
INTRODUCTION
Hamstring strain injury (HSI) is one of the most common injuries in high-speed running-based sports.1 HSI results from a complex interaction web of modifiable and non-modifiable factors,2 and low hamstring strength has been associated with increased risk of HSI.3–6 Muscle strengthening has also been a focus of HSI rehabilitation programs, while strength recovery has been used as a milestone during treatment progression and return to sport decisions.7–9 Moreover, similar strength levels between limbs (right vs. left, dominant vs. non-dominant, or injured vs. uninjured) have been believed to reduce the risk of injury,10 and measures of between-limb asymmetry have also been commonly used as a return to sport criterion following a HSI.11 Therefore, hamstring strength assessment plays a key role in both the prevention and rehabilitation of HSI.
Isokinetic dynamometry is the gold standard method to assess muscular torque production as a descriptor of strength in humans, with peak torque being the most widely used outcome.12 However, the cost (around US$ 25,000), size, non-portability, and time-consuming protocols make this option not feasible for most clinicians. In the last decade, the single leg bridge test (SLBT) has emerged as a clinical assessment of the hamstring capacity.13 This test requires a single rater and a 60 cm high box. It may be performed at the edge of the field, as well as inside the physical therapy room, gym, locker room or other sports facility. The score is given by the number of valid repetitions performed until exhaustion, and SLBT has good intra-rater reliability (intraclass correlation coefficients of 0.77–0.89 and 0.89–0.91, respectively).13
The SLBT has been introduced in the sports context as a way of estimating the hamstring capacity in a range of athletic populations,13–16 including athletes in rehabilitation following HSI.9 However, considering the nature of the SLBT (i.e., a repetition-to-failure test), it seems reasonable to hypothesize that the SLBT score would not be correlated with the maximum hamstring strength, which is the outcome mostly traditionally related to prevention and rehabilitation of HSI. Therefore, the primary aim of this study was to examine the association between SLBT scores with concentric and eccentric knee flexor peak torques. Secondarily, this study aimed examine the association of between-limb asymmetries provided by SLBT and isokinetic tests.
METHODS
Study Design
In this cross-sectional study, volunteers performed SLBT and isokinetic tests in a single visit to the laboratory. The study was approved by the Federal University of Health Sciences of Porto Alegre (Porto Alegre, Brazil) ethics committee, and all volunteers provided informed consent before starting study participation.
Participants
One-hundred male soccer players were assessed: 51 from senior teams and 49 from under-20 teams (20.06±3.41 years old; 74.81±8.59 kg; 1.79±0.07 m; 12 goalkeepers, 24 backs, 40 midfielders, and 24 forwards). All players had professional work contracts and were regularly engaged in the training routine of two football clubs from a first state division league in Brazil. Professional and under-20 players followed a routine usually encompassing one to two daily training sessions, three to five days per week, according to each team’s weekly schedule (i.e., training, games, and trips). Evaluations were carried out during the first two weeks of preseason.
Procedures
Coaching staffs were informed that players should not perform vigorous training sessions 24 hours prior to assessments. Players received the following recommendations: (i) not to perform high-intensity physical activities 24 hours before the tests; (ii) not to take any kind of analgesic and/or anti-inflammatory drugs 48 hours before the tests; and (iii) not to consume stimulant substances (e.g., caffeine) on the testing day. All players performed the isokinetic test first, followed by the SLBT. The side tested first was alternated between participants.
Isokinetic assessment followed standardized procedures.17 After a general warm-up (five minutes of cycle ergometer exercise), players were positioned in the isokinetic dynamometer (Biodex System 4; Biodex Medical Systems, Shirley, NY) according to the manufacturer’s recommendations. Players performed 10 submaximal concentric knee flexion/extension repetitions at 90°/s for specific warm-up and familiarization with the equipment. Thereafter, two attempts of three consecutive maximum concentric contractions were executed at 60°/s, followed by two attempts of three consecutive maximum eccentric contractions at 60°/s. A one-minute rest period was allowed between attempts. The highest concentric and eccentric knee flexor peak torques were used for data analysis. Considering that body mass plays a role in SLBT performance, peak torque values were normalized by the players’ body mass to ensure a fairer comparison between tests.
The SLBT (Figure 1) was performed only after the volunteer claimed to be recovered from the isokinetic assessment and was ready to perform a new maximal effort. At least a 10-minute rest period was given before performing the SLBT. During the rest period, raters introduced the SLBT to volunteers using video records and standard explanations, following recommendations by Freckleton et al.13 Players were instructed to lie down on the ground with one heel on a box measuring 60 cm high. The testing limb was positioned in approximately 20° knee flexion. Participants were instructed to cross arms over the chest and push down through the heel to lift their bottom off the ground. Players were advised that for the SLBT they should perform as many repetitions as possible until failure. Consistent feedback was provided throughout the procedure to ensure that the correct technique was achieved. Each trial required the participant to touch their buttock onto the ground, without resting, and then extend the hip to 0°. The target height of the upward movement was determined after a familiarization repetition to show to the volunteers the correct execution. This height was measured with a one-meter scale to be repeated during the evaluation of the opposite limb. To be considered a valid repetition, the non-working limb was required to be held stationary in a vertical position to ensure that momentum was not gained by swinging this limb and the knee had to touch the rater’s hand, placed at the target height (i.e., the tested hip at 0°), before returning to the initial position. When the correct form was lost, one warning was given and the test was ceased at the next fault in technique. Maximum valid repetitions were recorded.
.jpeg)
For both SLBT and isokinetic dynamometry, between-limb asymmetry was calculated considering the right limb as the reference one (i.e., between-limb asymmetry represents the left limb percentage difference to the right limb).
Statistical Analysis
The total sample size required for a correlation study with ρH1 = 0.3, α error prob = 0.05, and power = 0.80 was 93 volunteers (G*Power 3.1.9.7). Two hundred limbs (100 on each side) were included in the analysis. Descriptive statistics (mean ± standard deviation, 95% confidence intervals, and minimum and maximum values) was used to describe the participants’ performance. Kolmogorov-Smirnov test confirmed the normal distribution of data. Associations between SBLT and isokinetic dynamometry were assessed through Pearson’s correlation coefficient. The following correlation criteria were adopted: 0, none; ≤0.2, poor; 0.2 ≤ 0.5, fair; 0.5 ≤ 0.7, moderate; 0.7 ≤ 0.9, strong; 1, perfect.18 Trend line equation and r-squared values were calculated to indicate how well the estimated trend line values fit the actual data. Statistical significance was set at 5% (p<0.05) for the comparisons.
RESULTS
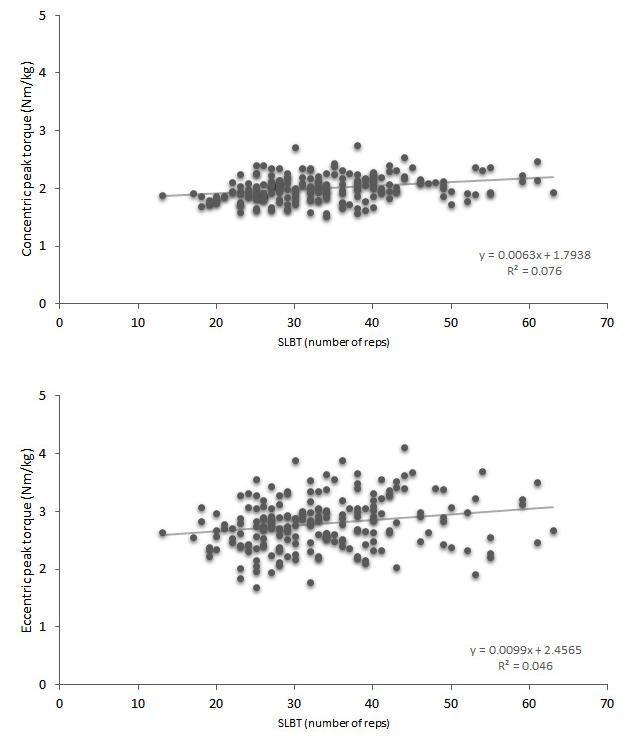
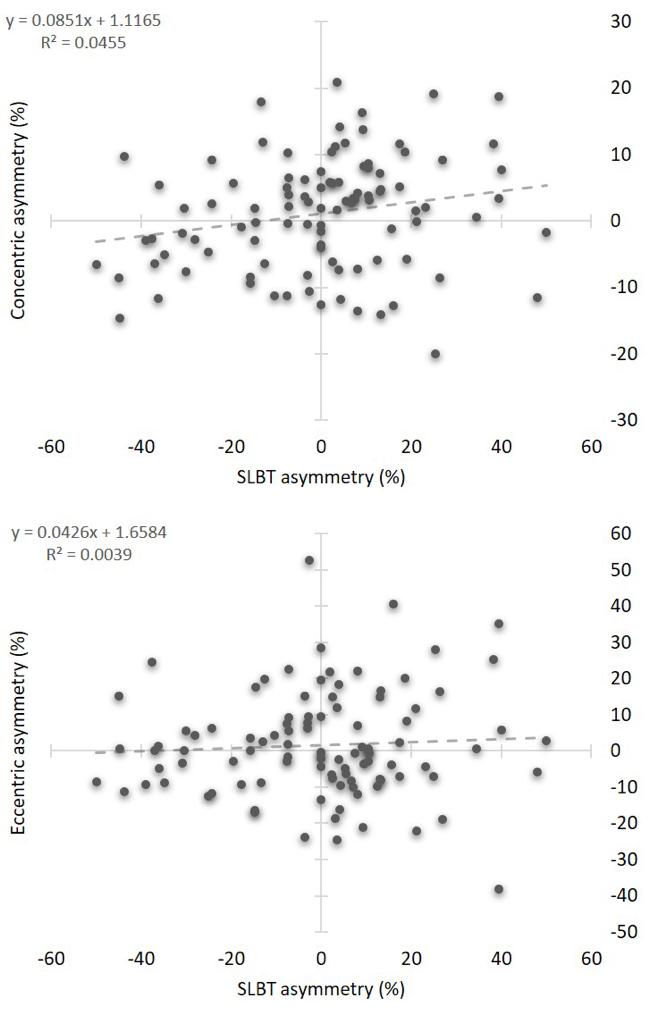
Table 1 summarizes the results of the study. There was a poor association of SLBT score with concentric peak torque (p<0.001, r=0.275) and eccentric peak torque (p=0.002, r=0.215) (Figure 2). The SLBT between-limb asymmetry was poorly associated with asymmetry found in concentric peak torque asymmetry (p=0.033, r=0.213) and was not associated with eccentric peak torque asymmetry (p=0.539, r=0.062) (Figure 3).
_score_with_concentric_peak_torque_(top)_and_e.jpeg)
_between-limb_asymmetry_with_concentric_peak_t.jpeg)
DISCUSSION
The SLBT became popular after a prospective study showed that low scores were associated with an increased risk of HSI throughout the season in Australian football players.13 Since HSI have been usually associated with low levels of maximum strength measured in isokinetic tests3–5 and Nordic hamstring exercise tests,6 interpretation of the SLBT as a new tool for assessment of maximum hamstring strength perhaps has occurred naturally in some contexts. The prospect of evaluating the hamstring capacity using a test with low technology requirements (i.e., just a box) is tempting for clinicians without access to isokinetic dynamometers or other strength assessment devices. However, the results of this study found only poor associations between SLBT scores and isokinetic dynamometry measures, suggesting that SLBT should not be used to estimate the maximum hamstring strength-related outcomes of soccer players.
Maximum strength capacity is a criterion for progression of rehabilitation and return-to-sport following HSI, typically determined using isokinetic dynamometry9 and/or isometric tests performed with hand-held dynamometers.8,9 Mendiguchia et al.9 introduced SLBT as a clearance criterion for semiprofessional male soccer players with HSI. Players were required to perform >25 repetitions and have <10% asymmetry between limbs to be considered able to return to sport, in addition to a range of criteria including maximum hamstring strength asymmetry <10%.9 Findings of the present study further support that SLBT and maximum hamstring strength tests must be used in a complementary manner during the athlete’s evaluation. In other words, an athlete performing SLBT with a high number of repetitions and low between-limb asymmetry will not necessarily perform satisfactorily in some maximum strength testing such as isokinetic dynamometry.
It is important to note that isokinetic dynamometry assesses the isolated action of the knee flexor muscles during concentric or eccentric contractions performed in an open kinetic chain movement. Conversely, SLBT involves maintaining a quasi-isometric knee position while the hamstrings act as hip extensors, while other muscles (i.e., glutes and trunk stabilizers) are simultaneously recruited to perform a closed kinetic chain movement. A growing body of work has emerged highlighting the heterogeneity of hamstring activation in different exercises (e.g., knee-dominant vs. hip-dominant movements),19–22 which could be a factor responsible for the poor association of SLBT scores with isokinetic peak torques. However, the poor association may also be due to the purpose of the isokinetic dynamometry (as performed in the present study) which intends to assess the individual’s capacity to produce maximum strength (i.e., peak torque), while SLBT has already been suggested as a ‘hamstring strength-endurance’ test.9,15 It is plausible that muscular endurance (i.e., resistance to fatigue) is the most dominant factor in a repetition-to-failure test such as SLBT.
It is noteworthy that results of the present study do not belittle or question the usefulness of SLBT. Reliable submaximal strength endurance tests are relevant in the context of assessing the risk of orthopedic disorders (e.g., the role of muscles engaged in core stabilization for low back pain).23 Given that male professional players cover an average total distance close to 11 km in a 90-min game, with 350 m and 1150 m performed in sprints and high-intensity running, respectively,24 fatigue-induced loss of strength in lower limb muscles is an expected phenomenon. Studies conducted with simulated and official soccer games have evidenced that hamstring strength capacity is significantly affected in those situations.25–27 Interestingly, the last third of each half in soccer games are the periods with the highest incidence of HSI.28 Although a cause-effect relationship cannot be established, it seems reasonable that hamstring fatigue may play a role in the higher susceptibility to HSI in the final parts of the game. Thus, assessing hamstring muscle function through a reproducible and feasible endurance test may be valuable and has practical implications for planning prevention and rehabilitation programmes.
Clinicians must be aware of what they are measuring when using SLBT (or any other ‘strength test’ executed in the clinical setting or in the edge of the field). Results of the current study make clear that SLBT does not assess the maximum hamstring strength. Further studies are needed to address the ability of SLBT to accurately estimate the fatigue resistance of the hamstring muscles, since fatigue in other muscles involved in the movement may be responsible for the end of the test. For example, it has been shown that the gluteal musculature has important activation during the single leg bridge,29 possibly higher to that of the biceps femoris.30 Consequently, a gluteus with low fatigue resistance might anticipate the end of the SLBT. Clinicians must also keep in mind that fatigue is a task-dependent phenomenon,31 and a high score in SLBT does not necessarily transfer directly to fatigue resistance in a sporting situation. In other words, it is unknown whether a player with a higher score in a quick, cyclical, repetition-to-failure test such as SLBT responds with less hamstring fatigue to a longer, intermittent, and multicomponent exercise exposition such as a soccer game. Furthermore, despite the increased HSI risk found in Australian football players with low SLBT scores highlights the potential of this assessment tool,13 there is a lack of prospective studies evidencing the association of the SLBT with the HSI in soccer and other sports; thus, caution is recommended in considering SLBT score as a risk factor for HSI in all athletic populations.
The authors acknowledge that the current study has limitations. First, the assessments took place at the first two preseason weeks, thus SLBT scores and isokinetic peak torques likely do not represent the players’ peak fitness. However, this does not compromise the objective of the study to examine the association between the two assessment tools. Second, SLBT and isokinetic dynamometry are physically demanding testing protocols, and both tests had to be carried out in a single visit to the laboratory due to the clubs’ training routine. Although a rest interval was given to volunteers to allow for recovery from the transient fatigue, a hypothetical performance impairment in the second test (SLBT) of some volunteers cannot be excluded. Third, the SLBT depends on the raters ability to perform real-time tracking of the volunteer’s movement technique during the testing execution, warning him about the first fault and ceasing assessment in the second fault. Thus, as with most field tests, some error is inherent to the SLBT, but it is not believed that this compromises the results.
CONCLUSION
In conclusion, the SLBT score of male soccer players is not associated with concentric and eccentric knee flexor peak torques obtained by isokinetic dynamometry. Between-limb asymmetry provided by SLBT is also not associated with isokinetic asymmetry. Therefore, SLBT should not be used as a clinical tool to assess the maximum strength of hamstring muscles. Clinicians interested in maximal hamstring strength-related outcomes for prevention, rehabilitation or performance purposes should use other tests (eg, isokinetic/isometric dynamometry, load cell-based devices, one-maximum repetition test) instead of SLBT to evaluate their athletes.
Conflict of interest
The authors reported no potential conflict of interest.
Acknowledgements
BMB thanks CNPq-Brazil for the research productivity fellowship.