INTRODUCTION
CrossFit® is an activity with increasing numbers of participants that offers benefits in terms of VO2 max, body composition, strength, endurance, and mental health.1 The prevalence of musculoskeletal injuries in CrossFit® practitioners ranges from 12.8 – 73.5%, while the incidence rates reported in previous studies ranges between 0.2 and 18.9 injuries per 1000 hours of training.2 Despite the belief that CrossFit® is a sport that causes a high number of injuries due to the high-intensity exercise, it presents similar injury rates compared to other recreational activities.1 The shoulder (26%), spine (24%), and the knee (18%) are the most commonly injured sites.1,2 In general, most of the injured CrossFit® athletes return to sport in few weeks, however, in 8.7% of injured practitioners a surgical procedure was required, most commonly at the knee joint.2 Injuries occur most commonly in novice athletes and are related to different weightlifting movements, such as deadlift, snatch, clean and jerk, squat, and overhead press.3–5
The shoulder was the most affected location for injury identified in a previous systematic review.2 Muscle injuries were frequent, and often related to a previous injury or inadequate technique.6,7 The most commonly involved muscles were the deltoid, trapezius, and scapular muscles.7 Despite the prevalence of muscle injuries in CrossFit®, no report regarding pectoralis major injury in CrossFit® practitioners was found in the literature. The pectoralis major is commonly injured in sports such as snowboarding,8 football, and weightlifting.9
Injury to the pectoralis major region is related to high-intensity and external overload and occurs usually in men in sports involving abduction and external rotation of the glenohumeral joint.10 The treatment of choice is a surgical repair performed within eight weeks; the surgical technique chosen considers the physician’s proficiency and preference,11 and generally offers a good prognosis.12 After surgical repair of the pectoralis major, positive outcomes include significant pain relief and improved aesthetic appearance; the return to sport occurs in roughly six months.13
Information about the rehabilitation process after a pectoralis major injury and subsequent surgical repair in CrossFit® practitioners is potentially important considering the number of athletes participating in the sport, the complex nature of this injury, and the lack of information in the literature about the rehabilitation process. Therefore, the purpose of this case report was to describe the rehabilitation process performed after the surgical repair of a pectoralis major rupture in a CrossFit® practitioner.
STUDY DESIGN
This case report was carried out according to the recommendations of CARE (Case Report Guidelines), which was developed to provide accuracy and transparency in the publication of case reports.14
Case Description
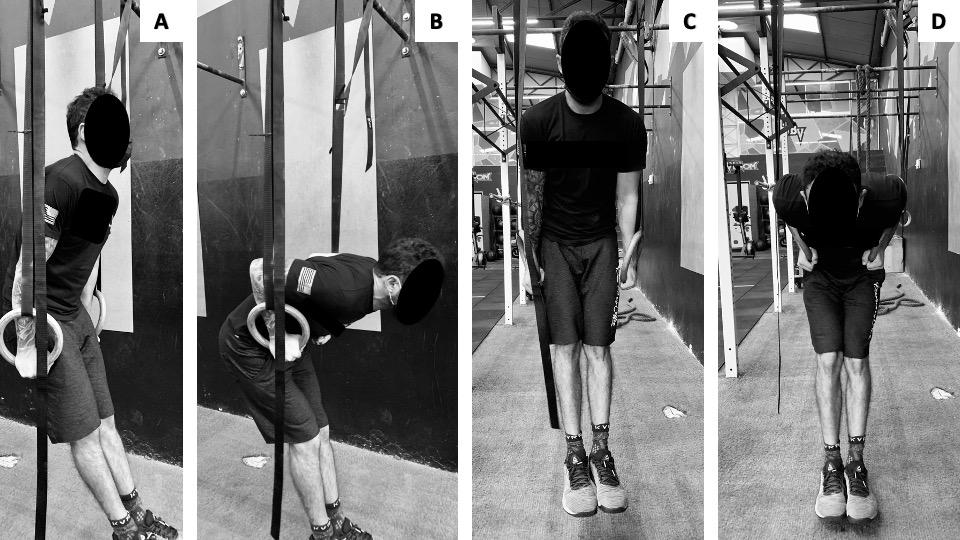
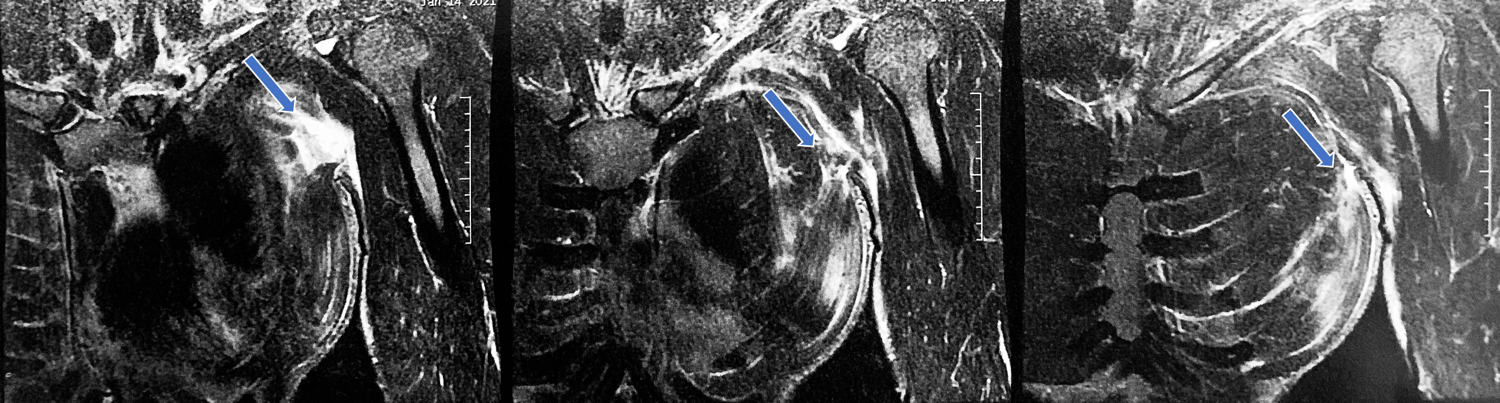
The subject of this case report, E.P.G was a 26-year-old man, (1.75m and 69kg), who had participated in CrossFit® for five years. As part of his training, the athlete performed the ring dip with five series of six movements, the first without additional weight, and the later series with 10 kg, 20 kg, 30 kg, and 40kg respectively. The weights were added using two vests and two bags. (Figure 1). During the eccentric phase of the last series the patient reported feeling a “click”, as well as the feeling that the left pectoralis major was “tearing apart”. Subsequently he also reported stiffness and loss of movement in the left shoulder complex. A Magnetic Resonance Image (MRI) was performed and verified a complete rupture of the sternal portion of the left pectoralis major tendon (non-dominant arm), with retraction of 5 cm of the tendinous stump, signs of edema, as well as stretching of the clavicular portion (Figure 2). A surgical approach was chosen considering the potential benefits regarding the rate of return to sport when compared to conservative treatment.15
_frontal_plane_(c_and_d).png)
_showing_the_rupture_(blue_arrows)_of_the_lef.png)
Outcomes
Surgical Treatment
A direct repair of the tendon in the humerus using two unicortical buttons and two high-resistance tape wires was used via a deltopectoral approach.16
Rehabilitation Program
Recent systematic reviews have synthesized the literature regarding pectoralis major ruptures occurring during sports and with subsequent surgical repairs.9,13 Pectoralis major injuries are rare and the studies included in the systematic reviews present with low methodologic quality, lack of clear injury description, diversity of reported outcomes, and poorly described rehabilitation processes.9,13 Seven studies in these reviews recommended passive shoulder range of motion within four to six weeks after surgery, followed by isometric exercises, and progressive increases in resistance training after six months. In addition, full activity was allowed within six months.13 The rehabilitation protocol described in this case report was constructed considering the current literature available in relation to a pectoralis major rupture followed by surgical repair. The experience of the therapist regarding the sport was used to inform the rehabilitation process.
No studies have been published that discuss pectoralis major tendon repair strain properties; the amount of stress this tissue can tolerate in the post-surgical is not fully understood.17 Therefore, exercise prescription is dependent on the tissue healing process and individual functional readiness in all stages; this process is based on clinical impression.17 CrossFit® is a sport that allows the adaptation of the exercises considering the three major usual gestures (gymnastic; LPO; catabolic). Thus, it was performed a weekly progression of the exercises following the recommendations to protect the surgery (Table 1).
The subject used an arm sling for 30 days in medial rotation position for pain control and protection of the surgical intervention. The rehabilitation program began three weeks after surgery and was performed three times a week for two weeks, and two times a week until the end of rehabilitation at week 16. Each session lasted for 60 to 70 minutes. There were post-operative restrictions until week four regarding stretching and strengthening exercises, for that reason, the protocol focused initially on preventing deformities/contractures of the joint capsule and biceps brachialis, coracobrachialis and subscapular muscles. Also, one important goal was to improve mobility of the scar. Passive range of motion began in post-op weeks three and four, and muscle strength, proprioception, and return to sport was the focus of weeks five to sixteen. The full protocol is presented in Appendix 1.
Outcomes
The subject achieved full active shoulder extension, internal rotation and external rotation on the affected side in week six, and full shoulder flexion and abduction in week seven (Table 1).
Muscle strength assessed using model microFET2; Hoggan Health Industries Inc, West Jordan, UT demonstrated asymmetry in week seven in the groups evaluated, however, this asymmetry was not present in week fourteen. At that time, the subject presented with relative symmetry in shoulder abduction (LSI ≅ 84.78), adduction (LSI ≅ 97.58), internal (LSI ≅ 86.15), and external rotation (LSI ≅ 85.06) strength. Also, muscle balance was assessed using the agonist (abductors): antagonist (adductors) ratio (Table 2).
After sixteen weeks of postoperative treatment the subject was able to return to all athletic activities related to CrossFit® without range of motion or strength deficits. The practitioner showed no limitation or fear to return to practicing any movement of the sport (including the ring dip) due to the progressive load applied and the safety adopted during the rehabilitation. The patient adhered to the protocol and followed the recommendations inside the box and at home.
DISCUSSION
The subject of this case report was a 26-year-old male that had been performing daily and systematic CrossFit® training for five years. He did not use anabolic steroids. The subjects age is within the range of CrossFit® practitioners (20-40 years) described in previous studies.18 Also, males are more likely to sustain an injury than females.19 The success experienced by this athlete with the provided protocol is important considering that the pectoralis major is essential to strenuous activities.8
The results of this case report are similar to two previous case reports that described a post-op protocol for a pectoralis major rupture in a male snowboarding athlete and in a soldier of the US army.8,20 Those protocols had duration of sixteen8 and twenty-four weeks,20 and similar to the one used in the current case report, were performed to control pain, avoid adherence formation, gain range of motion, restore muscle power, and to return to daily activities/sport. In both cases, the participant had full active and passive range of motion, muscle power symmetry according to isometric dynamometry and returned to his previous level of athletic activities at the end of the treatment.8,20
Ninety percent of CrossFit® practitioners that have had an upper limb surgical procedure returned to sport,12 and several authors have shown the benefits of the surgical management for pectoralis major injuries.18,21,22 In fact, surgical treatment of a complete tendon tear has been consistently superior to non-surgical options, particularly in young individuals.8,17 Thus, the choice for the surgical treatment followed by the rehabilitation protocol executed was chosen for the injury presented by the athlete. CrossFit® practitioners commonly present with a high degree of intrinsic motivation, enjoyment of the challenges associated with the sport, and athletic affiliation23 which together contribute to the adherence and maintenance of this activity. Together, these factors may be considered to have been associated with the success of the rehabilitation of the subject of this case report.
Regarding injury mechanism, the subject of this case was injured during the eccentric phase of the Ring Dip that consists of elbow extension with shoulder adduction (with an external load of 40 kg). In prior case reports, the snowboarding athlete injured during a forced abduction with external rotation, and the soldier sustained the injury during the concentric portion of a bench press (external load of 143 kg).8,20 In all cases, an audible sound, pain, loss of movement, and weakness of the affected side was experienced.
These results suggest that a pectoralis major injury likely occurs when the muscle is under maximum contraction on the demand of the specific exercises with external overload. . In addition, history of previous injuries, lack of coach supervision, the experience on CrossFit®, and the participation in competitions may be related to the etiology of injury.2
Isolated injuries in the proximal region of the upper limbs with indication for surgical treatment related to participation in CrossFit® may be increasingly seen in clinical practice, as the number of CrossFit® practitioners has grown substantially in the past several years. There are reports in the literature of latissimus dorsi injury, stress fracture of the humeral head, and isolated rhabdomyolysis of the infraspinatus muscle in CrossFit® athletes.24–26 To the authors knowledge, this is the first case report regarding a rehabilitation protocol after the pectoralis major rupture with subsequent surgical repair in a CrossFit practitioner.
The main strength of this case report was the medical team as the surgeons and physiotherapists involved had experience in the treatment of CrossFit® injuries. Also, the short time between the surgery and the beginning of the rehabilitation protocol must be highlighted as a factor for good prognosis. Finally, the adherence of the subject to the intervention proposed by the medical team is a factor that should be considered when evaluating the success of the protocol.
The limitations must be highlighted. As is typical with case reports (without a comparison subject or group), the results herein can only be described for this subject and are not considered transferrable to other subjects. This case report assessed the program’s impact on the shoulder range of motion and muscle strength. However, the return to daily activities/sport was assessed only qualitatively and not through a patient-reported outcome or scale.
Conclusion
The results of this case report indicate that a Crossfit® practitioner can be successfully returned to sport after surgical repair of the pectoralis major. While isolated injuries of the pectoralis major have a rare occurrence in Crossfit® practitioners, the results of this case report indicate that a protocol focused on range of motion, muscle strength, and sports-specific movements is effective to promote the return to athletic activities. Future studies are necessary to evaluate the effectiveness of this type of protocol in different high-level and recreational CrossFit®.
Conflicts of Interest
The authors report no conflicts of interest.