
INTRODUCTION
Overhead (OH) athletes such as baseball pitchers are subject to a variety of overuse injuries due to high and repetitive stresses placed on the shoulder. The glenohumeral articulation in particular is susceptible to injury secondary to a lack of inherent stability for the purpose of allowing large ranges of functional mobility.1 Overuse injuries to the glenohumeral joint and surrounding tissues are commonly first managed non-surgically. However, those that do require surgery typically involve a lengthy rehabilitation process and have potential for poor outcomes in athletes hoping to return to their prior level of competition.2,3 Reasons for poor outcomes observed in injured OH athletes include the instability of the shoulder, severity of the injuries suffered, the surgical interventions performed to repair the injuries, as well as many others.
While there are multiple valid and reliable tests used to assess lower limb function and strength during the rehabilitation process, few exist for determining the strength and function of the upper extremity. For example, athletes that suffer an anterior cruciate ligament injury requiring surgery often undergo a rigorous and lengthy pre-operative and post-operative rehabilitation process that involves multiple tests of lower limb strength and function at various time points post-surgery. Among these are isometric and isokinetic tests at various joint angles or speeds often used to objectively measure muscle strength, determine agonist/antagonist relationships, and forecast rehabilitation outcomes.4,5 Although isokinetic dynamometry is considered the gold-standard with regard to muscle strength testing in the clinical setting, it is not always an option for clinicians.6 Further, the same post-injury rehabilitation testing strategies observed in lower limb injuries are not utilized to the same degree in shoulder injuries due to the lack of validated and clinically relevant tests available to the clinician and patient.7 Therefore, there is need to identify additional tests for the upper extremity that can reliably determine strength and function of the shoulder such that clinicians can make informed decisions when preparing an OH athlete to return to competition or sport.
The Athletic Shoulder (ASH) test has recently been proposed as an objective and reliable measure of isometric force production (as a proxy for strength) of the shoulder girdle musculature.8 The test involves measuring force production of the combined shoulder musculature at varying degrees of shoulder abduction with the athlete in the prone position using a force plate. The high validity of force plates and multiple test positions to target different combinations of musculature providing objective measures of upper extremity strength make the ASH test an intriguing option to aid the clinical care team in making decisions on return to play with OH athletes. While data has been published evaluating rugby and softball players with the ASH test, data does not yet exist for baseball pitchers performing the test.8,9 Baseball pitchers exhibit well-documented adaptations in shoulder strength and function (such as humeral and glenoid retroversion, posterior capsular tightness, increased labral forces, humeral head translation, capsular expansion, decreased internal rotation and increased external rotation ROM) in the dominant arm and core/hips when compared to the non-dominant side that other athletes do not.10–12 As such, any test measuring upper extremity strength should be sensitive to the adaptations that the OH athlete’s shoulder undergoes.
Therefore, the purpose of this study was to establish values for healthy baseball pitchers performing the ASH test, compare those values with other common tests of shoulder strength and function, and compare ASH test performance bilaterally. It was hypothesized that the dominant arm would perform significantly better on the ASH test compared to the non-dominant arm. A secondary purpose of the study was to evaluate if ASH test performance was related to fastball velocity in baseball pitchers. It was hypothesized that ASH test performance would positively correlate with fastball velocity.
METHODS
The study was cross-sectional in nature and examined healthy male baseball pitchers recruited from local collegiate and high school baseball programs including those that had made a successful return to competition following previous injury. Testing took place within three weeks of the anticipated start of the season, or following completion of a competitive baseball season such that subjects were acclimated to throwing regularly. Seven of the subjects were left hand dominant while the remaining were right hand dominant. Six of the subjects were high school players and the remaining were Division-II collegiate pitchers. Informed consent (or parental consent with subject assent for those younger than 18 years old) was obtained for all subjects prior to their participation in the study. The Sanford Health Institutional Review Board approved the study and the rights of all subjects were protected.
Data collection consisted of two sessions. First, subjects arrived for a clinical assessment where anthropometrics, past injury history, shoulder strength, and shoulder range of motion (ROM) data were collected. Prior to ROM and strength testing, all subjects warmed up for five minutes on an upper body ergometer at a self-selected pace. Passive shoulder external and internal rotation ROM was then assessed bilaterally using the scapular stabilization method previously described in detail by Wilk et al.13 A trained researcher moved the subject’s shoulder through either internal or external rotation until the end range was determined and recorded by a second researcher using a goniometer. Two measurements were taken for each motion and the average of the two was used for analysis. If the two measurements differed by greater than 10%, a third measurement was taken and the average of the three was used for analysis.
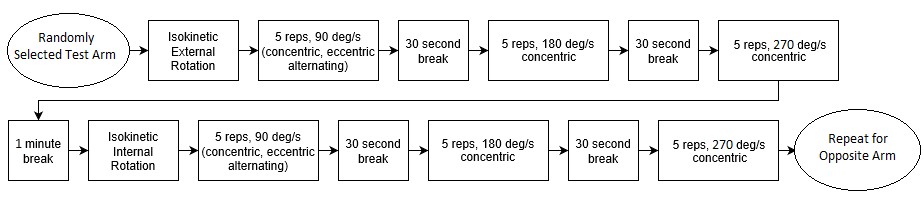
Next, isokinetic and isometric shoulder strength was measured. Isokinetic strength was assessed using an isokinetic dynamometer (Biodex, Mirion Technologies, Shirley, NY) with subjects seated upright with 90° of shoulder abduction and 90° of elbow flexion in the scapular plane as described previously.14 Internal and external rotation strength were measured concentrically at speeds of 90, 180, and 270°/s and eccentrically at 90°/s for each arm with five reps per speed. The initial testing arm was chosen randomly and subjects were allowed a warmup set to familiarize themselves with the protocol (Figure 1). Peak torque normalized to bodyweight was collected for each test condition. Peak torque has been found to be reliable when isokinetically measured for shoulder internal and external rotation.15 The strength test battery (isokinetic or isometric) was assigned randomly with at least three minutes of rest between the two protocols.

Isometric shoulder strength was measured bilaterally using the ASH test. Testing was performed as described by Ashworth et al.8 with subjects prone on the floor at a pre-determined level of shoulder abduction and palm of the hand resting on a force plate. In addition to the three “I, Y, T” test positions used, a fourth position of 0° shoulder abduction was used where the subjects’ hand was resting by their side. For each test position, subjects were asked to push into a portable force plate (Bertec Inc., Columbus, OH) with as much force as possible for three seconds. This was repeated for three trials at each test position with 30 seconds of rest between each trial (Figure 2). Verbal encouragement was provided for each trial and force data was collected at 1000 Hz. Peak force was extracted for each trial, normalized to bodyweight, and averaged across the three trials for analysis.

Approximately one week later, subjects returned for a bullpen session in a biomechanics laboratory. No subjects had played a game or been injured between testing sessions. The lab setup consisted of an artificial mound 13.7 meters (45 feet) from a simulated strike zone. The strike zone was positioned to account for the shortened throwing distance. Subjects were allowed to complete their own warmup process consisting of static and dynamic stretching, light throwing of baseballs and weighted balls, and pitches off a mound. Once subjects indicated they were ready to throw with maximum effort, ten fastballs were thrown at the strike zone. Pitch speed was recorded using a radar gun (Stalker Pro II, Stalker Sports Radar, Plano, TX) and the five fastest pitches thrown for strikes were averaged and used for analysis.
All data analysis was performed in MATLAB (Version 2021a, Mathworks, Natick, MA). Shoulder strength and ROM results were compared for bilateral differences using paired t-tests. Additionally, the relationship between ASH test performance and fastball velocity was assessed using Pearson correlation (α = 0.05).
RESULTS
Thirty-five male pitchers participated in this study. Ball velocity and subject anthropometrics can be found in Table 1.
Means and standard deviations for passive shoulder ROM data can be found in Table 2. Subjects exhibited significantly greater external rotation (ER) ROM and significantly less internal rotation (IR) ROM on the dominant arm compared to the non-dominant arm (p < 0.001 for each). There was not a significant difference in total ROM bilaterally between arms (p = 0.16).
Multiple significant differences were observed in isokinetic strength bilaterally (Table 3). Subjects produced significantly greater peak torque when measuring both the external and internal rotators eccentrically in the dominant arm compared to the non-dominant arm (p = 0.002 and p = 0.004, respectively). The internal rotators of the dominant arm also produced significantly greater peak torque concentrically compared to the non-dominant arm at all three speeds tested (p < 0.05 for all). Additionally, the dominant arm external rotators produced significantly greater peak torque concentrically compared to the non-dominant arm at the 270°/s test speed (p < 0.05).
Isometric peak force measured by the ASH test was not significantly different bilaterally for two of the four abduction positions (Table 4). Subjects produced significantly greater peak force at the “T” (90° abduction) and “Y” (135° abduction) test positions on the dominant arm compared to the non-dominant (p < 0.001 and p = 0.001, respectively).
Peak force production during the ASH test for the throwing arm was not statistically significantly related to fastball velocity (Table 5).
DISCUSSION
The purpose of this study was to collect data on healthy baseball pitchers performing the ASH test, in both the dominant and non-dominant arms. Other relevant and frequently used measures of shoulder strength and function are presented in addition to ASH test results to provide a comparison to commonly used clinical assessments. The results of this study support the initial hypothesis that pitchers would perform significantly better on the ASH test with the dominant arm compared to the non-dominant arm. The ASH test was not found to be a good predictor of fastball velocity for pitchers in this study, rejecting the secondary hypothesis. Many of the additional findings support those previously reported; with pitchers exhibiting greater external rotation and limited internal rotation on the throwing arm as well as increased concentric internal rotator strength and eccentric external rotator strength compared to the non-dominant arm.14,16–19
Pitchers in this study exhibited significant differences bilaterally in passive shoulder ROM for internal and external rotation. This coincides with previous findings in baseball pitchers where the dominant arm undergoes an adaptation of increased external rotation and decreased internal rotation.20–22 Pitchers in this study had an ER increase of 9.9° and an IR decrease of 13.5° on average in the throwing arm compared to the contralateral side, demonstrating lack of significant overall loss of ROM. These findings are comparable to previous studies where it has been found that the ER-IR increase-decrease relationship is near equal.20,21
In this study, ten of the players (28.6%) had differences of <5° for ER bilaterally. A prospective study by Wilk et al.23 found that professional pitchers without a difference in shoulder ER on the throwing arm of at least 5° greater than the non-throwing arm were at 2.2 times greater risk of upper extremity injury. While the athletes in this study were not of professional caliber, it is likely that the findings from Wilk et al. may translate to high school and collegiate players. Thus, the ten players with differences of <5° for ER bilaterally may be at higher risk of injury. Future prospective research in non-professional athletes assessing pre-season and intra-season ROM is imperative for further clarification and appropriate risk-profiling.
Multiple significant differences were observed bilaterally in isokinetic strength measurements. Specifically, pitchers demonstrated significantly greater eccentric external rotator peak torque as well as significantly greater concentric internal rotator peak torque at all three testing speeds on the dominant arm compared to the non-dominant (Table 3). Pitchers also exhibited significantly greater concentric external rotator strength at the fastest test speed. These findings support those previously reported that OH athletes develop significant rotator cuff strength differences bilaterally for both the internal and external rotators.14,17,24 Interestingly, the current findings contradict previous findings of reduced external rotator strength,14 as pitchers presented with an increase in eccentric and concentric ER strength. The differences in level of play of the athletes in this study may be a possible explanation for these findings. Adaptations to the glenohumeral joint complex are likely progressive as the throwing athlete ages and may be more pronounced in professional athletes compared to the population in this study. However, this study provides benchmark data for high school and collegiate athletes and could be easily expanded and repeated in the professional population to evaluate normative data in that population.
Specific to the ASH test, pitchers demonstrated significantly greater isometric strength at 90° and 135° of shoulder abduction on the dominant arm compared to the non-dominant. This could be a result of the angle of shoulder abduction at which pitchers commonly throw, between 80 and 110+ degrees.25 The throwing shoulder horizontal adductors are likely stronger in these positions through adaptations acquired by pitching. This novel outcome demonstrates that the ASH test is capable of detecting bilateral strength differences in baseball pitchers presenting with musculoskeletal adaptations common to overhead athletes. Only one other study has used the ASH test to examine shoulder strength in throwing athletes and found no significant differences bilaterally.9 Potential explanations for the conflicting results may lie in the positioning utilized for the modified version of the ASH test and from player types. Biaggi et al.9 examined subjects in supine positioning rather than prone as the ASH test is typically performed and included players from all fielding positions, rather than pitchers alone. This study utilized pitchers only and the prone position for the purpose of isolation of shoulder strength in dedicated OH throwing-specific athletes. The findings of the current study warrant future research using the ASH test and the prone position to examine shoulder strength in OH athletes from other sports such as tennis and handball to determine if similar trends exist in these populations.
Mean peak force for both arms was ≥11% bodyweight for all positions tested in the ASH test. Only two participants (5.7%) in the 0° and 135° abduction positions and three participants (8.6%) in the 90° position produced less than 9% peak force normalized to bodyweight. While the sample size of this study is not large enough to establish normative ASH test values for baseball pitchers at all levels (e.g. professional and youth), the data presented here provides a good basis for assessing adolescent and college pitchers. These findings could be utilized by clinicians as a pre-season screening tool to monitor shoulder health or as a rehabilitation guideline when determining progress in injured baseball pitchers. The benefits of including this test as part of a battery of tests to determine shoulder function and strength include the high reliability, validity of force plates, and opportunities to explore additional isometric force-time variables such as impulse and rate of force development in an isolated, controlled setting with low risk for further injury or instability during testing. Future research should be done to determine the clinical relevance of the ASH test and its relationship with other tests of upper extremity function such that clinicians can be confident that the test adds value and clarity to the complex process that is rehabilitation of shoulder injuries, which currently lacks reliable and objective methods for determining return to play appropriateness.
This study is not without limitations. First, the current ASH test protocol requires the use of a force plate, limiting the usability when one is not available. Future studies may investigate the feasibility of more cost-effective options such as a handheld dynamometer for administering the ASH test. The cohort tested for this study consisted of high school and collegiate athletes. This limits the generalizability of the findings to populations outside of the one studied such as youth and professional. Although significant differences were discovered in the ASH test bilaterally, there has been no study which has examined ASH test performance and outcomes in injured OH athletes. Therefore, the ASH test may be more useful as a pre-season and post-injury benchmark for recovery following injury, or as a baseline for healthy players to determine adequate rest between throwing outings, and the results should be taken into appropriate context. Examining the effects that rehabilitation has on ASH test performance at multiple time points during recovery from injury/surgery is also critical to understand the true relevance of the test. Furthermore, players with specific injuries and surgeries should be investigated, as anatomic and functional deficit varies with differing injury patterns which may be reflected in ASH test data. Nonetheless, the current study presents intriguing results regarding value and utility of the ASH test.
CONCLUSION
This study presents the strength and ROM profile for a group of healthy collegiate and high school pitchers in which ASH data had not previously been reported. Pitchers in this study produced significantly greater peak force at the 90° and 135° abduction positions, which are similar to the position of the shoulder when throwing a baseball. These findings are in agreement with the adaptations commonly observed in pitchers in which shoulder ROM and strength are altered to favor the throwing motion. While these results may be intriguing for clinical use, caution should be taken when using peak force from the ASH test as a means of predicting fastball velocity in pitchers.
ACKNOWLEDGMENTS
The authors would like to thank Zadok Isaacs, Jason Thompson, and Cody Reed for their help in the data collection process.
FUNDING
This research was internally funded by Sanford Health.
DISCLOSURES
The authors have no financial or conflicts of interest to disclose.
This study was approved by the Sanford Health Institutional Review Board.