.18–23 Therefore, low-load blood flow restriction (LL-BFR) training using external loads of 20-40% 1RM has been suggested as an alternative to traditional strength rehabilitation.24,25 During LL-BFR training, a pressurized cuff is applied to the proximal thigh that occludes venous outflow while maintaining arterial inflow.24,25 The combination of venous occlusion and resistance training is believed to induce muscle hypertrophy secondary to elevated systematic hormone production, cell swelling, production of reactive oxygen species, intramuscular anabolic signaling and fast-twitch fiber recruitment.25–27
A recent systematic review showed promising results of LL-BFR training on quadriceps mass after ACL reconstruction.28 As LL-BFR training is an increasingly popular method for the rehabilitation after an ACL reconstruction, it is important to evaluate the value of this treatment.24,25 Therefore, the present systematic review aimed to investigate the effect of LL-BFR training on quadriceps strength, quadriceps mass, knee joint pain and ACL graft laxity after ACL reconstruction compared to non-BFR training.
MATERIALS AND METHODS
The review protocol was registered on PROSPERO (CRD42020163467) and was performed according to the Preferred Reporting Items for Systematic Reviews and Meta-analysis guidelines.29
Search strategy and study selection
A systematic literature search in PubMed, EMBASE.com, Cochrane Library/Wiley, CINAHL/Ebsco and Web of Science/Clarivate Analytics was performed on 19 February 2021 (BK, MH). The following search terms, including all synonyms, were used to search in all databases as index term and as free-text words: blood flow restriction and anterior cruciate ligament (See Appendix 1 for the detailed search strategy). The results of the literature search were collected in the reference management program RefWorks and were de-duplicated.30 Studies were included if they compared LL-BFR and non-BFR training after ACL reconstruction with pre- and post-intervention quadriceps strength or quadriceps mass or knee joint pain or ACL graft laxity measurement. Non-BFR training was defined as strength training without vascular restriction. The exclusion criteria were: systematic reviews, editorials, case reports and studies not published in a scientific, peer reviewed journal. Two reviewers (BK and AT) separately and independently screened all titles and abstracts. The full text was reviewed if title and abstract suggested a study of interest. In case of disagreement, consensus was achieved by a third researcher (MS). In addition, trial reference lists of included studies were screened for relevant articles.
Data extraction
Data of included articles were extracted with the use of RevMan 5.4 (Review Manager 5.4, The Cochrane Centre Collaboration, Copenhagen, Denmark, 2020) including: year of publication, study design, number of patients, study arms, graft used for ACL reconstruction, patient characteristics, LL-BFR training protocol, non-BFR training protocol, and quadriceps strength, quadriceps mass, knee joint pain, and ACL graft laxity measurements.31 When raw data of outcome measurements were not available, the authors were contacted to provide raw data.
Study quality and reporting
The independent reviewers (BK and AT) assessed the risk of bias of the included studies with the use of the Cochrane Risk of Bias Tool. Non-randomized studies were assessed with the ROBINS-I checklist.32 The included studies were evaluated on: selection bias, performance bias, detection bias, attrition bias, reporting bias and other bias.
Data synthesis
Outcome measurements were extracted with the use of RevMan 5.4.31 The difference in pre- and post-intervention mean and standard deviation (SD) was used to calculate the standardized mean difference (SMD). In case SD was not available, this was estimated in accordance with recommendations provided by Cochrane Handbook for Systematic Reviews.33 Data were pooled for a meta-analysis if the included studies were clinically, methodologically and statistically homogenous. In case of considerable heterogeneity (I2 >75%) of the study results, a qualitative analysis was performed.34 The level of statistical significance was set at p≤0.05.
RESULTS
Study selection and characteristics
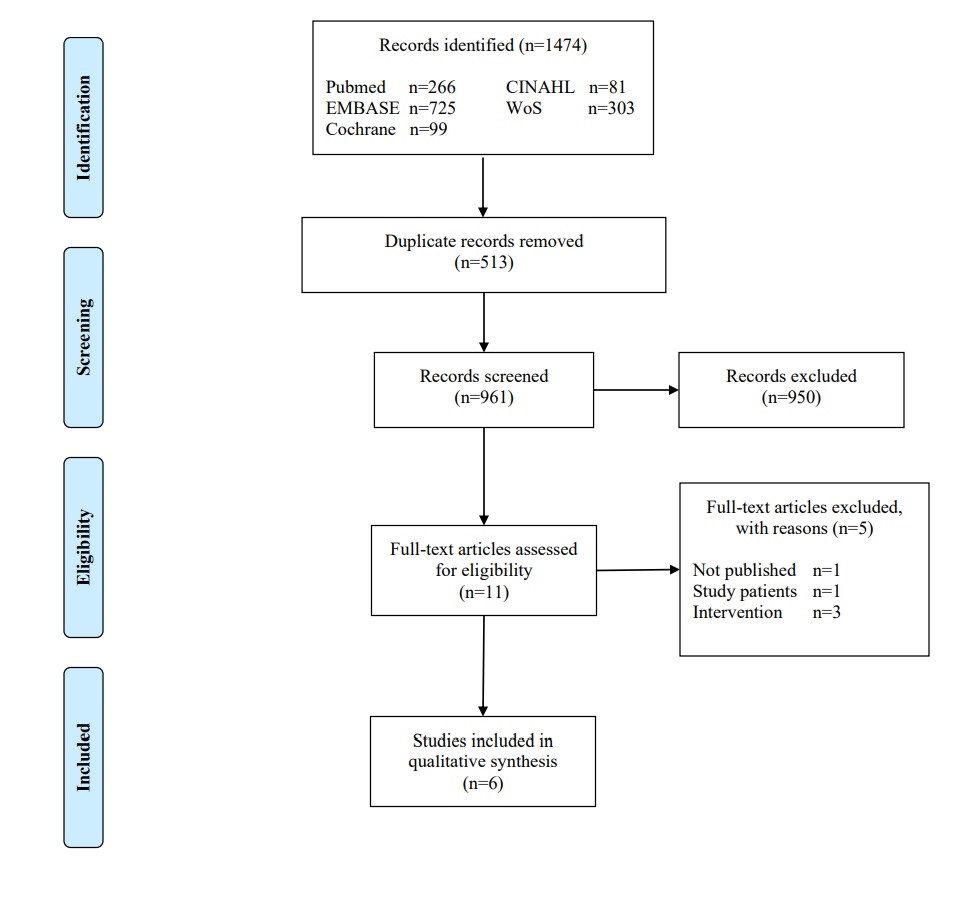
The database search yielded 1474 articles. After initial title and abstract screening, 11 articles were assessed for eligibility. The remaining 11 articles were fully read and six articles met the inclusion criteria. The two independent reviewers agreed on selection of eligible studies and achieved consensus on which studies to include. No additional studies were identified through reference list screening. Therefore, six articles were included in the systematic review (Figure 1). Table 1 shows an overview of the study characteristics.

Three studies were conducted in the United Kingdom, two in Japan and one in Norway.18,35–39 The studies conducted in the United Kingdom are three reports from the same study.18,35,36 However, the three reports from the same study described different outcome measurements, thus, were included in this review. The included studies involved a total of 152 patients who had been randomized into LL-BFR (n=76) or non-BFR (n=76) group.18,35–39 Sample sizes ranged between 16 and 44 patients.18,35–39 Five studies used hamstring graft for ACL reconstruction, whereas one study did not report type of graft.18,35–39 Patient characteristics were not statistically significant different between the LL-BFR and non-BFR group. Table 2 shows an overview of the patient characteristics.
LL-BFR and non-BFR protocols
The intervention protocols are shown in Table 3. The duration of the intervention varied from 11 days up to 14 weeks and training sessions varied from two sessions/week up to two sessions/day.18,35–39 LL-BFR training was used in combination with low-load leg press, leg extension or straight leg raise exercises.18,35–39 The external load varied from body weight up to 30% 1RM and was not specified in two studies.18,35–39 Automatic personalized tourniquet systems and pneumatic cuffs were used during LL-BFR training.18,35–39 The occlusion pressure ranged between 148 and 238 mmHg, while cuff width ranged from 9 to 14 cm.18,35–39 In three studies LL-BFR pressure was defined as 80% of the limb occlusion pressure (ranged from 140 to 160 mmHg), whereas the occlusion pressure was based on previous research in three studies (ranged from 180 to 240mmHg).18,35–39 LL-BFR was intermittently applied with reperfusion periods ranging from 30 to 180 seconds.18,35,36,38,39 In three studies, non-BFR training consisted of the same exercise protocol as LL-BFR training but without vascular restriction.37–39 Hughes et al. used different exercise protocols in the non-BFR and LL-BFR group.18,35,36 In the non-BFR group, the patients performed three sets of 10 repetitions using external loads of 70% 1RM. In the LL-BFR group, the patients performed four sets (30-15-15-15) using external loads of 30% 1RM.18,35,36
Risk of bias
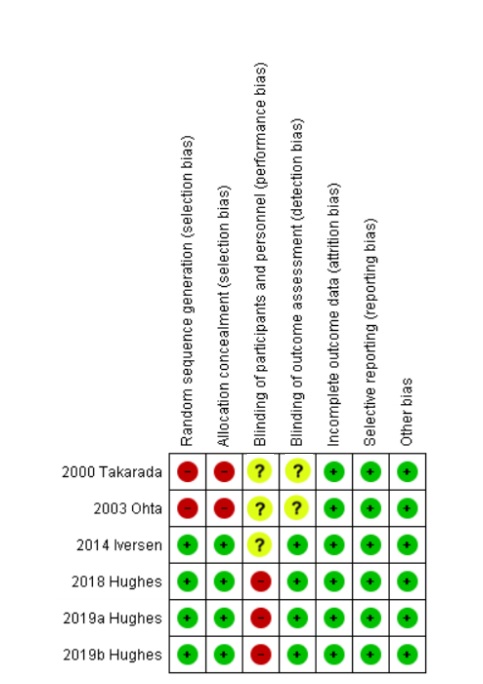
An overview of the quality assessment of the included studies is reported in Figure 2. Random sequence generation and allocation concealment was defined as high risk for bias in two of the six studies. In all studies blinding of participants and personnel was unclear or could not be performed.

Heterogeneity
Comorbidities and concomitant injuries of study participants were not defined in the included studies. Furthermore, different LL-BFR and non-BFR protocols with heterogeneous outcome measurements were used. Therefore, only a qualitative analysis was performed.
Outcome measurements
Quadriceps strength
Quadriceps strength was evaluated in two studies by measuring RM, isokinetic contraction at 60°/seconds, isokinetic contraction at 150°/seconds, isokinetic contraction at 180°/seconds, isokinetic contraction at 300°/seconds or isometric contraction at 60° knee flexion.35,37 Quadriceps strength was measured pre-operatively and at nine up to 16 weeks postoperatively.35,37 Ohta et al. showed significantly less strength deficits in isokinetic knee extension at 60°/seconds (p<0.001), isokinetic knee extension at 180°/seconds (p=0.004) and isometric contraction at 60° knee flexion (p<0.001) after LL-BFR compared to non-BFR training.37 Hughes et al. reported significantly less strength deficits in isokinetic knee extension at 150° and 300°/seconds after LL-BFR compared to non-BFR training (p=0.010).35 However, no significant differences in RM (p=0.220) and isokinetic knee extension at 60°/seconds (p=0.200) were observed between LL-BFR and non-BFR training.35
Quadriceps mass
Three studies used MRI to measure changes in quadriceps cross-sectional area (CSA), while one study used ultrasound to measure changes in vastus lateralis muscle thickness.35,37–39 Quadriceps mass was measured pre-operatively and 14 days up to 16 weeks postoperatively.35,37–39 Takarada et al. showed significant less reduction in quadriceps CSA after LL-BFR compared to non-BFR training (p=0.046).38 Ohta et. al reported a significant increase in quadriceps CSA after 14 weeks LL-BFR compared to non-BFR training (p=0.040).37 Iversen et al. concluded that there was no significant difference in quadriceps CSA between LL-BFR and non-BFR training (p=0.626).39 Hughes et al. used ultrasound to assess changes in vastus lateralis muscle thickness and demonstrated no significant difference in quadriceps increase between LL-BFR and non-BFR training (p=0.230).35
Knee joint pain
Knee joint pain was assessed using a numerical rating scale in two studies, while one study used the Knee Injury and Osteoarthritis Outcome Score (KOOS) pain score.18,35,36 Knee joint pain was evaluated following each session, 24h post-exercise or 10 weeks postoperatively.18,35,36 Two studies observed significant lower knee joint pain scores in LL-BFR compared to non-BFR training.18,36 Furthermore, one study showed significant greater increase in KOOS pain score after LL-BFR compared to non-BFR training.35
ACL graft laxity
Two studies used a knee ligament arthrometer to measure changes in ACL graft laxity.35,37 ACL graft laxity was measured pre-operatively and at 10 up to 16 weeks postoperatively. No significant difference in ACL graft laxity was observed between LL-BFR and non-BFR.35,37
DISCUSSION
The most important finding of the present systematic review was that low-load blood flow restriction (LL-BFR) training after anterior cruciate ligament (ACL) reconstruction may be beneficial on quadriceps strength and quadriceps mass compared to non-BFR training. Furthermore, LL-BFR training may decrease knee joint pain compared to non-BFR training with similar effects on ACL graft laxity. Thus, the present systematic review suggests that LL-BFR training may be an effective alternative to non-BFR training after an ACL reconstruction.
Regarding quadriceps strength, Ohta et al. showed less quadriceps strength deficits after LL-BFR compared to non-BFR training.37 In addition, Hughes et al. demonstrated similar and greater effects on quadriceps strength after LL-BFR compared to non-BFR training.35 Ohta. at al used low-load resistance training (LLR) training as non-BFR training, while Hughes et al. used heavy-load resistance training (HLR) training as non-BFR training. Therefore, the findings of the present review are consistent with current literature comparing LL-BFR training to LLR and HLR training in healthy and postoperative patients.40–46
In regard to quadriceps mass, two studies demonstrated that LL-BFR training was more beneficial on quadriceps cross-sectional area (CSA) compared to non-BFR training.37,38 In contrast, Iversen et al. observed no difference in quadriceps CSA between LL-BFR and non-BFR training.39 The authors acknowledged that subtherapeutic training (e.g. training duration of 12 days) and LL-BFR application (e.g. no personalized BFR pressures) were possible reasons for this difference.39 Current evidence recommends training durations of 6-12 weeks and the use of personalized LL-BFR pressures (80% of limb occlusion pressure [LOP]) to achieve muscle strength and hypertrophy.23–25 In contrast to the previous studies, the non-BFR group of Hughes et al. did not consist of LLR but HLR training.35 In their study, ultrasound was used to examine vastus lateralis muscle thickness and no difference in muscle thickness was observed between LL-BFR and non-BFR training groups.35 Thus, the results of the present review are consistent with literature showing that LL-BFR training may be beneficial on quadriceps mass compared to LLR training and equally effective when compared to HLR training in healthy and postoperative patients.40–46
The application of LL-BFR has generally been indicated for the elderly or injured/postoperative patients who cannot tolerate high external loads.43,47–50 This review adds evidence on the application of LL-BFR as three studies assessing pain observed improved pain relief with LL-BFR compared to non-BFR training in patients following ACL surgery.18,35,36 This is in contrast with a recent systematic review that observed no significant difference in pain relief between LL-BFR and non-BFR training in individuals with knee joint pain.51 The study participants were heterogeneous and included individuals with patellofemoral pain, risk of symptomatic knee osteoarthritis, anterior knee pain and post knee arthroscopy.51 Furthermore, the heterogeneity in LL-BFR pressures and cuff width could explain the lack of effect on knee joint pain.51 Current evidence suggests that therapeutic restriction (defined as 80% of LOP) is achieved at lower LL-BFR pressures with wide compared to narrow cuffs.52–56 Furthermore, lower LL-BFR pressures are associated with less discomfort and greater safety.52–56 Thus, the use of non-personalized pressures without calculating the LOP may cause pain.52–56 In the present systematic review, all studies on knee joint pain used wide cuffs with an automatic personalized tourniquet system to calculate the LOP.18,35,36 Furthermore, all studies used HLR training as non-BFR training. Thus, pain relief may be the result of low external loads and hypoalgesia effects of LL-BFR training compared to HLR training.47,48,57,58
A major challenge in the rehabilitation after an ACL reconstruction is optimizing muscle strength while minimizing mechanical stress to the knee joint.59–61 The importance is represented by the remodeling process of the ACL graft. The remodeling process consists of three phases and the restructuring towards the properties of an intact (non-injured) ACL takes more than six months after reconstruction.21,62 Thereby, accelerated rehabilitation protocols and high load resistance training may compromise graft remodeling and may result in increased ACL graft laxity.19–21,63 BFR training in combination with low external loads has the advantage of minimizing mechanical stress to the knee joint compared to HLR training.47,48 However, in the present systematic review only two studies evaluated ACL graft laxity and showed no significant difference on ACL graft laxity with LL-BFR compared to non-BFR training.35,37 Therefore, more randomized controlled trials are needed to evaluate the effect of LL-BFR training on ACL graft laxity compared to HLR training.
The present systematic review has several limitations. First of all, due to the heterogeneity in intervention protocols and outcome measurements no meta-analysis could be performed. Secondly, differences in LL-BFR and non-BFR protocols affect the results of the present systematic review. Three studies compared LL-BFR training to HLR training, while three other studies compared LL-BFR training to LLR training.18,35–39 Furthermore, three of the six studies used LL-BFR protocols as recommended by current evidence.18,35,36 Thirdly, blinding of participants and personnel could not be performed or was unclear in the included studies.18,35–39 This could affect the results, as the patients may have experienced a nonspecific effect or a placebo effect due to the novel nature of LL-BFR training. Overall, the methodological quality of the included studies ranged from moderate to good. Lastly, no long-term effects of LL-BFR training after ACL reconstruction were reported.
CONCLUSION
The results of this systematic review indicate that LL-BFR training after ACL reconstruction may be beneficial on quadriceps strength, quadriceps mass, and knee joint pain compared to non-BFR training with non-detrimental effects on ACL graft laxity. However, more randomized controlled trials with operational definitions, standardized intervention protocols and outcome measurements are needed to add evidence on the clinical value of LL-BFR training.
Conflicts of Interest
The authors declare no conflicts.