


INTRODUCTION
A previous study has reported that there was no difference in draft rank, games missed, or performance across uninjured, nonoperative, and operative players for those who were drafted by Major League Baseball (MLB) organizations.1 However, only 59% of the 216 high school to professional level pitchers could return to play at the same level or higher after superior labrum (SLAP) repairs.2 Indeed, overhead throwing athletes who underwent SLAP repairs on the throwing side had at least a two times less likely to return to their previous level activity, compared to non-overhead athletes.3 Consequently, it is critically important to identify the factors that predispose baseball pitchers to increased shoulder injury risk.
The scapular dyskinesis test has been implemented in visual dynamic assessment schemes that seek to classify altered scapular motion, which has been intriguing to clinicians and researchers.4–15 Previous meta-analyses have demonstrated that asymptomatic athletes with the presence of scapular dyskinesis at baseline increased their risk of developing shoulder injury by 25% to 43%, compared to their counterparts without scapular dyskinesis.16,17 However, no significant relationship was observed between scapular dyskinesis and throwing-related shoulder injury.17 Those meta-analyses included heterogenous subjects in a variety of sports from preadolescent to elite cohorts, whereby adverse internal variability should be considered. In contrast, scapular dyskinesis on the dominant side has been demonstrated to be associated with a decrease in throwing arm conditions identified by a self-report outcome assessment for collegiate baseball pitchers during the course of a single season, while no difference was found in the throwing arm conditions for position players regardless of scapular dyskinesis.13 Additionally, Tsuruike et al14 reported that a collegiate baseball pitcher with the history of SLAP repair showed moderate scapular dyskinesis, in which the medial border of the scapula was abruptly protruded on the throwing arm side during weighted arm lowering in the sagittal plane.
The protocol of the scapular dyskinesis test has been demonstrated to vary with different weight loads ranging from no external weight to the use of 5 kg held in both hands. Bilateral arm movement speed also varies with different instructions ranging from two to five seconds to complete each elevation and lowering phase, and multiple planes of motion have been used including the sagittal, coronal, and scapular plane.4–14,17 Tsuruike et al12 demonstrated that EMG activity of the anterior deltoid and upper trapezius decreased during arm lowering from full flexion (eccentric contraction), compared to arm elevation (concentric contraction) during the scapular dyskinesis test. This physiological research provides rationale for the clinician to utilize the addition of weight in order to structurally stress the stability of scapulae as there appears to be less muscular activation during the arm lowering phase. Furthermore, the authors12 observed that collegiate baseball players developed an adaptation in periscapular muscle activity during the scapular dyskinesis test in which the upper trapezius muscle was less activated on the dominant side than on the non-dominant side, while the lower trapezius muscle was more activated compared to the non-dominant side.
Few prospective cohort studies have investigated whether the presence of scapular dyskinesis identified during the preseason in baseball pitchers may predispose them to throwing-related injuries during the course of intercollegiate baseball seasons. Therefore, the purpose of this study was to study the relationship between the presence of scapular dyskinesis and throwing-related injury in collegiate baseball pitchers during each respective course of up to four subsequent seasons. The authors hypothesized that collegiate pitchers with scapular dyskinesis would have an increased incidence of throwing-related injury during the course of intercollegiate baseball seasons.
METHODS
Participants
A single Division 1 National Collegiate Athletic Association team participated in this study over a four-year-period. All subjects met during preseason meetings in January and gave informed consent to the procedures as approved by the Institutional Review Board in the Office of Research at San José State University prior to data collection each year. This study prospectively followed these players throughout each respective season pertaining to incidence of upper extremity injury. The inclusion criteria were that the subjects had to be asymptomatic competitive baseball pitchers, free from neurologic or physiologic conditions in their upper body prior to each upcoming season. Pitchers were excluded from participation if they appeared in two games or less during each season. Each season typically consisted of 56 (± 1.3) official games over an average of 95 (± 3.7) days.
Procedures
The scapular dyskinesis test was conducted in the second week of January during the preseason each year. The subjects were asked to in the standing position, simultaneously lower both arms from full flexion with a 3.2 kg wrist cuff worn on both extremities over a five-second period while following a metronome set at 60 beats per minute.12–14 The amount of weight used during the scapular dyskinesis test was based on previous studies.12–14 The scapular dyskinesis test was recorded with a digital video camera (Panasonic Camcorder HC-V770, Osaka, Japan) that was mounted level on a tripod four feet from the floor and set seven feet behind the subject. The videotape was copied and distributed to one physical therapist (PT) and two athletic trainers (AT) who determined the Kibler scapular classification types at around 90° of shoulder flexion on both sides during the lowering phase of the arm movement.6 All three of the examiners had two-to 10 or more years of experience in the performance and interpretation of the scapular dyskinesis test in clinical practice with overhead athletes including baseball players and had published in this area. Player’s hand dominance was not disclosed to the examiners throughout the scapular dyskinesis assessments. Subsequently, this study classified the athletes into four patterns of scapular kinesis: 1) both sides with scapular dyskinesis, 2) scapular dyskinesis on the throwing side but not on the non-throwing side, 3) scapular dyskinesis on the non-throwing side but not on the throwing side, 4) neither side with scapular dyskinesis.
Data analysis
Athlete-exposures (AEs) were calculated for each of the throwing-related shoulder and elbow injuries with the number of pitchers involved during the course of the respective season over the four year-period including both practices and games. The team had one no-practice day every week for 14 weeks or the average of 95 days during the respective season, leading to the average of 81 days which were used to calculate AEs. Odds ratios were calculated to describe the association of throwing-related injury between pitchers with and without scapular dyskinesis along with descriptive statistics for incidence of injuries. Also, the p-value of the odds ratio was calculated as the area of the normal distribution that fell outside ± z value.18
The initial scapular dyskinesis assessments were analyzed using the four-type Kibler classification system.6 In the Kibler classification all Type I, Type II and Type III findings were transposed and recorded as a “yes” value for scapular dyskinesis and all Type IV findings were transposed and recorded as a “no” value for no presence of scapular dyskinesis.5,13,15 The inter-rater reliability of scapular dyskinesis was then calculated using the yes/no classification system15 that was used to identify the degree of agreement between two examiners in terms of the presence of scapular dyskinesis.
RESULTS
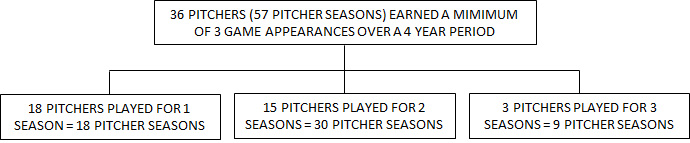
A total of 36 male collegiate baseball pitchers (height: 185.3 ± 5.6 cm, weight: 88.8 ± 7.8 kg, age: 20.0 ± 1.5 years) were included; 18 pitchers who were rostered for only one season, 18 pitchers remained with the team for more than one year and were subsequently tested each year they were active on the roster. Fifteen out of the 18 were rostered for two seasons, and three were rostered for three seasons (Figure 1).

The inter-rater reliability yielded an 92% agreement, resulting in a kappa (κ) correlation of 0.81 between the PT and AT1 on the throwing side of 13 pitchers while it was a 77% agreement with a κ correlation of 0.55 for the non-throwing side. Similarly, the inter-rater reliability yielded an 84% agreement with a κ correlation of 0.68 between AT1 and AT2 for the throwing side of 44 pitchers while it was a 77% agreement with a κ correlation of 0.56 for the non-throwing side. In the case of disagreement, two examiners reviewed the video together and obtained a consensus. As a result, 27 pitchers were classified as having scapular dyskinesis on the throwing side during the lowering phase of arm movement. For those 18 pitchers who remained with the team for more than one year, 81.0% of the scapular dyskinesis test results were not changed on the throwing side from the previous to the following year, whereas 42.9% of the results remained unchanged on the non-throwing side. Examples of scapular presentations are provided in Figures 2a and 2b.


Thirty-eight injuries were diagnosed by the team physician over the four year-course of seasons. This included eight shoulder injuries. Three shoulder injuries were subsequently excluded from analysis due to nonthrowing-related mechanisms: two injuries occurred during batting practice (biceps subluxation) and weightlifting (biceps tendinitis), and the other injury occurred on the non-throwing side (anterior instability) (Table 1). As a result, five injuries (13.2% of a total of 38 injuries) were described as throwing-related shoulder injuries, which occurred during the course of the intercollegiate baseball seasons. None of the five throwing-related shoulder injuries occurred in the same pitcher. All of the injuries were diagnosed as overuse or chronic injuries, including three cases of subacromial impingement syndrome (SIS), one SLAP lesion, and one case of thoracic outlet syndrome (Table 1).19 None of the injuries were acute or of sudden onset.
The incidence rate of throwing-related shoulder injury for the pitchers was 1.04 per 1,000 AEs during the course of the season. The five injured pitchers were disabled from throwing until each of them was re-evaluated and allowed to pitch by the team physician during each respective course of season. The number of days at the onset of injury from the first day of game were 30 (± 14) on average for those pitchers with scapular dyskinesis while the number of days to return to play from the onset of injury were 19 (± 14) on average.
Ten throwing-related elbow injuries were diagnosed by the team physician over the four seasons (26.3% of a total of 38 injuries). The incidence rate of throwing-related elbow injury was 2.08 per 1,000 AEs during the course of season. Those injuries included seven ulnar collateral ligament (UCL) sprains, two medial muscle-tendon strains, and one case of lateral epicondylitis without throwing-related shoulder injury (Table 1). One pitcher who had a history of UCL sprain in the previous year developed another UCL sprain in the following year. The rest of the throwing-related elbow injuries occurred in nine different pitchers. Also, one pitcher who suffered SIS also developed a mild UCL sprain.
Four of the five pitchers with throwing-related shoulder injuries were classified with the presence of scapular dyskinesis on their throwing side (Table 2). The odds of shoulder injury for the pitchers with the presence of scapular dyskinesis on their throwing side was 0.174 (4 divided by 23 pitchers), compared to the odds of 0.034 for the pitchers without the presence of scapular dyskinesis (1 divided by 29 pitchers). Subsequently, the odds ratio was 5.04 [95% confidence interval (CI): 0.53-48.3]. However, no significant difference was observed in the frequency of throwing-related shoulder injury between the pitchers with and without the presence of scapular dyskinesis (p = 0.16).

Seven out of the 10 pitchers who did not have the presence of scapular dyskinesis on their throwing arm side developed throwing-related elbow injuries (Table 2). Thus, no relationship was considered between the presence of scapular dyskinesis on the throwing arm side and a throwing-related elbow injury.
DISCUSSION
Forty-seven percent of the collegiate baseball pitchers showed the presence of scapular dyskinesis on their throwing arm side. Subsequently, five throwing-related shoulder injuries were observed over the four year-course of collegiate seasons while 10 throwing-related elbow injuries were observed. The ratio of throwing-related elbow to shoulder injuries observed in this study were similar to a previous study in which predraft baseball players incurred throwing-related elbow injuries 3.5 times as many as shoulder injuries.1 The results of the current study prospectively indicated that collegiate baseball pitchers with the presence of scapular dyskinesis on their throwing side increased odds of suffering throwing-related shoulder injuries, compared to those without the presence of scapular dyskinesis during the course of a season, although the odds ratio did not reach a significant difference (p = 0.16). The findings of this study were not fully consistent with previous studies. Shitara et al20 demonstrated an odds ratio of 1.23 for high school baseball pitchers with the presence of scapular dyskinesis, compared to pitchers without scapular dyskinesis. The authors followed the protocol of the scapular dyskinesis test utilized by Uhl et al15 in which the subjects elevated arms in the sagittal and scapular plane without an external weight load. As a result, they identified the presence of scapular dyskinesis in 22 (28.2%) out of the 78 pitchers available for the assessment while they prospectively found 21 shoulder/elbow injuries during the course of season. It is plausible to speculate that no external weight application in their scapular dyskinesis tests decreased the ability of the test to identify scapular dyskinesis.
Another previous research study using the protocol of the scapular dyskinesis test performed bilaterally with 2.3 kg weights in both sagittal and coronal plane arm movements7 identified the presence of scapular dyskinesis in 122 of the 246 (49.6%) high school baseball players on the dominant side including both subtle and obvious scapular dyskinesis.9 The authors, however, did not find throwing-related upper extremity injuries to be related to the presence of scapular dyskinesis. One possible reason for the difference in the findings of this study might have been their inclusion of not only pitchers but also position players in their prospective study. High school pitchers are nearly two times more vulnerable to noncontact and overuse shoulder and elbow injuries than position players.21 Based on this injury prevalence finding, prospective studies should be exclusively implemented with baseball pitchers regarding the relationship between throwing-related shoulder injuries and scapular dyskinesis. Both previous studies suggested potential alterations of scapular dyskinesis during the course of the season while two of the studies did not re-examine scapular dyskinesis later in the season.9,20 The present study found that 81.0% of the scapular dyskinesis test results were not changed on the throwing side from the previous to the following year for those 18 pitchers who remained with the team for more than one year. This indicates that most, if not all, of the highly competitive collegiate baseball pitchers had likely developed their scapular adaptations related to long-term repeated throwing motions.
In addition to scapular dyskinesis on the throwing side, clinicians need to be aware of habitual throwing-related scapular adaptations, such as greater degrees of internal rotation and anterior tilt of the scapula on the dominant side, compared to the non-dominant side.22 This internal rotation of the scapula has been argued in a cadaveric study to predispose baseball pitchers to increase the area of internal impingement generated during maximal external rotation in the late cocking phase of the throwing motion.23 In addition, glenohumeral internal rotation deficit often seen in baseball pitchers along with posterior capsular thickening24,25 may increase the anterior tilt of the scapula to create what is known as “a wind-up effect” of the scapula.26
Factors implicated in the mechanism of UCL injury include peak and mean pitch velocity, body weight, height, and age.27 These predictive factors may yet explain 7% of variance in UCL reconstruction rates in MLB pitchers.27 With respect to scapular dyskinesis associated with UCL injury, a cadaveric study revealed that an increase in the internal rotation of the scapula significantly increased the valgus torque of the elbow in the position of maximum glenohumeral external rotation, compared to the resting scapular position.28 However, the results of the present study are not consistent with those of Itami et al,28 and found that no relationship was observed between the scapular dyskinesis test and throwing-related elbow injuries in collegiate baseball pitchers.
Limitations
This study included collegiate baseball pitchers with asymptomatic shoulders at baseline. Thus, the implication of the findings to individuals of differing ages, levels of performance, and presence of shoulder symptoms should be limited. Also, the athletes in this study sustained only five throwing-related shoulder injuries over four seasons, which might be insufficient to conclude no statistical relationship in throwing-related injuries for the baseball pitcher with the presence of scapular dyskinesis. Additionally, the amount of weight load used in the scapular dyskinesis test was 3.2 kg which may indicate another limitation. However, the mean body weight of the subjects in this study was 88.8 kg, which was 20 kg more than that of the previous studies advocating the weight load of 2.3 kg for the scapular dyskinesis test.20,24 Those previous studies were also implemented with heterogeneous overhead athletes including female athletes and different NCAA divisions, such as water polo, swimming, volleyball, tennis, and softball, in addition to baseball. Consequently, the authors suggest that the amount of weight load used in a study of the scapular dyskinesis test should be discerned for the type of sport in which the athlete participates as well as the subject’s body weight. An additional limitation might include the athletes who were observed over the course of two to three seasons although none of the five throwing-related shoulder injuries diagnosed were in the same subjects.
CONCLUSION
The results of this study indicate that collegiate baseball pitchers with the presence of scapular dyskinesis had increased odds of suffering throwing-related shoulder injury, compared to those without the presence of scapular dyskinesis over the course of four seasons. However, no statistically significant difference in injury was observed between those with and without the presence of scapular dyskinesis on the throwing side, likely owing to insufficient throwing-related shoulder injuries observed during the course of this study. Further studies are warranted to investigate the application of the currently advocated scapular dyskinesis test and its relationship to throwing-related injury prevention in baseball players.
Conflicts of interest
The authors report no conflicts of interest.
Acknowledgement
The authors thank Connor Lauffenburger, MA, ATC for his assistance with data collection during this study.