


INTRODUCTION
Hip adductor injuries account for 101 - 43%2 of all non-contact injuries among professional ice hockey players, with 23.5% of strains being recurrent injuries.3 A systematic review discovered that higher level of play and lower hip adduction and abduction strength to be associated with increased risk of adductor injuries across several sports.4 Prior research has established that ice hockey players create robust force during the glide and recovery phase of the skating motion and are at an elevated risk for non-contact musculoskeletal injuries.5 During the ice skating motion, the hip flexors and adductors are the primary stabilizers of the hip and assist with limb deceleration.6 In addition to increased eccentric forces, strength imbalances between the hip extensors and abductors (prime movers) and the hip flexors and adductors (stabilizers) can also lead to an increased risk of injury. The link between hip adductor weakness and subsequent groin injuries has been demonstrated across several sports such as rugby7 and soccer.8 Strength imbalances may present as side-to-side differences predisposing an athlete to injury, often identified during strength screenings.9
Tyler et al10 found pre-season hip adduction strength in professional hockey players to be 18% lower in those who subsequently sustained an adductor strain. In subjects without a history of adductor strains, their adduction strength was 95% of their abduction strength; compared to 78% of their abduction strength in subjects with a history of adductor injuries. The authors concluded a hip adductor-to-abductor strength ratio of less than 80% was highly predictive of future injury, leading to a 17 times greater likelihood of subsequent adductor injuries in professional hockey players.10
Worner et al utilized the five-second squeeze test in 333 professional and semi-professional ice hockey players in Sweden to assess self-reported function and muscle strength, as well as to guide rehabilitative management. A significant correlation was found between hip muscle strength and the ability to discriminate between the “traffic light levels” of discomfort (Numeric Rating Scale 0-2=green, 3-5=yellow, 6-10=red). Subjects who reported discomfort in the “yellow” or “red” levels had reduced adduction and abduction strength compared to players with a “green” light.11 They advocated for frequent and routine squeeze testing to allow for early identification of groin and adductor related injuries, as well as assist with progressing the rehabilitative program.
A similarly designed cross-sectional hip-strength profile study was performed in Australian footballers focused on elite, sub-elite, and amateur players. Prendergast et al7 utilized belt-fixated hand-held dynamometry (HHD) to study hip strength trends across various levels of play in Australian footballers. The authors concluded that hand-held dynamometry with external-fixation has moderate to excellent intra-examiner reliability for hip muscle testing (ICC 2.1 from 0.76 to 0.95)12 as well as high correlation with isokinetic dynamometry for hip strength (r=0.60 to 0.90).13 However, no significant differences (p> 0.05) in isometric hip adduction and abduction strength or resultant strength ratios were found, regardless of leg dominance or playing level. In addition, symmetry was identified between preferred and non-preferred kicking legs at baseline.7
Tyler et al10 proposed that obtaining an adduction-to-abduction strength ratio of 90% to 100% and an adduction strength equal to that of the uninjured side were suitable clinical characteristics for return to ice hockey following a hip adductor strain in professionals. Belt-fixated hand-held dynamometry as described below is a clinically relevant method to assess strength at the rink-side with minimal time and equipment constraints for sports medicine staff.
Therefore, the primary purpose of this study was to compare isometric hip adduction and abduction strength profiles among bantam, high school, tier one juniors, and NCAA Division I collegiate ice hockey players. A secondary purpose was to identify whether differences in strength profiles between dominant and non-dominant limbs exist.
METHODS
Subjects
Male ice hockey players were recruited from five separate teams representing progressively higher levels of play for a cross-sectional population. Researchers contacted coaching staff from each respective team and utilized this contact, along with parent consent for recruitment.
Subjects were included if they were males ages 13 to 23 years old, had ice hockey experience of at least five years, and were currently participating in hockey activities of at least one training session and game per week during the season. Subjects were excluded if they had sustained a lower extremity injury that caused them to miss one or more games in the three months prior to testing, experienced pain during testing, or were unable to provide a maximal voluntary isometric contraction (MVIC). Ethical approval was obtained from the University Institutional Review Board, University Athletics Ethics Committee, and Public Schools Ethics Committee. All participants provided a signed informed consent form prior to participation.
Study Design
Each subject was asked to complete a voluntary questionnaire prior to testing which included their age, weight, height, competitive team level, dominant leg, hockey position, side of the ice for their position/face-offs, hours of skating during in-season and off-season, injury history, and history of adductor strains. Assessments were completed during the 2018 regular season training period. All testing occurred in the first half of the competitive season during November and December of 2018. Testing was completed independently of scheduled training sessions due to varied intensities, duration, and frequency of practices across teams.
Isometric hip adduction and abduction strength was measured for both the dominant and non-dominant legs. The adduction-to-abduction ratio was calculated by dividing the mean adduction score by the mean abduction score. Data was normalized to body mass. Testing order was randomized between players via coin toss for adduction or abduction and leg dominance.
Hip adduction and abduction isometric strength was measured using a hand-held dynamometer with external belt-fixation (Figures 1, 2). The HHD utilized was the MicroFET 2 © (Hoggan Scientific, LLC, Salt Lake City, UT.). Batteries were changed and both units were calibrated prior to each session of testing to ensure accurate data collection. Testing set-up also included the use of portable treatment tables, fixation-belts, and two glass suction cup handles per table. Previous studies have demonstrated HHD with external belt-fixation has excellent inter-tester reliability when assessing hip strength in strong individuals.12 Belt-fixation limits the bias of tester strength, particularly in exceptionally strong athletes such as those in this study.12


The primary (M.O) and co-researcher (G.S) performed the strength assessments. While the inter-rater reliability of the testers was not performed, the assessors completed two familiarization sessions together totaling three hours to ensure they followed the same standardized protocol. Testers measured an equivalent number of players from each team, across all levels of play. A standardized procedure was utilized with random placement of subjects between the two testers to mitigate bias. The protocol utilized was modeled after that previously described by Thorborg et. al.12 Subjects were positioned in supine with the leg in neutral, which has been found to detect larger adductor impairments at 0 degrees compared to 45 degrees.14 A fixed belt was positioned holding the HHD 10 cm proximal to the apex of the lateral malleolus with the position marked bilaterally prior to the beginning of familiarization trials. A mark was placed to ensure appropriate set-up when transitioning between adduction & abduction trials bilaterally (Figure 1, 2). Submaximal familiarization trials were provided for both adduction and abduction testing positions to ensure the correct application of force through the HHD and gradually adding tension over the five second trial and test. Five efforts were completed for each muscle group testing position: two warm-up efforts at 50% and 75% of MVIC and three efforts at 100% MVIC. All contractions were held for five seconds, with a 30-second rest between each warm-up and testing trial to avoid fatigue. The mean of three trials was used for statistical analysis. The examiners used a standardized command for encouragement given to each participant of “3-2-1 and push, push, push, push, and relax.”8
Statistical Analysis
Data was analyzed using IMB SPSS Statistics version 25. All data were assessed for normality using the Shapiro-Wilk test and found to be normally distributed. Demographic information was calculated and presented as means and standard deviations. A series of one-way analysis of variance (ANOVA) were used to assess if there were any significant differences in demographics between playing levels. Post hoc Bonferroni adjustments were performed for any significant main effects between tests. Data was normalized for kg of bodyweight.
A series of two-way and three-way ANCOVAs were conducted to determine the effect of playing level and limb dominance on peak hip isometric strength and hip strength ratios after controlling for age and team allotment.
RESULTS
Eighty-seven male ice hockey players were included with a mean age of 17.6 ±2.54 years. Bantam players (n=17) were recruited from the local youth hockey association, comprising their highest level of bantam AA ice hockey players under age 14 players. High school varsity players (n=29) were recruited from two local high schools aged 15 to 18 years. Tier one junior players (n=22) were recruited from the state’s United States Hockey League (USHL) team consisting of premier skaters under the age of 20, no longer playing high school hockey and hoping to play collegiately. Finally, elite division I NCAA athletes (n=19) were recruited from the state’s university, competing in the National Collegiate Hockey Conference (NCHC) with multiple players having National Hockey League commitments.
Players of all positions were included, consisting of nine goalies, 28 defensemen, 11 centers, and 38 forwards. Ninety-four percent of subjects reported being right leg dominant based on their preferred leg to kick a ball, while 32.2 % reported being right-handed shooters. 34.9% reported a history of previous hip adductor injury [F(1, 87)=2.295, p=.084, power=.560]. A significant difference was found between height of the bantam players compared to all other teams, with their height being significantly less. There was no significant difference in age, height, weight, or BMI among high school, semi-professional, or collegiate players.
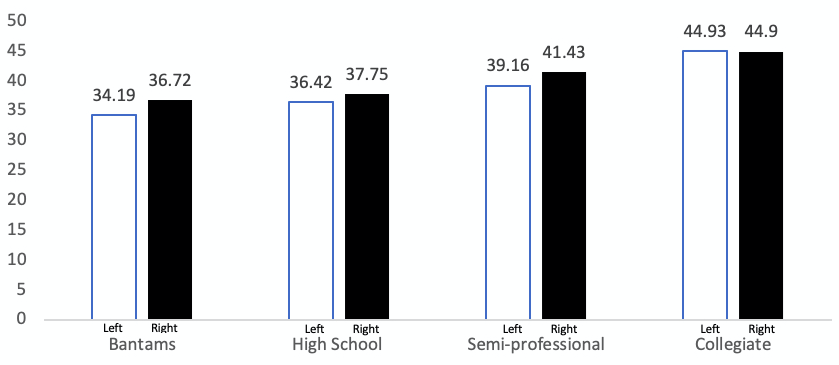
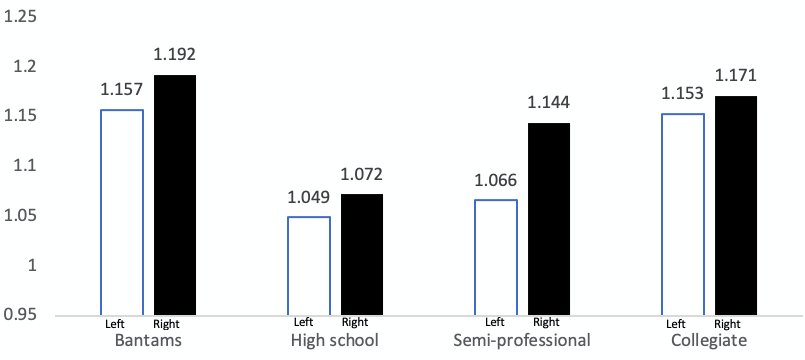
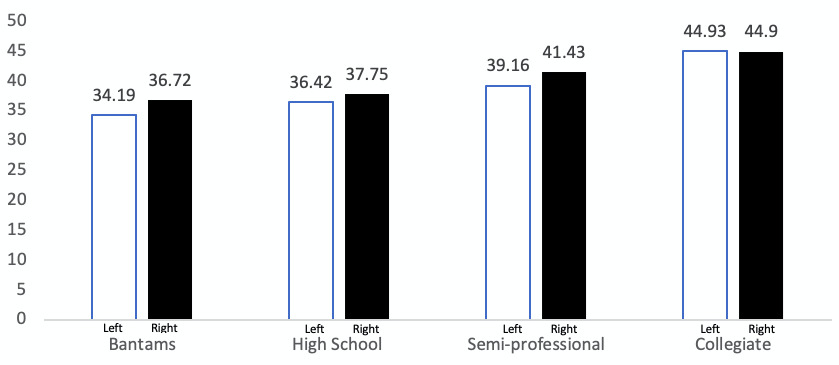
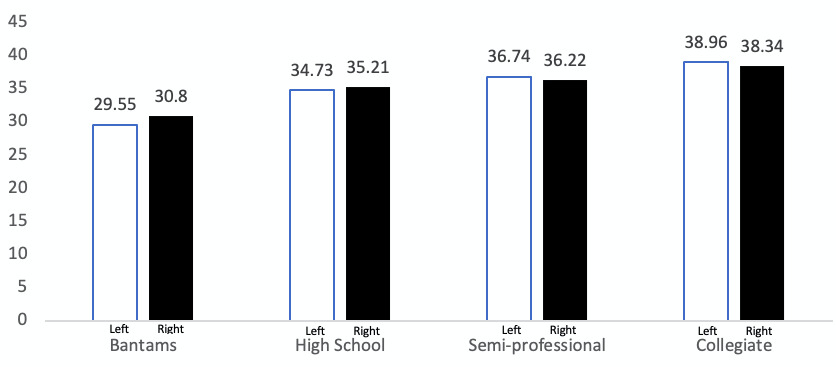
Of the 87 ice hockey players recruited for this study, no significant difference was found between playing levels for the ratio of hip adduction-to-abduction strength profiles. The isometric hip adduction and abduction strength of each playing level are represented below (Figures 3, 4, 5). Without adjustments, the ANOVA for peak hip adduction and abduction isometric strength demonstrated no significant interaction among playing levels when normed for bodyweight. No subjects were excluded from testing due to injury, illness, or pain with maximal voluntary contraction. (Table 1). Force in pounds per kilogram of bodyweight is shown in Table 2.

No significant differences in hip strength ratios were found between dominant and non-dominant kicking legs across all levels of play. Furthermore, no significant difference was found between unilateral mean adduction or abduction strength and shooting hand or leg dominance.
In this sample, 52.9% of participants played one sport competitively (ice hockey), while 47.1% competed in at least one additional sport competitively during the year. No difference in injury risk existed between ice hockey specialized and multi-sport participants. Regarding injury, 39.1% reported a past history of lower extremity injury, excluding groin injury, however, 34.9% of participants reported a history of previous groin injury.
Three subjects were identified as having a unilateral adductor-to-abductor ratio of less than 80%, while two additional subjects were found to have ratios below 80% bilaterally (Table 3). These seven limbs represent 5.7% of all participants and 4% of all limbs tested. Of those identified, three were members of high school teams, one was a member of the semi-professional team, and one was a member of the collegiate team. Those with left-sided adductor-to-abductor ratios of less than 80% (four subjects) reported being right leg dominant and shot left-handed, 75% of whom reported a history of prior adductor injury. In addition, both athletes who recorded strength ratios below 80% bilaterally reported a history of prior adductor injury.
DISCUSSION
This is the first study to analyze hip adduction and abduction strength profiles across bantam, high school, tier one juniors, and collegiate American ice hockey players. The primary purpose of this study was to compare the hip strength ratios among a cross-sectional group of American ice hockey players. The secondary purpose was to assess effects of limb dominance, and determine if differences existed between the dominant and non-dominant limb hip strength ratios. The results demonstrated that there were no significant differences in hip adduction or abduction strength between dominant and non-dominant legs, shooting hands, or playing level in this sample when strength was normalized to bodyweight. This indicates the potential of assuming symmetry between dominant and non-dominant legs when it comes to tracking a player’s post-injury return-to-play progression. Utilizing average force to bodyweight regardless of age (Table 2) makes assessing hockey specific strength feasible at the rink-side.
These results are in contrast with findings by Thorborg et al.8 who demonstrated that the dominant leg was significantly stronger in elite soccer players, where unilateral actions are more prevalent. The findings may be attributed to the mechanical differences between soccer and hockey players as it relates to preferred kicking leg and functional strength requirements between sports.
Additionally, Tyler et al.10 reported contrasting findings in hip adduction-to-abduction strength ratios when testing professional ice hockey players using pre-season break-testing. The authors found pre-season adduction-to-abduction ratios to be 0.95 in uninjured players compared to 0.78 in players who went on to sustain an adductor strain. The collegiate subjects in the current study demonstrated in-season adduction-to-abduction strength ratios of 1.15 to 1.17. Differences in testing position between studies may contribute, as sidelying break tests of eccentric adductor strength were used in professional ice hockey. They also demonstrated lower unilateral hip strength ratios on the side that was subsequently injured. Similar findings between players experiencing groin pain and those without groin pain have been illustrated in soccer players, with those having groin pain being nearly 50% weaker than their non-painful counterparts.8 Studies in both soccer8 and rugby7 have demonstrated elite players as being significantly stronger than their lower-level counterparts, but this was not apparent in our sample when normed for bodyweight (Table 4).
The findings of the current study demonstrated bilateral adductor symmetry, similar to those found in soccer players8 and rugby players.7 While this finding is less common across other sports, it may represent a more common phenomenon in sports with high components of lateral movement, performed bilaterally and repetitively like ice skating. Previously, researchers have suggested that adductor and abductor strength ratios were lowest during the pre-season and increase throughout the season. These same authors proposed that soccer-specific strength likely deteriorates during the off-season and may place the athlete at an increased risk of injury when resuming sport specific activity.15
This study is limited by the smaller sample size from elite and bantam players. The results may not generalize to the public and athletes of all sports but do accurately reflect the captured hockey population.
CONCLUSION
The results of this study indicate that there were no significant differences in isometric hip adduction or abduction strength ratios between dominant and non-dominant kicking legs in American hockey players across various levels of play. Across all playing levels, ice hockey athletes generate approximately 0.5 lbs/kg of bodyweight with their adductors and 0.45 lbs/kg of bodyweight with their abductors.
Conflicts of interest
The authors report no conflicts of interest or relevant financial disclosures.
Statement of IRB/Ethics Committee Approval
Ethical approval was obtained from the University of North Dakota Human Research Ethics Committee, University of North Dakota Athletics Ethics Committee, and Grand Forks Public Schools Ethics Committee.
Acknowledgement
The authors thank Renee Mabey for assistance with data analysis, Cathy Ziegler and Scott “Jake” Thompson for encouragement and assistance throughout the University of North Dakota Sports Physical Therapy Residency Program.