
INTRODUCTION
Quadriceps strength is essential in both the healthy and rehabilitating knee, and can be quantified by measuring muscle torque using isometric dynamometry.1–4 The assessment of isolated quadriceps strength serves as an important indicator of recovery and is commonly used in combination with physical performance testing to guide the decision making process for return to sport.5,6 Strength deficits following knee surgery are commonly observed and have been implicated in poorer self-reported function, gait, return to sport, athletic performance, and may lead to the development of osteoarthritis, or secondary injuries.7–15 Previous authors have advocated for minimum thresholds for quadriceps symmetry prior to returning to sport after ACL reconstruction.16,17
A variety of factors contribute to muscular strength, including genetic, developmental, endocrine, and physical activity considerations.18–21 While many of these variables are subject to change throughout one’s adult life, long bone length, and limb length remain relatively stable. Previous studies have reported that there was a significant correlation between both height, weight, and isometric quadriceps strength.22,23 However, the role of bony morphology, specifically lower extremity limb length, has scarcely been evaluated with respect to a relationship with measurements of lower extremity muscular strength.
Previous authors have demonstrated that utilization of a tape measure from the anterior superior iliac spine to the medial malleolus demonstrates excellent reliability with limb length measurements compared to anterior-posterior full-length weightbearing radiographs.24 This measurement technique allows for the opportunity to obtain accurate limb length measurements in the clinical setting without necessitating full-length weightbearing radiographs to determine true limb length. Therefore, the purpose of this study was to evaluate the relationship between lower extremity length, including tibia and femur length measured radiographically, and isometric quadriceps strength in patients undergoing knee surgery. The null hypothesis was that there would be no correlation between lower extremity length and isometric quadriceps strength.
METHODS
Prior to patient enrollment, the study protocol was approved by an external institutional review board (IRB) through two separate IRB protocols. Consent to participate was obtained for each IRB protocol with in-person documentation. The first IRB protocol considered the collection of lower extremity radiographs at clinic visits (#07.24.2019), while the second IRB protocol considered the collection of isometric quadriceps strength data in the biomechanical testing facility (#10.21.2019_RL_Complex Knee). Patients from a single knee surgeon’s practice were prospectively enrolled from June 2019 until February 2020. Inclusion criteria included patients from a single knee surgeon’s practice that underwent knee surgery, who were ≥14 years and ≤65 years of age, and who obtained full length anterior-posterior weightbearing radiographs. Patients with ligamentous, meniscal, or cartilage pathologies were included. Additionally, all patients completed performance testing at a single biomechanical testing facility, using the same dynamometer (Biodex Medical Systems, Inc., Shirley, NY). Patients were excluded if they were unable to complete testing, did not obtain full length weightbearing radiographs, radiographs did not visualize the necessary anatomical landmarks (ASIS, medial malleolus, center of the femoral head, roof of the notch, center of the tibial plateau; n=2), patient was unable to bear weight, or had undergone a previous lower extremity osteotomy. Additionally, individual patient limbs were excluded from the non-operative cohort if contralateral autografts were harvested (n=2). All new patients routinely obtained long leg alignment radiographs in the senior author’s practice. Both the injured limb and the non-injured contralateral limb were used for analysis. Quadriceps strength testing was performed at a single time-point post-operatively; this time-point was six months after ligamentous, meniscal repair, and cartilage surgeries and four months after basic knee arthroscopies.5 Weightbearing status was recorded as either weightbearing or non-weightbearing for the first six weeks following surgical intervention. Patients that underwent revision ligament reconstruction, posterior cruciate ligament reconstruction, osteochondral allograft reconstruction, isolated meniscal repair and transtibial meniscus radial or root repairs were all non-weightbearing. Primary and revision anterior cruciate ligament reconstructions with or without peripheral meniscal repairs, and diagnostic arthroscopies were allowed to weight bear immediately following surgery.
Radiograph measurement technique
All radiographic measurements were obtained from full length weightbearing anterior-posterior x-rays. These images were obtained using three to four individual images on a 432 cm x 43.2 cm vertical digital detector. The x-ray beam was centered at the knee at a distance of 182.9 cm. Twenty-five-millimeter sizing balls were utilized to normalize the radiographs for accurate measurements. The beam was angled independently for each shot from the hip to the ankle, with distortion corrected by processing algorithms.
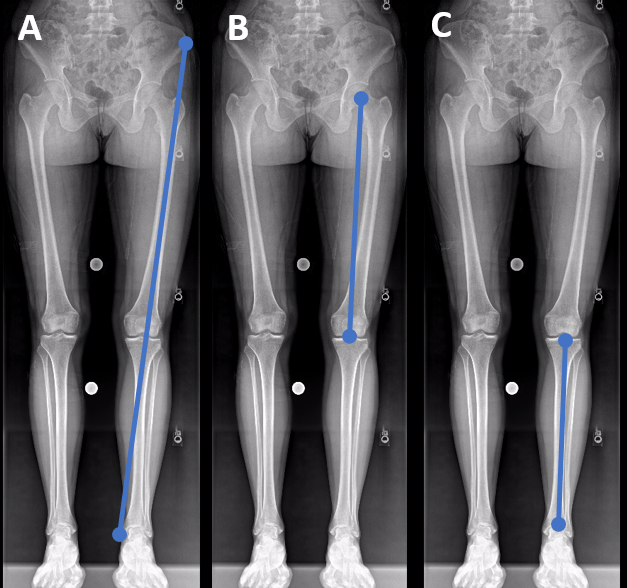
The length of the tibia was measured from the center of the tibial plateau, between the middle of the tibial eminences, down to the center of the most distal aspect of the tibial plafond. The femur length was measured from the center of the femoral head down to the joint line. Finally, total limb length was measured from the inferior aspect of the anterior superior iliac spine (ASIS) down to the most prominent point of the medial malleolus in a technique that was previously described (Figure 1).25,26 For the assessment of limb length correlation with strength deficit, an average of the surgical and non-surgical limb length was used for analysis.

This figure depicts the measurement strategies utilized on full-length weightbearing radiographs. The image on the left (A) demonstrates to full limb length measurement: from the inferior aspect of the ASIS to the most prominent aspect of the medial malleolus. The middle image (B) depicts the measurement technique for the femur: from the center of the femoral head to the trochlea point at the top of the notch. The right image (C) demonstrated the measurement technique for the tibia: from the center of the tibial plateau to the center of the tibial plafond.
Quadriceps Strength Testing
Quadriceps strength testing was performed at a single biomechanical testing facility, using the same dynamometer (Biodex Medical Systems, Inc., Shirley, NY) for all patients. Patients were seated on the machine with legs flexed to 90° and their back kept straight. Prior to testing, anatomical landmarks were identified. The operators ensured that the lateral femoral condyle was aligned with the dynamometer’s axis of rotation, and also that the forced arm was secured just superior to the lateral malleolus. Thigh, waist, and two chest straps were used to secure the patient to the chair.

This figure demonstrates the setup for quadriceps strength testing on the dynamometer. The subject is seated on the machine with legs flexed to 90° and their back kept straight. Key anatomical landmarks are identified: the lateral femoral condyle is aligned with the dynamometer’s axis of rotation (superior arrow), and the forced arm is secured just superior to the lateral malleolus (inferior arrow). Thigh, waist, and two chest straps were used to secure the patient to the chair.
Statistical Analysis
Because the distribution of all included datapoints was deemed to be normally distributed using a Shapiro-Wilk test, descriptive statistics were reported for all included patients using means and standard deviations. To compare values from the injured and non-surgical limbs, paired t-tests were utilized. Pearson’s correlation coefficient was used to report the correlation between radiographic limb length measurements (limb, femur, and tibia length) and isometric quadriceps strength variables (peak torque, average peak torque, average peak torque to bodyweight) for both the surgical and non-surgical limb. The following guidelines were used to assess the value of the calculated correlation coefficient (r): little to no relationship (0-0.25), weak relationship (0.25-0.50), moderate to good relationship (0.50-0.75), good to excellent relationship (0.75-1.00).27 All data were analyzed using SPSS Statistics (v24; IBM), with an alpha <0.05 for statistical significance. For the correlation analysis, post-hoc testing was applied using a Bonferroni correction to reduce the probability of a type I error.
The power of the current analysis was determined post hoc using the correlation coefficient of the average femur length and the surgical limb population of 40 patients. Assuming an alpha level of 0.05, it was determined that the current study achieved sufficient power (ß=81%).
RESULTS
Sixty-five patients met the inclusion and exclusion criteria within the prospective enrollment period. A total of 40 patients (26 males, 14 females), with an average age of 25.8 ± 11.7 years, met the inclusion and exclusion criteria and were included in the final analysis. The average BMI of the study population was 23.9 ± 2.4 kg/m2. Two patients’ non-surgical limb data were excluded from analysis due to patellar tendon graft harvest for a contralateral ligament reconstruction, leaving 38 knees in the non-surgical cohort. Among patients included in the final analysis, 24 had a ligamentous reconstruction procedure, six had cartilage transplant procedures, seven had isolated meniscus repairs, and three had knee arthroscopies.
Isometric quadriceps strength data were collected on all patients from both their surgical limb (n=40) and non-surgical limb (n=38) in the same clinical visit at an average of 5.8 ± 2.5 months (range, 3.5-15.1 months) postoperatively. The surgical limb demonstrated significantly lower peak torque, average peak torque, and average peak torque to bodyweight compared to the non-surgical limbs (p<0.001). The average strength deficit of the surgical limb compared to the non-surgical limb during strength testing was 29.6% ± 21.1% (Table 2).
Relationship Between Bone Lengths and Quadriceps Strength
Femur length in the non-surgical limb was significantly correlated with each of the quadriceps strength metrics considered: peak torque (r=0.43, p=0.048). Tibia length and limb length were not found to be significantly correlated with peak torque (r=0.32, 0.39 respectively, p>0.05). When the surgical limb was considered, femur length (r=0.37), limb length (r=0.36), and tibia length (r=0.33) were not significantly correlated with peak torque (p>0.05) (Table 3).
Among ligament reconstructions that did not utilize the contralateral patellar tendon for reconstruction (n=22), there was a significant negative correlation between both limb length and strength deficit (r= -0.47, p=0.03) and femur length and strength deficit (r= -0.51, p=0.02). There was not a significant correlation with tibia length and strength deficit (r= -0.35, corrected p=0.18).
DISCUSSION
The most important finding of this study was that femur length was significantly correlated with quadriceps strength for the non-surgical limb. Additionally, among knees that underwent ligament reconstructions, there was a significant negative correlation between both lower limb and femur length, and isometric quadriceps strength deficit. This novel approach of an anthropometric specific normalization of strength values may assist in the development of performance standards following surgical intervention. These findings shed light on specific bony morphological features that may influence strength variables measured clinically and could assist in optimizing and individualizing exercise prescriptions. Physical therapists and surgeons may use the findings in the current study to individualize goal setting based on patient morphology as it relates to strength recovery and guidelines for return to activity and sport following knee surgery.
While femur length was significantly correlated with quadriceps strength metrics for the non-surgical limb, after the use of the Bonferroni correction the current authors were unable to reject the null hypothesis, with respect to limb length and tibia length for either the surgical or non-surgical limbs. Bolz et al.28 found that in eight patients with limb length discrepancies (defined in their study as > 5 mm in side-to-side difference between limbs), the shorter limb was consistently weaker with respect to knee flexion and extension strength. In addition, Hamzat et al. demonstrated a significant relationship between patient height and quadriceps strength in healthy individuals in a pilot study.23 Multiple authors have also reported that local muscle volume is significantly correlated to isometric strength.29–31 The current study was limited to measures of static bone length and the relationship with isometric quadriceps muscle torque. The current authors did not perform additional imaging to measure muscular length or calculate cross-sectional volume, so the current authors cannot extrapolate our findings to corroborate results from previous studies examining the relationship between total muscle volume and strength. However, the current study does report that femur length was statistically significantly correlated with peak torque in non-surgical limbs and that length is a contributing factor to isometric muscle strength.
A significant negative correlation was identified between both overall lower limb and femur length and isometric quadriceps strength deficit between the surgical and non-surgical limbs at an average of 5.8 months postoperatively, among knees that underwent ligament reconstructions. This may suggest that patients with longer limbs are either quicker to recover quadriceps strength symmetry or are able to retain a greater percentage of their pre-operative strength following ligament reconstruction. Additionally, femur length was significantly negatively correlated with strength deficit, while tibia length was not. While this is the first known study to consider the association of limb and bone length on strength deficit following ligament reconstruction surgery, this correlation may help inform expectations for rehabilitation timeframes.
Traditionally, quadriceps strength is normalized to account for patient body weight,32–34 as was performed in the current study. However, because peak torque was shown to be significantly correlated to femur length in non-surgical limbs, it may be reasonable to add additional normalization protocols to account for an individual’s long bone length when considering isometric quadriceps strength. This suggestion was not supported by the analysis from Qazi et al.25 who found that although tibia and femur length were significantly correlated with leg extension strength, height alone is the preferred anthropometric measure for adjusting muscle mass and strength. However, it should be noted that the measurement techniques in Qazi et al.25 used the greater trochanter as the superior margin of the femur measurement, which fails to account for the full length of the quadriceps muscles. The literature would benefit from further analysis considering a universal method of normalization of isometric strength data based upon femur and/or extremity length and could look to the present study as a pilot for future reference. This further normalization could improve knee surgeons’ and therapists’ understanding of both post-surgical rehabilitation and also the effectiveness of strength training protocols, particularly when formal biomechanical testing is not available.
This study was not without limitations. First, the current authors acknowledge that full-length weightbearing radiographs may not be routinely available for all patients seen in a physical therapy clinic, and as such, the tibia and femur measurement techniques may be difficult to reproduce manually. Second, the relatively low sample size from a single surgeon’s practice may limit the external validity of the testing results including strength metrics which may be related to surgical recovery and other confounding variables (e.g. pain, swelling, arthrogenic muscle inhibition). Additionally, despite the fact that this sample size was determined to achieve sufficient power (ß=81%) on post hoc analysis, the current authors unable to perform a power analysis a priori. Third, the variability in the postsurgical follow-up period may contribute to differences in surgical limb strength. However, this study attempted to control for confounding variables as all patients were recruited from the same surgeon’s clinical practice, and all quadriceps strength data was collected by the same clinicians using the same instruments.
Conclusion
Femur length was significantly correlated with the isometric quadriceps peak torque for non-surgical limbs. Additionally, femur length and limb length were found to be negatively correlated with quadriceps strength deficit among ligament reconstruction patients. A combination of morphological features and objective performance metrics should be considered when developing individualized rehabilitation and strength programs
Conflicts of Interest Statement
The authors report no conflicts of interest.