
INTRODUCTION
The vastus medialis (VM) and vastus lateralis (VL) form part of the quadriceps femoris group in the anterior thigh. A balance between these two muscles is key to maintaining normal tracking of the patella in the trochlear groove during flexion and extension of the knee joint.1,2
The vastus medialis is located in the medial part of the thigh, and, though controversial, is generally agreed to consist of two components: the more proximal vastus medialis longus (VML) and the distal vastus medialis oblique (VMO).3–5 The VMO inserts at the medial border of the patella.
Like the VM, the VL is also considered to comprise two components: the vastus lateralis oblique (VLO) and vastus lateralis longus (VLL)6–8 due to differences in their muscle fiber orientations. The VLO is analogous to the VMO in that it is orientated more horizontally at the patella.6,9 While the VMO has been the subject of much research interest, there is less in the literature regarding the VL. However, studies have been carried out, particularly using electromyography, investigating both the VMO and the VL10–13 and their respective roles in maintaining patellar alignment both in normal individuals, and in patients presenting with patellofemoral pain (PFP).
The etiology of patellofemoral pain is known to be multifactorial14 and may be due to pathology or abnormalities in the regional anatomy,15 regional myofascial restrictions,16 or an imbalance between the contraction of the VMO and the VL, resulting in patellar maltracking.17 The condition is most prevalent in young, athletic individuals, with females being more affected than males.18 Treatment options for PFP include physiotherapy aimed at strengthening the VM, where VMO insufficiency is implicated, stretching exercises targeting the VL in cases of VL hypertrophy, or myofascial release where myofascial restrictions are identified.16 Previous studies have shown that it is possible to manipulate the pennation angle of the VMO and VL, either increasing the fiber angle with targeted exercises19,20 or reducing the angle by stretching,21 which has obvious implications for patellar tracking.
Self-myofascial release (SMR) is a technique to reduce fascial tightening by stretching it. It is commonly performed by using a roller to apply sustained pressure to the muscle. Studies on SMR have found that foam rolling increases joint range of motion (ROM) and reduces delayed onset muscle soreness before and after exercise.22–24 There is, however, a paucity of information in the literature regarding its effect on muscle architecture. Indeed, while acknowledging the effectiveness of SMR for increasing joint range of motion, Cornell & Ebersoll25 recommended the use of ultrasound to further investigate the changes brought about by acute SMR. The aim of this study, therefore, was to explore the effects of SMR by investigating changes in the fiber angles of the VMO and VL following a seven-week program of SMR using a foam roller. Ultrasound is a safe, validated, non-invasive technique that has been used extensively to investigate the architecture of the hamstrings26 and quadriceps.19,27–30
MATERIALS AND METHODS
This study received ethical approval from St George’s, University of London Ethics Committee. Participants were recruited from the University sports and athletics teams. Twenty-five young, athletic males volunteered and gave informed consent. A power calculation showed that a minimum group size of twenty-three would be needed to achieve statistical significance. Inclusion criteria were: male, age 18-35, no current knee pathology, no previous knee surgery, and a Tegner activity score ≥4.31 Using a male-only cohort provided a homogeneous sample, removing the confounding factor of sex difference. Males also have less subcutaneous fat,32 improving echogenicity of the muscle underneath.33
The volunteers underwent an initial ultrasound scan of the VMO and VL, then undertook a seven-week program of SMR, and were then re-scanned. One individual was selected at random for the intra-rater reliability study. This individual did not take part in the SMR program, and was scanned by the same operator, using the same ultrasound method, on eight different occasions during the study period.
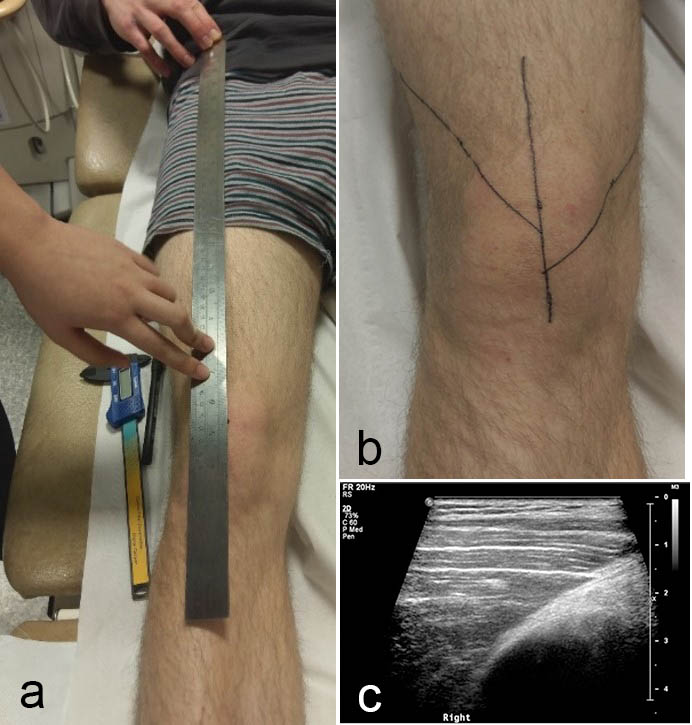
The subjects lay supine on an examination couch, with a pillow under the ankles for support. The mid-point of the patella was found using Duratool digital calipers (Duratool Corporation, Taichung City, Taiwan) and marked. A steel ruler was placed between the mid-point of the patella and the ASIS, and the femoral axis was then marked on the skin (Fig. 1a). The pennation angles of the VMO and VL were then measured on both lower limbs in turn (Fig. 1b), using a Philips iU22 ultrasound scanner with a L17-5 linear array probe (Fig. 1c). All measurements were taken by the same operator, using the same equipment. Measurements were taken three times, then averaged.
__vmo_and_vl_fibre_angles_were_identified_and_m.jpg)
Following the initial scan, volunteers commenced the seven-week SMR procedure using a 15 cm x 45 cm foam roller (PhysioRoom.Com Limited, Burnley, UK). The foam roller was to be used three times weekly, on three separate days, independent of exercise. The roller was placed under the proximal aspect of the anterior thigh while the subject was in the prone position with elbows on the ground. The contralateral limb was placed on top of the other limb (Fig. 2). Using their elbows, the subject then pushed himself back and forth so that the foam roller moved along the length of the anterior aspect of the thigh, from the top of the thigh to the upper border of the patella. Each motion was to be completed in no more than two seconds. This procedure was performed for one minute, and then repeated on the other thigh. A compliance diary was provided to monitor the subject’s activities.

On completion of the seven-week SMR program, the ultrasound scans were repeated.
RESULTS
Intra-Rater Reliability Study
The results of the intra-rater reliability study indicate good overall reliability of the measurements (Table 1). There was a substantial difference in the fiber angle of the VMO and the VL. The mean fiber angle of the combined right and left VMO was 63.8°, and the mean fiber angle of the combined right and left VL was 33.8°.
After seven weeks of SMR, there was a significant decrease of 7.0° (±9.73) and 8.21° (±10.53) in the pennation angles of the right and left VMO, respectively (p<0.001) (Table 2).
After seven weeks of SMR there was a significant decrease of 6.58° (±5.58) and 6.71° (±5.45) in the pennation angles of the right and left VL, respectively (p<0.001) (Table 3).
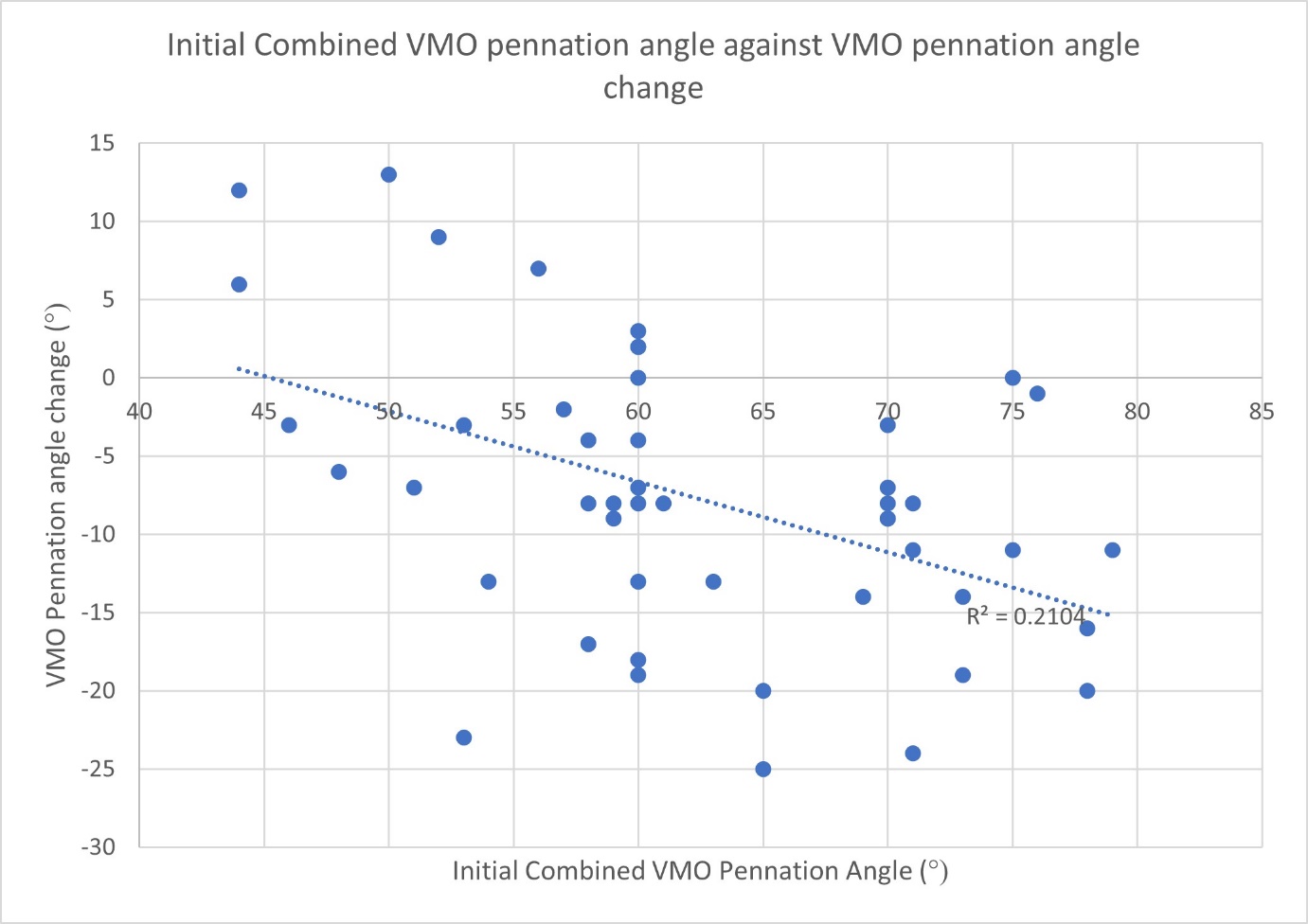
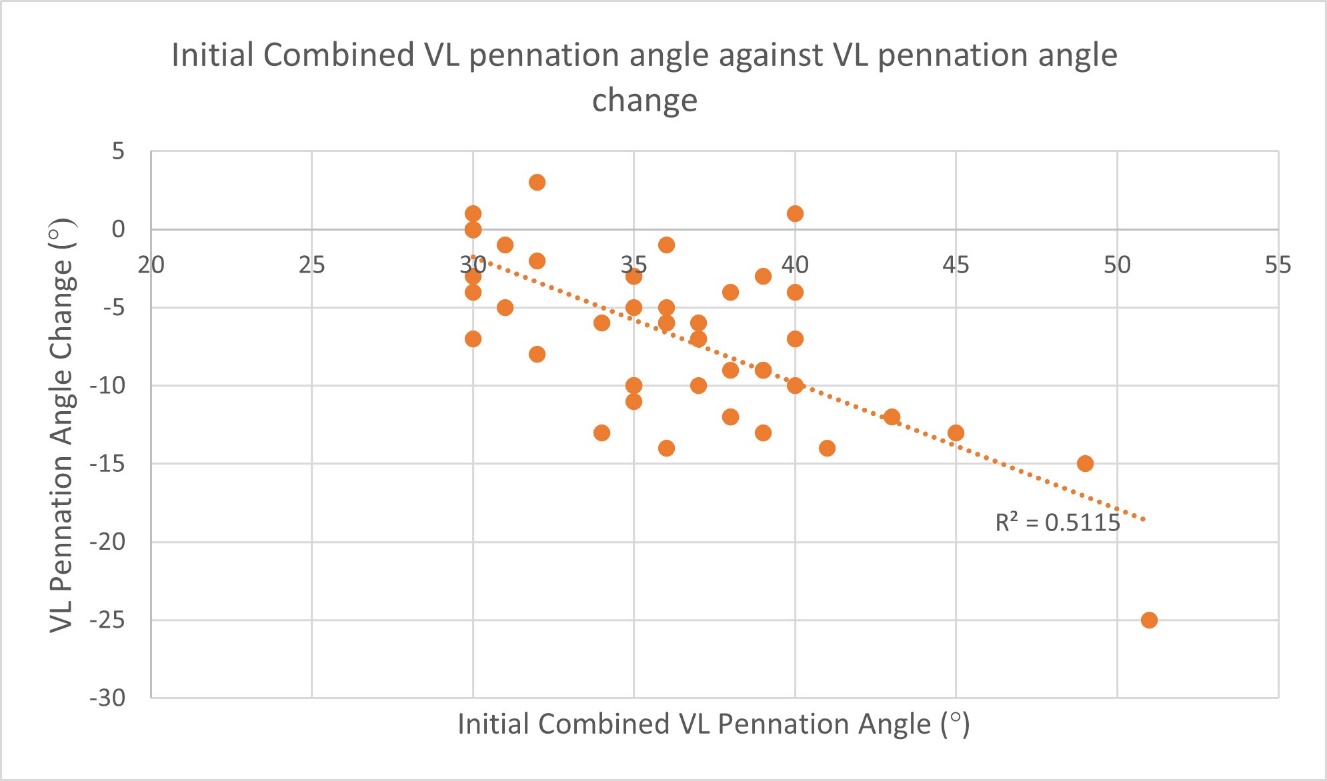
There was a weak and non-significant inverse correlation between mean initial combined left and right VMO fiber angle and VMO fiber angle change after seven weeks of SMR (Rsquared = -0.2104, p=0.15) (Fig. 3). There was a stronger inverse correlation between mean initial combined VL fiber angle and VL fiber angle change (Rsquared = -0.5115, p<0.001) (Fig. 4).


The average compliance recorded by the participants was 82%, i.e., the SMR was carried out on average 2.46 times per week by each participant.
DISCUSSION
Patellar maltracking due to an imbalance between the VMO and VL is thought to be a contributor to the etiology of PFP.2,15 There is a high prevalence of PFP (also known as ‘runner’s knee’) among young athletic individuals, where the problem may be due to VMO insufficiency or a hypertrophied VL. Where myofascial tightness in the anterior thigh is suspected, SMR may be recommended in order to improve flexibility and increase range of motion of the knee and hip.16
While several studies have shown that SMR improves joint range of motion, vascular endothelial function, flexibility, and delayed onset muscle soreness (DOMS) in athletic individuals,22,34,35 there is currently no information in the literature on the effect of SMR on the architecture of the VMO or VL, either in in asymptomatic individuals, or in patients presenting with PFP.
The study reported here has shown that seven weeks of SMR using a foam roller resulted in a statistically significant reduction (p<0.001) in the pennation angles of the VMO and VL in both lower limbs. There was a greater overall percentage change for the VL (-18%) than the VMO (-11.5%), which tends to suggest that the SMR had a greater effect on the architecture of the VL than that of the VMO. This may have been due to the fact that the VL extends further along the length of the anterior thigh than does the VM, and hence was affected more by the SMR, because the subjects were required to roll from the top of the thigh down to the top of the knee.
Although the subjects in this study were all asymptomatic, they were drawn from the demographic at high risk of developing PFP. The architectural changes to the VMO and VL provides clinical evidence that SMR could be effective in myofascial release in young athletic males presenting with PFP. Furthermore, a patient’s progress could be easily monitored in clinic by ultrasound scans using the method described here. However, it should be borne in mind that the subjects in this study were all asymptomatic, and, while the results were statistically significant, the clinical significance of these results is not clear: further work is needed to assess the effects of SMR on muscle architecture in patients presenting with PFP.
Interestingly, there was only a weak negative correlation between the initial VMO fiber angle and the degree of change in VMO fiber angle (Rsquared = -0.21), suggesting that the initial VMO fiber angle is relatively unimportant in the likely outcome of the treatment. This is in contrast with exercises to strengthen the VMO, where a low initial fiber angle has been shown to be predictive of a greater increase in post-exercise fiber angle.31 There was a stronger negative correlation between initial VL fiber angle and change (Rsquared= -0.51), which suggests that, in cases of VL hypertrophy, patients who would benefit most from SMR might be identified in clinic by a preliminary ultrasound scan.
There are some limitations to note in this study. Although volunteers were provided with a compliance diary to encourage participation, there was inevitably some variation in actual compliance. Some volunteers found initial use of the foam roller to be painful, which affected their compliance. Also, as the volunteers all took part in sports activities, some may have performed other quadriceps stretches throughout the seven-week period, which could have affected the fiber angles. Participants of this study all took part in various sports and exercise with differing levels of intensity (basketball, rugby, athletics, and cycling), which could have affected the outcomes. It would be useful to repeat this study on individuals who all participate in the same sport.
Conclusion
The results of this study indicate that seven weeks of SMR using a foam roller resulted in a statistically significant decrease the pennation angles of the VMO and VL in both limbs. There was, however, a greater percentage decrease in the angle of the VL. There was a moderate negative correlation between initial VL fiber angle and fiber angle change. These findings may provide information to help guide physiotherapy interventions for patients presenting with anterior knee pain.
Acknowledgements
The authors confirm that they have no conflicts of interest to declare. The study was internally funded by St George’s, University of London.