INTRODUCTION
Shoulder pain related to pathology of the long head of the biceps tendon (LHBT) can be debilitating and often interferes with an individual’s activity and participation.1–3 The biceps tendon and labral complex is a potential pain generator in overhead throwing athletes.4–6 Anterior shoulder pain caused by tenosynovitis of the LHBT in athletes can lead to decreased performance and persistent pain.4,7,8 LHBT “tendinopathy” may start as an inflammatory condition or tenosynovitis of the LHBT1–3 and progress to a degenerative tendinopathy of the LHBT (characterized by tendon thickening, disorganization and irregularity of the tissue including the presence of hemorrhagic adhesions and scarring).3 The incidence of LHBT tendinopathy remains unclear as it is often considered a secondary shoulder condition associated with other conditions including rotator cuff disease and subacromial impingement.1,8 However, the reported incidence of tendinopathies in sports appears to be rising due to increased participation and training frequency.9 Overall, the literature regarding diagnosis, appropriate management of disorders related to the LHBT, including physical therapy (PT) management and surgical intervention, especially in the younger, athletic population remains controversial.1,4,8,10
Management of LHBT tendinopathy may include rest, activity modification, non-steroidal anti-inflammatory drugs, corticosteroid injections and tendon fenestration.1,8,11 More invasive, surgical interventions include biceps tendon distal reattachment (tenodesis) or release (tenotomy).1,12 However, there is little consensus regarding the ideal approach to treating chronic pain related to the LHBT.2,3 Conservative management including PT is often recommended prior to more invasive interventions,3,13,14 yet conservative management may be suboptimal in relieving symptoms and many individuals go on to seek more invasive treatment alternatives including surgical intervention.
Conservative PT management of shoulder pain including LHBT pathology may involve a multimodal approach addressing associated impairments of the shoulder, scapular region and cervicothoracic spine with the application of exercise, joint and soft tissue mobilization as well as retraining dysfunctional movement patterns.3 A search of the literature revealed that most randomized controlled trials exploring PT management for LHBT conditions involved the utilization of biophysical agents including ultrasound, electrotherapy, extracorporeal shockwave therapy and iontophoresis however, there remains a paucity of high quality literature outlining the conservative management of LHBT tendinopathy in isolation.15–20 Considering chronic biceps tendinopathy often leads to invasive surgical intervention it is essential for physical therapists to recognize interventions that can be potentially effective in treating LHBT tendinopathy to avoid such procedures.21 Currently no quality studies have identified the most effective interventions for treating individuals with LHBT tendinopathy. Expert opinion in the form of the Delphi method is an important tool in fostering decision making when evidence is lacking.22 Therefore, the purpose of this study was to perform a Delphi study on common PT interventions utilized to treat individuals with biceps tendinopathy in order to generate expert consensus on recommended PT interventions.
MATERIALS AND METHODS
Study design
This study used a Delphi method to elicit opinions and determine consensus from targeted content experts.23 This design allowed for the recruitment of international content experts without constraints of geography, offered anonymity, and avoided the dominance of opinion by a minority. The web-based Delphi consists of three rounds of surveys with both a panelist (respondent) group and a work group (investigators) in order to answer the following question: Which conservative interventions are effective in treating individuals with long head of the biceps tendon tendinopathy? The three-step Delphi method took place between February and June of 2021. This research received exempt status by the University of Colorado Multiple Institutional Review Board (COMIRB) and was approved by the Human Research Ethics Committee (HREC) at the University of Newcastle; all participants provided informed consent prior to participation. The study was performed in line with the Conducting and Reporting Delphi Studies (CREDES) recommendations to assure study rigor.23
Participants and Recruitment
In line with CREDES recommendations, experts were sought globally23 and were defined and agreed upon by the work group. Experts on shoulder pain were systematically identified using three methods. First, experts were identified as clinicians and/or researchers who had international and nationally recognized training and experience in the PT management of shoulder pathology or experience in research related to specific PT interventions utilized to treat individuals with shoulder pain and/or pathology. Relevant manuscripts and abstracts were collected utilizing electronic libraries including PubMed, CINAHL and Google Scholar. Investigators composed a list of potential panelists consisting of physical therapists and researchers listed as first/last authors of peer-reviewed publications on the PT management of individuals with shoulder pathology. Second, experts were identified through presentation abstracts and records of conference programming specifically, individuals who had presented on shoulder pathology at the 2019 and 2020 American Physical Therapy Association (APTA) Combined Sections Meeting (CSM) specifically in the Orthopedics, Research, and Sports Sections. Third, experts were identified by searching the grey literature through Google to include additional conference proceedings, textbooks and non-peer-reviewed nationally or internationally published material. Experts were invited via email to participate in the study.
Work Group
The work group consisted of the five authors of the study: the lead investigator (AM, a board-certified orthopedic specialist and a fellow in the American Academy of Orthopaedic and Manual Physical Therapists), two senior academics (SS and JC), with experience in the Delphi technique, quantitative research methods and 50 years of combined experience in musculoskeletal medicine, and two research assistants (SA, LC) completing doctoral training in PT. The work group was responsible for study design, recruiting content experts, and circulation and analysis of the questionnaire data. Additionally, the work group made decisions regarding methodology, data analysis and quality assurance.
Systematic review of the literature
A systematic review of the literature was performed prior to questionnaire development to identify best practice for the PT management of LHBT tendinopathy. The electronic databases MEDLINE, CINAHL, Cochrane Library, PubMed and Physiotherapy Evidence Database (PEDro) were searched from inception to June 20, 2020. The search was developed and performed with assistance from a research librarian. The search strategy combined headings and keywords for “biceps tendinopathy” or “biceps tendinitis” and “physical therapy” or “management” or “rehabilitation.” Individuals from the work group screened titles and abstracts to discard irrelevant ones. Articles from the literature search were included if they described or recommended PT interventions. Articles discussing medical or surgical interventions were excluded. Full-text publications were searched for information relevant to PT interventions used to treat individuals with LHBT tendinopathy. Data extracted from the full-text publications were then used to guide development of general themes presented in the Round I Delphi survey.
Procedure
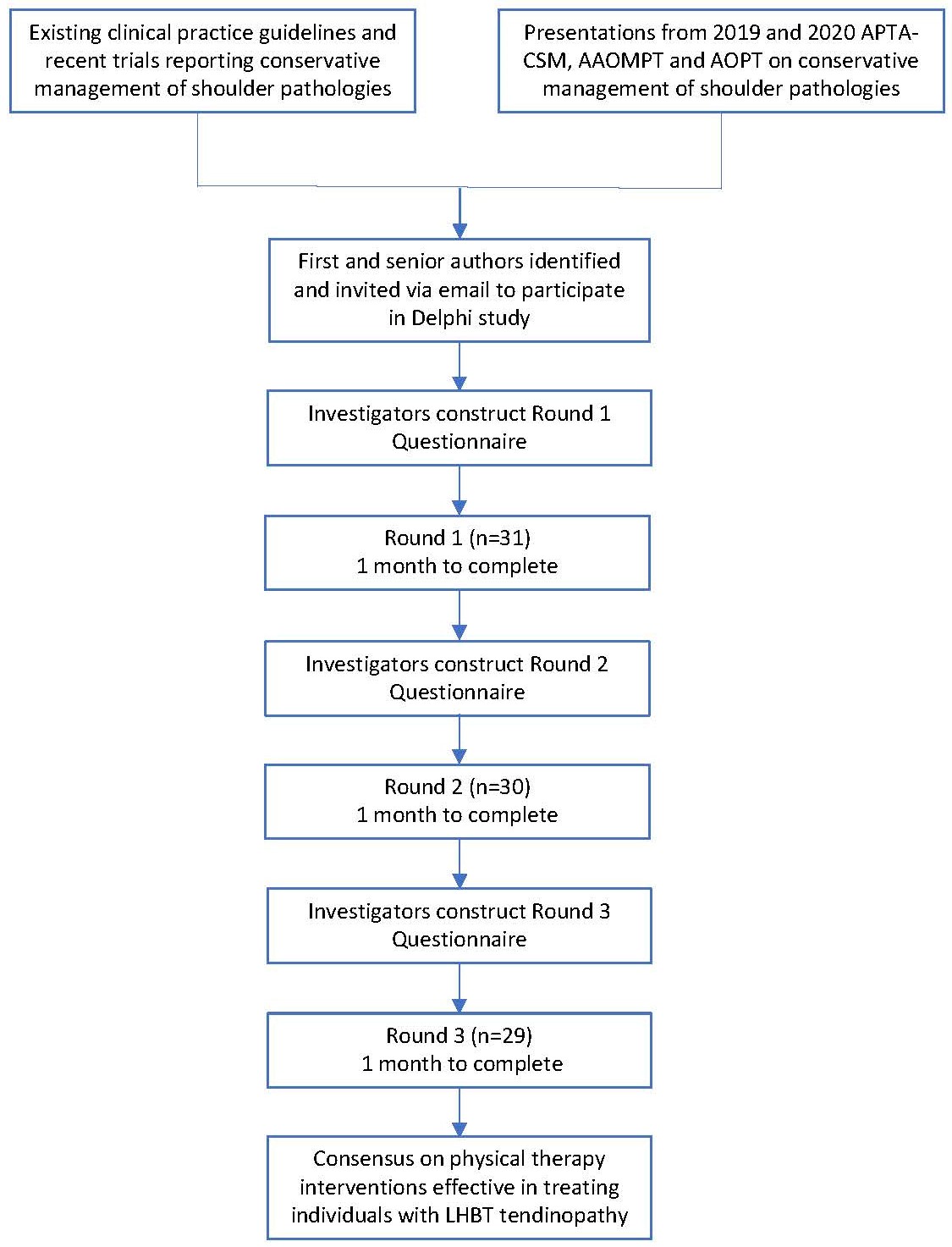
This Delphi consisted of a preparatory phase by the work group and three rounds of electronic surveys conducted via the Qualtrics (Qualtrics, Provo, UT) online platform. An email was sent to 136 potential panelists inviting them to participate in the Delphi survey, including a link with information about the study, informed consent, privacy, and a link to complete the Round 1 survey online. Email invitations generated from Qualtrics with links for Rounds II and III were sent to all respondents who completed Round I. Each Delphi round was conducted over a four-week period with three reminder emails to ensure survey completion. Between each round, investigators performed data management, analysis, subsequent survey creation, and survey testing for two weeks. An introductory invitation containing the link to the consent and Round I questionnaire was sent to the list of identified experts to inform them of the study and request their participation via email. Two weeks later, the invitation to participate was sent again to all experts who did not decline participation. Three follow up emails were sent to non-responders at intervals of one week. Throughout the entire Delphi process, all participants were blinded to the identity of the other participants in the respondent group. Details of participant recruitment can be found in Figure 1.

Instrument
Round I of Delphi
The first instrument consisted of an information statement describing the study, informed consent, demographic questions, and nine open-ended questions on the conservative management strategies that the participants believe are most common and effective for the physical therapy treatment of individuals with LHBT tendinopathy (Appendix 1). The first two open-ended questions inquired about general interventions followed by six open-ended questions on interventions including exercise-based interventions, manual therapy, and biophysical agents. The last question asked for further comments on PT interventions used to treat individuals with LHBT tendinopathy. The purpose of Round I was to gather information and inform investigators of the most common and effective interventions utilized, or believed to be utilized, to treat individuals with LHBT tendinopathy. The use of open-ended questions was intentional to reduce the potential for bias and allow individuals to describe interventions openly.
Definitions of all terms were provided upon initiation of the survey to assure familiarity and congruence with the terms. The definition of LHBT tendinopathy used for the purpose of the study was: an inflammatory condition or tenosynovitis, occurring in the path of the LHBT as it courses in the intertubercular or bicipital groove of the humerus.1,2 The continuum of clinical pathology ranges from acute inflammatory tendonitis to degenerative tendinopathy.1,2 Without the use of imaging, LHBT pathology is typically diagnosed through a combination of patient identified location, palpation, special tests and other provocative maneuvers.24 The term manual therapy was defined as skilled hand movements and skilled passive movements of joints and soft tissue intended to improve tissue extensibility; increase range of motion; induce relaxation; mobilize or manipulate soft tissue and joints; modulate pain; and reduce soft tissue swelling, inflammation, or restriction. Techniques may include manual lymphatic drainage, manual traction, massage, mobilization/manipulation, and passive range of motion.25 Manual therapy was also defined in terms of non-thrust manipulation (mobilization) or thrust manipulation. Non-thrust manipulation was defined as a passive procedure which involves a low velocity, low to high amplitude force to a targeted region which is modified based on clinician assessment and patient feedback; thrust manipulation was defined as a passive procedure which involves a high velocity, low amplitude force to a targeted region which is modified based on clinician assessment and patient feedback.25 The term intervention was defined as the purposeful interaction of the physical therapist with an individual to produce changes in the condition that are consistent with the diagnosis and prognosis.25 Lastly, the term biophysical agents was defined as a broad group of agents that use various forms of energy and are intended to assist muscle force generation and contraction; decrease unwanted muscular activity; increase the rate of healing of open wounds and soft tissue; maintain strength after injury or surgery; modulate or decrease pain; reduce or eliminate edema; improve circulation; decrease inflammation, connective tissue extensibility, or restriction associated with musculoskeletal injury or circulatory dysfunction; increase joint mobility, muscle performance, and neuromuscular performance; increase tissue perfusion and remodel scar tissue; and treat skin conditions.25 Subsequent rounds were used to reach a consensus among reported recommendations while incorporating modifications and inclusion of new items.
Round II of Delphi
From the qualitative analysis of responses from Round I, themes were identified and subsequently coded to present themes in Round II. A qualitative, thematic analysis approach was used to interpret, construct, and develop themes summarizing the participants’ recommended interventions.26,27 Using this approach, thematic interpretations remain close to participants’ words. Themes and subthemes were identified and subsequently coded by A.M. and L.C. and disputes were settled by S.A. The purpose of Round II was to achieve consensus on intervention strategies identified in Round I. Additionally, Round II included questions regarding the stage of healing (acuity) in which each intervention would be utilized. Identified themes and subthemes included: Resistance Exercise/Muscle Performance (subthemes: tendon loading techniques, progressive resistance exercises, open/closed kinetic chain exercises, task specific/functional activities), Stretching and Flexibility, Manual Therapy (subthemes: non-thrust manipulation, thrust manipulation, soft tissue techniques), Patient Education, Biophysical Agents, Dry Needling, Other and Treatment Statements. Questions were organized using a 4-point Likert scale ranging from 1 (“strongly agree”) to 4 (“strongly disagree”). Participants were also asked to rate through multiple choice questions, the stage(s) of tissue healing they would recommend each intervention be used with options of “acute”, “subacute”, “chronic”, or “I would not use or recommend this intervention”. Common definitions of the stages of healing were included again for standardization.28 Finally, respondents were asked to report their level of agreement with statements regarding clinical decision making (which resulted from Round 1 open ended statements) pertaining to treating individuals with LHBT tendinopathy using the Likert scale described above.
Round III of Delphi
The questionnaire for Round III contained the same questions that were presented in Round II, including all definitions, intervention techniques, and stages of acuity. Each question was accompanied by tables and figures illustrating the results of Round II. The respondents were asked to review the feedback from Round II and rescore each intervention.
Data Analysis
The survey instrument was built on Qualtrics survey software (Qualtrics, Provo, UT). After Round I was complete, data were exported from Qualtrics to an excel sheet for analysis. Three investigators completed the theme and coding synthesis process individually. The 3 investigators (A.M., L.C., and S.A.) then came together to reach consensus for themes to advance into Round II. After the completion of Round III, data were exported from Qualtrics to an excel sheet for further analysis by the workgroup. For Round III, a benchmark of ≥75% agreement as an a priori cutoff was utilized, as seen in similar study designs.23,29 Recommendations rated as 3 (disagree) or 4 (strongly disagree) by ≥75% of the panelists were collapsed into “disagree” and not considered recommended interventions. Intervention recommendations rated as a 1 (strongly agree) or 2 (agree) by ≥75% of the panelists were collapsed into “agree” and included as recommended in the final consensus. Scores were tallied for each intervention including the frequency of respondents and corresponding percentages.
RESULTS
Respondent Characteristics
A total of 136 potential participants were contacted via email. Ten potential participants had email addresses that were currently not active, leaving 126 eligible participants. One expert declined to participate due to a disagreement in the definition of biceps tendinopathy utilized in our study. One hundred and five experts did not respond to the invitation to participate or the reminders. Thirty-one (24.6%) participants completed the consent form and responded to Round I (Figure 1). The respondent group consisted of experts from the United States (n = 19), United Kingdom (n=2), Australia (n=2), Sweden (n=2) and one from each of the following countries: Spain, New Zealand, Turkey, Canada, Italy, and the Netherlands. Thirteen respondents were female (41.9%), eighteen were male (58.1%), and 0% responded as non-binary. Respondents had a variety of degrees, including Masters, Doctorate, Doctor of Science (DSc), and Doctor of Philosophy (PhD), in addition to other specialty certifications. Twenty-six of 31 (83.9%) of the respondents in Round I were clinicians. Of those clinicians, fifteen (48.4%) had 20 or more years of clinical practice. Twenty-seven of 31 respondents (87.1%) consented to be acknowledged for their participation (Table 1).
Round I
Comments from Round 1 were summarized and statements containing similar constructs were grouped and reduced for each theme. For example, the following five items were originally included in the list of statements for Round 1: 1) common and effective interventions used to treat LHBT tendinopathy 2) common and effective exercise-based interventions used to treat LHBT tendinopathy 3) common and effective manual therapy-based interventions used to treat LHBT tendinopathy 4) common and effective biophysical agents used to treat LHBT tendinopathy 5) other common and effective interventions used to treat LHBT tendinopathy. Across all five item categories, 217 initial statements from the open-ended responses specific to physical therapy interventions were provided in Round 1 and condensed into 47 intervention-based statements across eight newly formed themes (resistance exercise/muscle performance, stretching and flexibility, manual therapy, patient education, biophysical agents, other, dry needling, and treatment statements).
Rounds II and III
One respondent did not complete the survey from Round II despite weekly reminders; therefore 30 of 31 of the respondents participated in Round II (96.7% retention rate between Round I and Round II; Figure 1). Retention rates for respondents were reduced from 30 to 29 from Round II to Round III (96.6% retention rate between Round II and Round III); (Figure 1). Twenty-nine respondents completed Round III (93.5% retention rate between Round I and Round III). A detailed description of consensus for “agree” and “disagree” per intervention category for Round III is reported beginning with Table 2.
Intervention Themes
Resistance exercise/muscle performance
Among respondents there was strong consensus in favor of tendon loading techniques as an effective intervention for treating individuals with LHBT tendinopathy. Consensus “agree” was reached for five of five tendon loading techniques in Round II and Round III (Table 2). Respondents reached consensus “agree” that progressive resistance exercises would be prescribed for nine of 11 muscles/muscle groups not including upper trapezius and pectoralis major muscles. Consensus “agree” was also established across six of six open and closed chain kinetic chain exercises including minimal change in consensus between Rounds II and III. Task specific functional activities (reaching, lifting, overhead activity, and occupation and sport specific tasks) reached consensus “agree” with all respondents in Round II and III (Table 2).
Stretching/flexibility
Respondents demonstrated consensus “agree” in favor of stretching/flexibility for five of seven identified muscles/muscle groups in Round II increasing to seven of seven muscles/muscle groups in Round III with four participants changing to agree in Round III to include upper trapezius as a target muscle for stretching (Table 2).
Manual Therapy
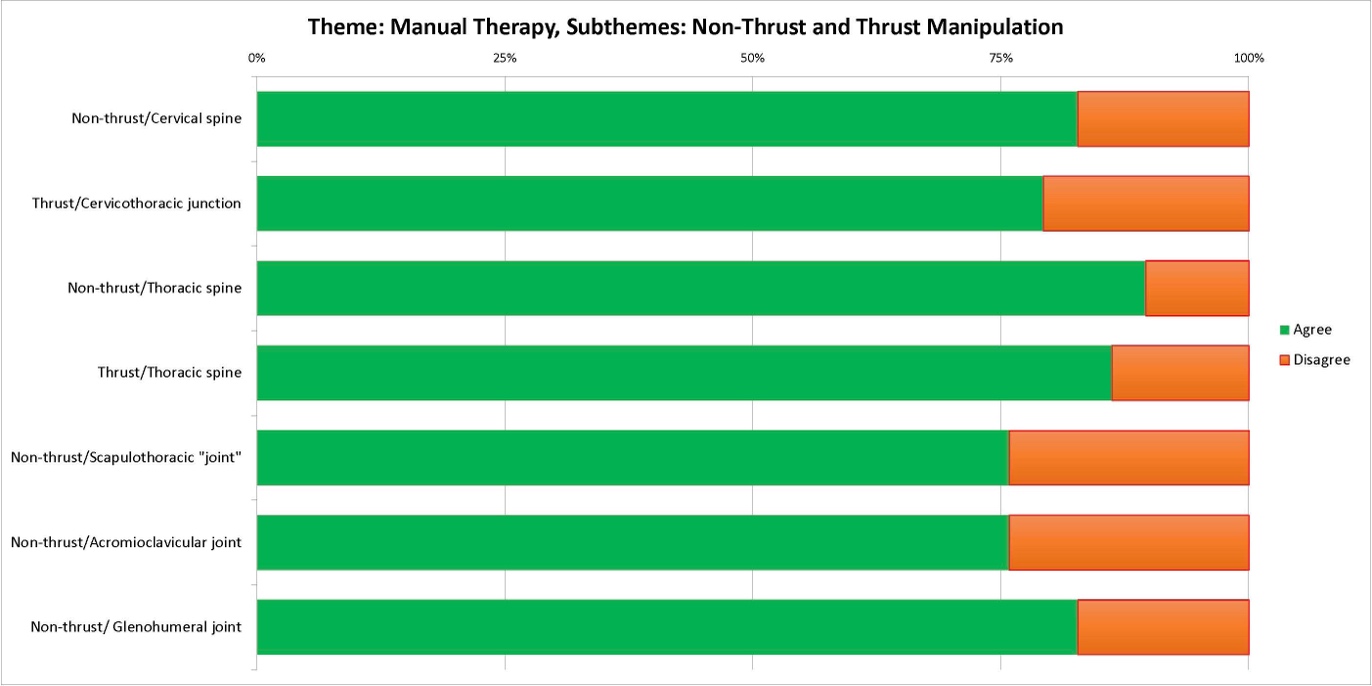
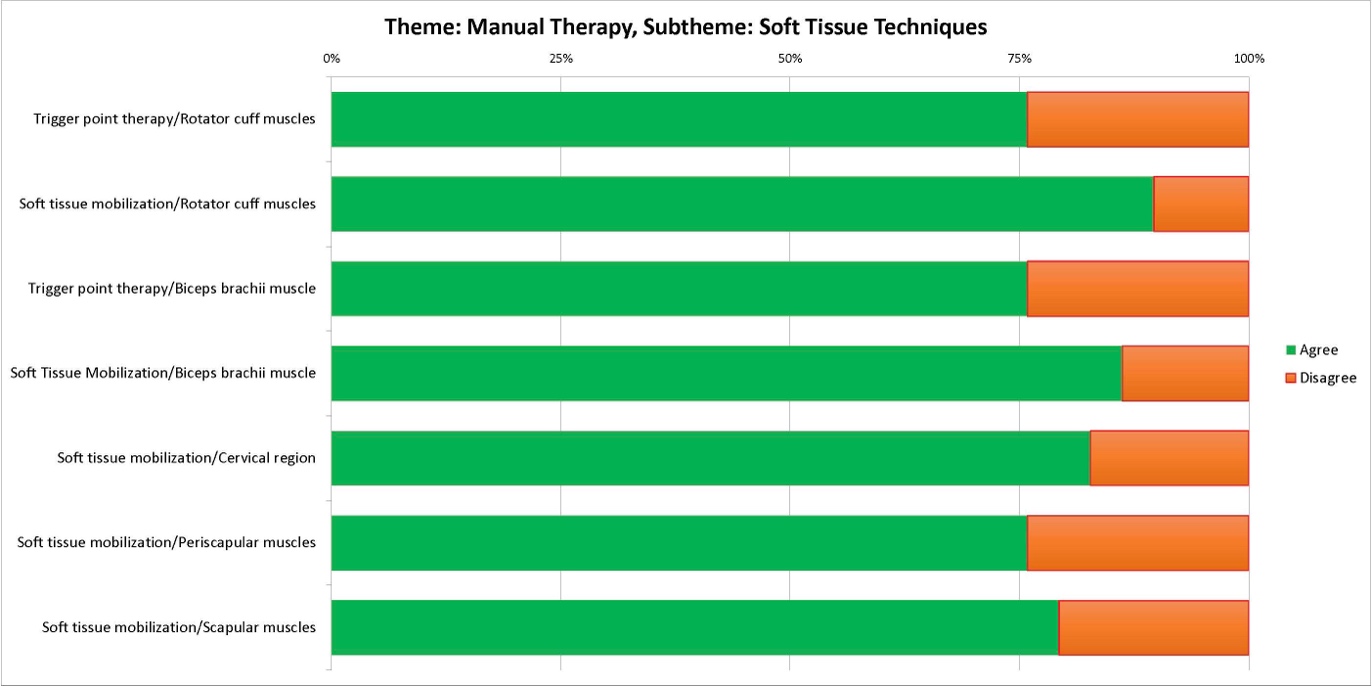
Non-thrust manipulation techniques (five of five) achieved consensus “agree” by respondents in Round III with techniques to the acromioclavicular joint and scapulothoracic joints not reaching the threshold for agreement by respondents in Round II. Four thrust manipulation techniques were included in the questionnaire with only two of four regions (thoracic spine and cervicothoracic junction) achieving overall consensus “agree” by respondents in Round III (Table 3 and Figure 2). Intervention to the thoracic spine region received the highest level of consensus “agree” in both non-thrust and thrust manipulation techniques; 89.65% and 83.34% respectively in Round III. Specific thrust and non-thrust manipulation techniques included Grade I-II and Grade III-IV non-thrust, Grade V thrust and mobilization with movement (MWM) all of which achieved consensus “agree” in Round II and III. Soft tissue techniques were included in the manual therapy category and two of 11 techniques (soft tissue mobilization of the biceps brachii and trigger point therapy to the rotator cuff muscles) achieved consensus “agree” in Round II compared to seven of 11 techniques in Round III. All other soft tissue techniques to specified regions (six of 11) did not reach consensus for “agree” or “disagree” (Table 3 and Figure 3).


Patient Education
Patient education concepts related to advice achieved eight of eight consensus “agree” in Round III. Concepts that achieved 100% consensus included: activity and occupational modification, training/loading modification and education surrounding the PT treatment plan and pain neuroscience education (Table 4).
Biophysical Agents
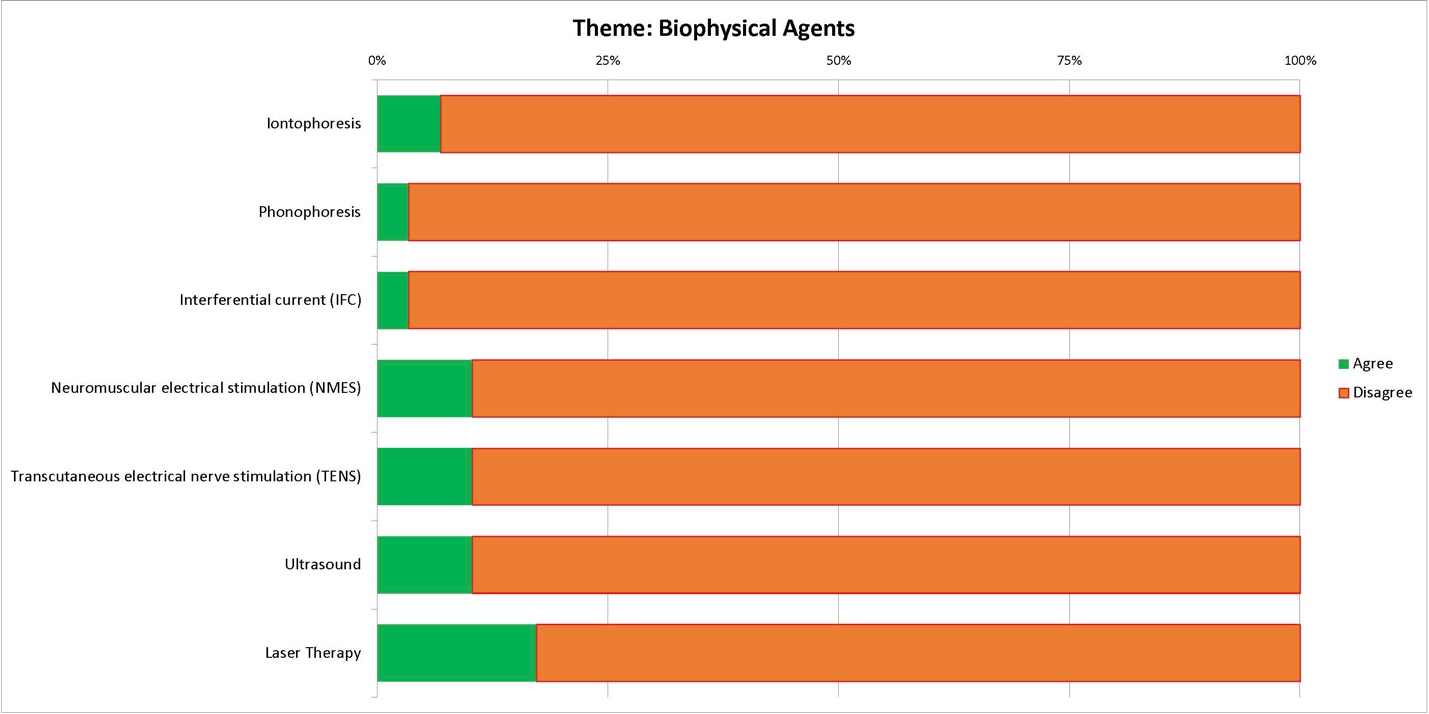
Respondents reached consensus “disagree” on seven of nine biophysical agents including iontophoresis, phonophoresis, three forms of electrical stimulation, ultrasound and low-level laser therapy (LLLT), (Table 4 and Figure 4). Therefore, thermal agents including cryotherapy and moist heat did not reach consensus agree or disagree. Additionally, there was no change in consensus “agree” in the seven of nine categories between Round II and Round III.

Dry Needling
Among respondents there was consensus “agree” on dry needling to the biceps brachii muscle in Round II and Round III. In Round II respondents reached consensus “agree” on needling the rotator cuff muscles but consensus “agree” was not achieved in Round III (Table 4).
Other
The other category included additional interventions that respondents commented on by providing free text answers to open-ended questions in Round I. Respondents reached consensus “agree” on two of five items to include cognitive behavioral therapy and non-steroidal anti-inflammatory drugs (NSAIDs) and consensus “disagree” on two of five items including extracorporeal shock wave therapy (ESWT) and dry cupping therapy (Table 4).
Treatment Statements
Respondents reported their level of agreement with treatment-based statements in terms of intervention (which resulted from Round 1 open ended questions) and consensus “agree” was reached in six of eight statements with one statement (clinical decision making should be prescriptive) reaching consensus “disagree” and the other reaching non consensus (Table 5). Statements that were consensus “agree” included utilization of a pragmatic and multimodal approach to intervention following clinical practice guidelines when available. Additional statements are included in Table 5.
DISCUSSION
The primary purpose of this Delphi study was to identify experts in the PT management of shoulder pain and utilize their experience and expertise to identify interventions that are common and effective in treating individuals with LHBT tendinopathy. For the 29 expert respondents who contributed to the final results, findings demonstrated that 61/86 interventions across seven intervention themes met the criteria of 75% consensus of being effective for the treatment of LHBT tendinopathy; conversely, 9/86 interventions across seven themes reached a 75% consensus of being ineffective for the treatment of LHBT tendinopathy. These findings suggest there are several physical therapy interventions across multiple intervention themes (with high consensus) including resistance exercise, stretching and flexibility, manual therapy, and patient education that are recommended by experts to treat individuals with LHBT tendinopathy. These interventions may serve as a proposed guideline of interventions to be investigated in clinical trials and trialed with patients clinically due to a lack of additional evidence to guide optimal management.
One noteworthy finding was the overall high consensus with the intervention of exercise including the themes of resistance exercise/muscle performance and stretching/flexibility and subthemes of tendon loading techniques (including isometrics, concentric and eccentrics), progressive resistance exercises, open/closed kinetic chain exercises and task-specific functional activities (Table 2). These findings are not surprising considering strong recommendations in the literature for including exercise therapy as the first-line treatment to improve pain, mobility, and function in patients with subacromial shoulder pain.30 Studies specific to tendinopathies describe exercise therapy, specifically eccentric exercise, as an effective component of an exercise program in treating individuals with tendinopathy.31–33 Respondents agreed that “progressive loading of the LHBT should be matched to tissue capacity and pain severity/irritability” based on consensus with those treatment statements, combined with a consensus on the recommendation of five of five tendon loading techniques. Respondents also demonstrated consensus on nine of 11 progressive resistance exercises, and consensus on all interventions in the theme of stretching/flexibility and subthemes of open/closed kinetic chain exercises and task-specific functional activities. Krupp and colleagues3 state that a comprehensive rehabilitation program should focus on restoring dynamic stability to the shoulder and rehabilitation may vary depending on clinical presentation. Further, according to Krupp et al.3 patients may progress through four phases (pain management and restoration of range of motion (ROM), active range of motion (AROM) and early strengthening, rotator cuff and periscapular strengthening, return to sport) which may explain why respondents recommended 32 of 34 exercise interventions and included the use of exercise interventions across all stages of tissue healing (acute, subacute, chronic).
A second noteworthy finding was the lack of agreement among respondents on interventions within the dry needling theme and the manual therapy subthemes of thrust manipulation and soft tissue techniques (Table 3). Respondents reached consensus on non-thrust manipulation interventions to the glenohumeral joint, cervical and thoracic spines, scapulothoracic and acromioclavicular joints and thrust manipulation interventions to the cervicothoracic regions (Figure 2) but did not meet the a priori consensus of 75% for thrust manipulation of the glenohumeral joint or cervical spine. Therefore, it is possible the respondents were familiar with literature surrounding manual therapy interventions known to be more effective in treating individuals with shoulder pain. Well described in the literature are the effects of cervicothoracic and thoracic manipulation in individuals with shoulder pain34,35 demonstrating findings of reduced pain and disability immediately and up to 52 weeks.36,37 However, there is overall less evidence to support thrust manipulation to the cervical spine and glenohumeral joint for the management of shoulder pain. Respondents did not reach consensus on instrumented soft tissue mobilization or deep transverse friction techniques (Table 3). Deep transverse friction techniques have been recommended for the treatment of various tendinopathies,38,39 however, evidence is anecdotal40 and the authors are not aware of studies investigating these techniques specifically for treating individuals with LHBT tendinopathy. The subtheme of dry needling did not reach consensus on four of five interventions, with dry needling to the biceps brachii muscle being the only intervention reaching consensus (Table 4). Recent research recommends needling for the treatment of tendinopathy,41–43 but only a single case series specific to dry needling of the LHBT for the treatment of LHBT tendinopathy was identified.21
A third notable finding was the consensus “disagree” in the theme of biophysical agents on seven of nine items including iontophoresis, phonophoresis, electrical stimulation (interferential current, neuromuscular electrical stimulation and transcutaneous electrical nerve stimulation), ultrasound, and low-level laser (Figure 4). In the theme of other there was also consensus “disagree” on shock wave therapy. Findings from a recent review of systematic reviews, specific to tendinopathies, found moderate-quality evidence to support the use of low level laser for pain and disability in the short-term and shock wave therapies showed a statistically significant improvement in pain and function at all follow-up periods.33 However, the opinion persists that most of the available therapeutic modalities are only supported by weak evidence44 with moderate evidence of no effect for interventions, such as laser therapy, extracorporeal shockwave therapy, pulsed electromagnetic energy, and ultrasound.30 Additionally, based on the systematic review of the literature performed prior to the study, only low quality randomized controlled trials exist specifically outlining meaningful improvements using biophysical agents to treat LHBT tendinopathy.
Overall, the pooled recommendations of the respondents are consistent with current recommendations that a multimodal approach is optimal for the management of shoulder pain.37,45–48 Physical therapy management of LHBT tendinopathy may involve a multimodal approach addressing associated impairments of the shoulder, scapular region and cervicothoracic spine with the application of exercise, joint and soft tissue mobilization as well as retraining dysfunctional movement patterns.3 As such, the respondents reached consensus on a number of interventions across different themes and subthemes supporting a multimodal approach to treatment. Preliminary evidence on the PT management of LHBT tendinopathy is not robust enough to draw strong conclusions1,2,13,16,19–21 and few studies focus on a multimodal approach. Therefore, obtaining international expert consensus on a multimodal treatment approach further informs treatment recommendations, which could potentially be utilized prior to electing for surgical options. Surgery (biceps tenodesis) may be a safe option and may offer a satisfactory rate of return to sport in young athletes,4 however, according to Frank et al.49,50 there is an increased risk of surgical revision in athletes under 20 years old with a history of throwing activity. Therefore, based on the results of this Delphi study conservative PT based management prior to individuals electing for more aggressive surgical intervention for the management of LHBT tendinopathy may be recommended based on these expert opinions.
Limitations
There were several limitations to this Delphi study. First, the respondents included in this study were those willing to participate and may not reflect all clinicians and researchers with expertise in treating shoulder pathologies. Additionally, the respondent group consisted of individuals from various countries. Although this diversity was also seen as a strength, the definitions that were used in this study may not have been commonly used by all respondents. Further, the views of the Delphi panelists may differ from other content experts who declined the offer to participate in the study, thus the expressed opinions may not be fully representative of all experts in the field. Further, any recommendations made as a result of this Delphi, warrant further investigation in trials as evidence of effectiveness of the recommended interventions is still lacking in this specific patient population.
CONCLUSION
The results of this study highlight the current absence of well-defined, PT interventions used to treat LHBT tendinopathy. Expert respondents reached consensus that a multimodal approach including exercise, manual therapy and patient education could be used to manage LHBT tendinopathy. Given the chronic nature of the condition combined with the lack of established guidelines for PT intervention, future research is needed to guide physical therapists who manage the condition.
Conflicts of interest
All authors do not have conflicts of interest to report.
Grant Support
This work was supported by The American Academy of Orthopedic Manual Physical Therapists (AAOMPT) under a grant from Cardon Rehabilitation (Ontario, Canada). Neither AAOMPT nor the funding agency had any role in the study design, analysis, interpretation, or decisions about publication.
Acknowledgements
The authors would like to thank all the respondents who participated in the study. The authors would like to thank Cardon Rehab (Ontario, Canada) and the American Academy of Orthopaedic Manual Physical Therapists for the Cardon Research Grant which supported this work.