
INTRODUCTION
Anterior cruciate ligament (ACL) injuries can be career-ending for athletes,1 and have life-long health consequences2 and economic costs.3 As such, prevention of ACL injuries has immense potential benefits which have fueled enough research to support both a meta-analysis of meta-analyses4 as well as a Clinical Practice Guideline.5 One of the most effective programs, The 11+ has been shown to have a numbers needed to treat value of 70,6 preventing about one injury every three seasons for a 20 person male roster. This benefit comes from the investment of 20 minutes into a warm-up program which is performed before training and games.6 Unfortunately, coaches see the high cost of implementation as a barrier.7,8 Since the majority of coaches who implement prevention programs only implement parts of programs9 the time required to perform the program is likely perceived by coaches as too long.
Prevention programs would be more efficient if high-risk athletes could be directly targeted. Targeting is theoretically possible as the mechanisms of ACL injury are well understood.10 The complex interplay of forces that tear the ACL,10 as well as the gameplay situations and kinematics occurring during the injury event are well described.11–15 Prospective studies have not, however, identified strong risk-factors that are consistent with the injury mechanism.16–19 There is a gap between injury mechanism studies and prospective risk factor studies as the latter have not accounted for the timing of injury in their search.16–19
Two variables are crucial in the injury mechanism and should be accounted for: time and force. The ACL injury occurs quickly after ground contact11 and one of the forces that tear the ACL is the knee valgus moment.20 A cluster analysis method has been developed that has identified early peaks in knee valgus moments (simply referred to as Early Peaks in this manuscript) with timing consistent with the ACL injury21 and therefore is a potential risk factor for ACL injury. It has been shown that kinematics observed during ACL injuries are associated with the frequency of Early Peaks,22 further strengthening the case for Early Peaks as a risk factor for ACL injury. As ACL injuries are relatively rare with only about two injuries per 10000 hours of participation for females,23 prospective studies require either large sample sizes or very long follow-ups for statistically robust results. Strong evidence for potential risk factors built from basic science on ACL injury mechanisms should precede prospective risk factor studies.
The case for Early Peaks as a potential risk factor would be strengthened if intervention programs known to decrease the risk of ACL injury could decrease the frequency of Early Peaks observed using laboratory-based motion analysis. The aim of the current study was to evaluate the effects of The 11+ intervention program, performed by female soccer players during a single season, on the frequency of Early Peaks during athletic tasks. It was hypothesized that The 11+ program decreases the frequency of Early Peaks in valgus moments in female collegiate soccer players.
METHODS
This is a secondary analysis of a completed prospective cohort study on the effects of The 11+24 on kinetics and kinematics of several tasks.25 All procedures were approved by the Institutional Review Board at the University of Delaware. Subjects were given written and verbal descriptions of all study protocols and signed an informed consent. A convenience sample of 10 female collegiate soccer teams were invited to participate in the study. Three teams (NCAA Division I and II) accepted, out of which two (Division I) volunteered to implement The 11+ program and one team (Division II) volunteered to serve as a control. The teams were therefore not randomized but assigned based on their own preference. All participants for whom data was available for both pre- and post-season motion capture were used for this analysis.
Data Collection
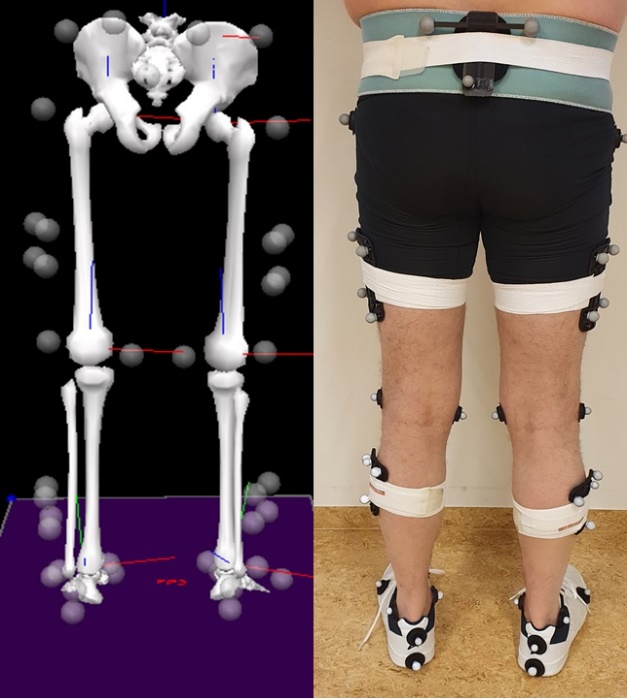
Anatomical markers were placed on the pelvis (iliac crests), thigh, shank, and feet to create a lower extremity musculoskeletal model. Tracking markers attached to rigid shells were placed on the pelvis, thighs, and shanks and secured with elastic wraps. Tracking markers were additionally placed on the heels of the shoes. An overview of the markers and musculoskeletal model is provided in Figure 1. All markers were placed by the same person for all data collections. The person placing the markers had additionally passed the reliability training measures used by the lab to ensure consistency. Marker trajectories were tracked at 240Hz using an eight-camera motion capture system (Vicon, Oxford Metrics Ltd, London, England). Force data were captured with a 6-component embedded force place (Bertec, Worthington, Ohio, USA) sampling at 960Hz.

The athletes hit the force plate three times with each leg for each of three different change of direction tasks. Greater approach speed has been shown to influence the knee valgus moment during cutting maneuvers.26 Approach speed during the tasks was therefore not controlled but athletes were encouraged to perform the movements with maximum speed and intensity. The movements were:
a) Running forward-to-running backward change of direction. The athlete ran forward about 3m until they reached a force plate and pushed off it to change direction and run backward as fast as possible.
b) Lateral shuffle change of direction. The athlete did lateral shuffles for about 4 strides until they reached a force plate and pushed off it to switch directions to do lateral shuffles in the opposite direction. The leading leg was used to change directions and was the trailing leg after the direction change.
C) Cutting maneuver. The athlete ran forwards for about 3m until they reached a force plate and pushed off it to achieve a 90° cut away from the stance leg.
Intervention
The 11+24 intervention was led by team personnel (coach / athletic trainer). Teams were instructed to perform the intervention as described by FIFA Medicine Handbook (https://www.fifamedicalnetwork.com/wp-content/uploads/cdn/11plus_workbook_e.pdf). Team staff was supported by one in-person educational session provided by a researcher highly qualified in the implementation of injury prevention programs at the start of the study, provided with written materials, and a program DVD. Team staff involved with the intervention were given the option to contact the researchers with any questions or concerns regarding the intervention. The program was used during the three-week pre-season and during approximately 22 weeks of the season, but not during the off-season or into the play offs. The teams were contacted in order to gather information regarding whether they were actively utilizing the intervention program, but no other information regarding compliance was collected.
Data Processing
Marker trajectories were used to fit a seven-segment musculoskeletal model using the six degree-of-freedom method. Knee joint moments were calculated using inverse dynamics on raw marker and force plate data and normalized by weight (kg) * height (m). The external knee joint moment is described in this analysis.
The calculated moment was low pass filtered. A low pass filter cut-off frequency that retains the curve shape of the ground impact while also reducing the complexity of the signal is required for the cluster analysis step. A fast Fourier transform spectrum analysis was carried out on two randomly selected trials. It was found that most of the signal content was contained in frequencies below 24Hz. However, a low pass filter cutoff of 6Hz was necessary to perform the cluster analysis. The amplitude of the ground impact is therefore greatly affected by the filter. However, the shape of the waveform is retained.
Cluster Analysis
Injuries to the ACL occur shortly after ground contact. The first 80ms of stance was used for cluster analysis to allow identification of knee moment peaks at or before 60ms. Cluster analysis was conducted similarly to previous studies21,22 where the time series were first transformed into the signed difference. Thus, the only information being clustered on was changes in direction of the signal (increasing or decreasing). The Euclidean distance was used as the distance metric and the ward d227 algorithm used to create clusters.
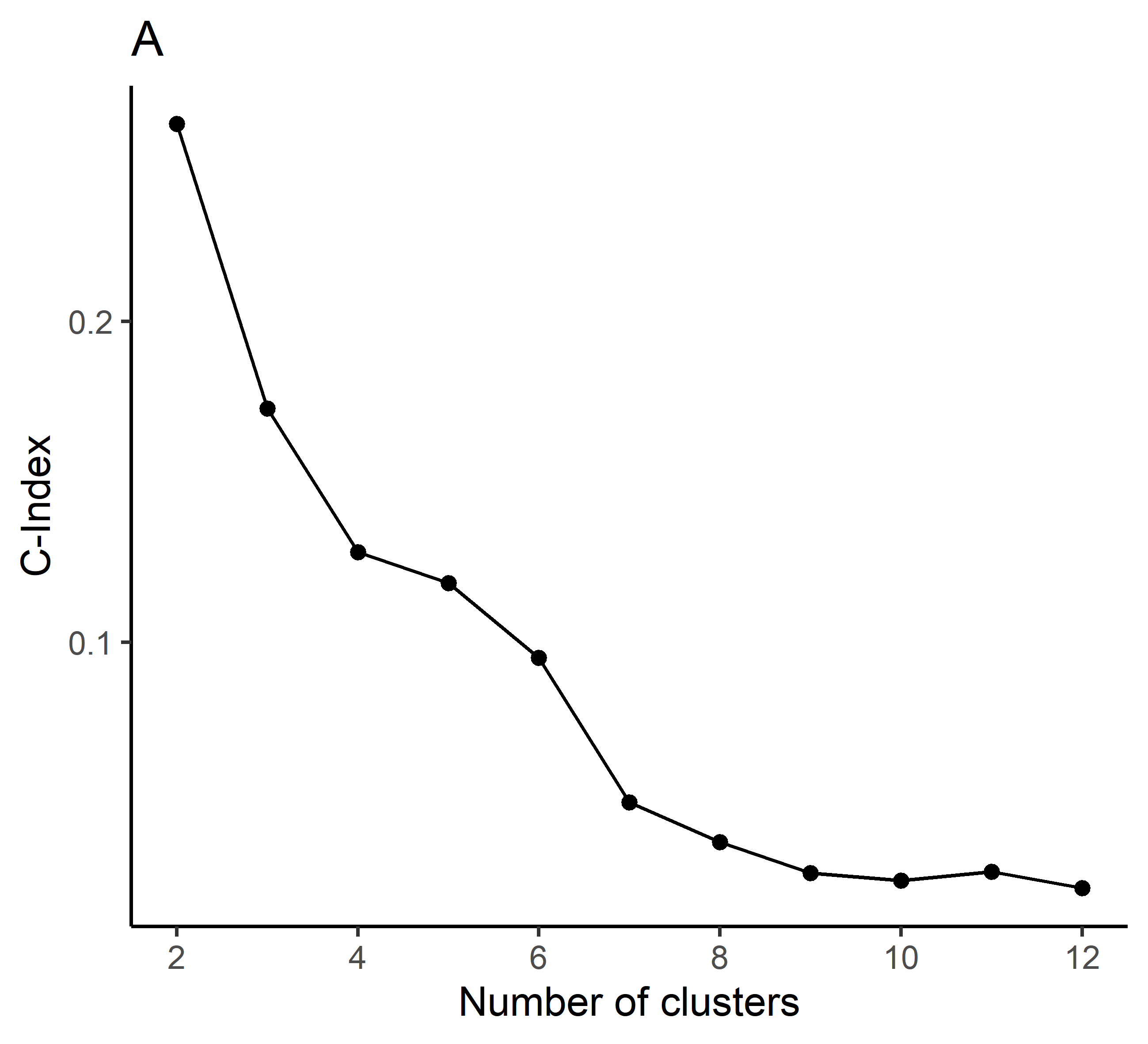
The C-Index was used to determine the fit of the clustering process and the appropriate number of clusters created. The C-Index is the ratio of the sum of distances within clusters minus the smallest distance observed, to the difference between the largest and smallest distances in the data set.28 Values closer to zero represent better clustering. The number of clusters to analyze was chosen as the ‘elbow’ of the C-Index plot, the point where adding more clusters starts to have diminishing returns in fit.
The relevant waveform for the ACL injury mechanism is an early peak in the knee valgus moment. Previous studies with cluster analysis on knee valgus moment data21 have shown that some of the clusters identified will show the relevant early peak shapes, and some will not. Furthermore, the timing of the peak knee valgus moment can be variable. For those reasons, a visual inspection was used to create subgroups which are similar in terms of whether or not an early peak knee valgus moment is present. For this analysis, subgroups of waveforms was also created depending on if the timing of the peak is before or after 40ms, which has been identified as the timeframe where an ACL injury is most likely to occur.11
Statistics
The main outcome measure was how frequently cluster waveforms with peaks before 80ms were observed. Since differences between legs were not important for this analysis, legs were pooled for the analysis. To determine the effects of the intervention on the number of Early Peak knee valgus moments, a mixed linear regression with a Poisson link function was used.29 A regression model was calculated for each Early Peak type identified with potential relevance for ACL injury. The number of times each waveform was observed (integer scale of 0-6) after the intervention season was the dependent variable. Independent variables were the teams (three categories), the number of times each waveform was observed at the pre-season data collection (integer scale of 0-6, and the movement task (three categories). All independent variables were tested as main effects and no interactions were included in the statistical models. The random variable was each individual athlete as a random intercept. Primary hypothesis testing was done comparing models with and without the inclusion of the effect of team using a Chi squared test. The primary effect size is the increase in fixed-effect R^2 (lognormal) of adding the effect of team to the model and was calculated using the MuMIn package.30 Post-hoc testing to compare the different teams was performed using the Satterthwaite’s method implemented with the lmerTest package31 when the primary hypothesis test was significant. Alpha was 0.05.
RESULTS
Subjects
A total of 69 athletes were recruited. The intervention teams confirmed that the intervention was carried out an average of 2.2 times per week. Three subjects enrolled in the study but did not attend any data collections. One data file was missing. Data from 65 subjects was available for the pre-season motion testing: 20 control athletes, 22 from intervention team 1, and 23 from intervention team 2. An overview of the flow of subjects through the study is shown in Figure 2. Eight subjects (three controls, four intervention) did not attend the post season testing due to injury and one subject did not complete any of the test movements analyzed in this study. All available data were used for the cluster analysis, 2190 trials from 67 subjects. A total of 57 athletes had complete data for both pre- and post-season testing and were used for the statistical analysis.

Cluster Analysis
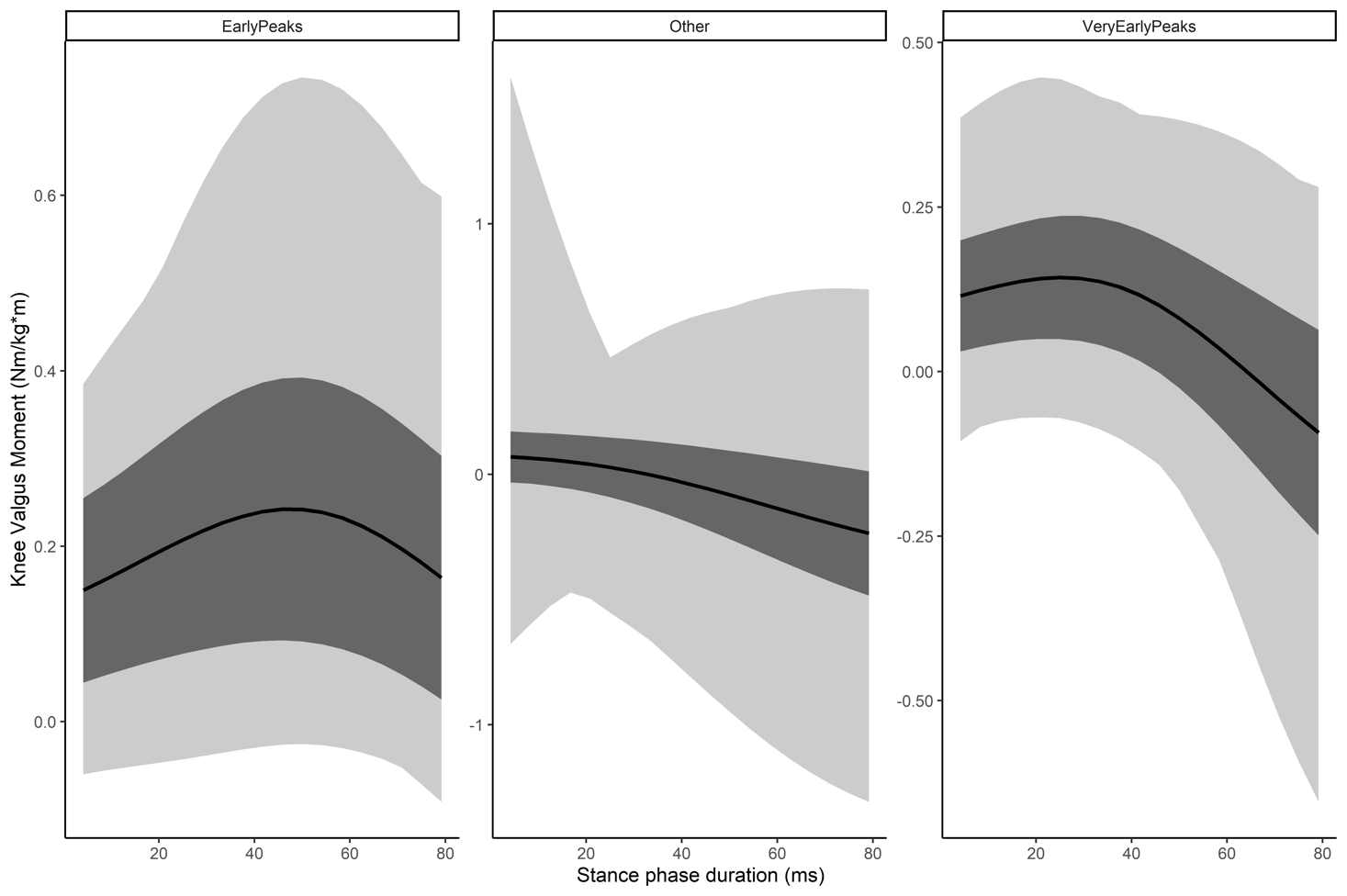
Consistent with previous studies,21 seven clusters were formed (Appendix A, Figure 1) with a C-index of 0.05 (Figure 3) for the seven cluster solution. Visual inspection revealed three distinct shapes (Figure 4) two of which had potential relevance to the ACL injury mechanism. Similar clusters were therefore merged into the categories Very Early Peaks (peaks occurring within 40 ms, two clusters) and Early Peaks (peaks occurring between 40 and 60ms, one cluster). The remaining four clusters were categorized as ‘other’. The mean frequency of each cluster by season and team are shown in Table 1.


Frequency of Very Early Peaks
The model for Very Early Peaks (within 40ms of ground contact) had an R^2 of 0.57 for the full model, and 0.17 for the fixed effects. The R^2 increase of adding the intervention effect was 0.03 (p = 0.363). Full model results are reported in Table 2. Very Early Peaks frequency was similar across movement tasks. Pre-season frequency was associated with post-season frequency. However, there was no effect of the intervention on Very Early Peak frequencies.
Frequency of Early Peaks
The model for Early Peaks (peaks between 40 and 60 ms after ground contact) had an R^2 of 0.45 for the full model and 0.34 for the fixed effects. The R^2 increase of adding the intervention effect was 0.15 (p = 0.004). Full model results are reported in Table 3. Early Peaks were more common for lateral shuffles than the other movement tasks. Pre-season frequency was associated with post-season frequency. One of the two intervention teams had a lower frequency of Early Peaks following the intervention, but the other did not.
DISCUSSION
The main results of the study were that The 11+ intervention reduced the frequency of Early Peaks for intervention team 2, but not intervention team 1. The effect was modest, explaining just shy of 20% of the variance in Early Peak frequency. No intervention effect was observed on the number of Very Early Peaks. Adherence to the intervention may explain why only one of the teams had a reduced frequency of Early Peaks. The teams were asked how often they performed the intervention. However, the adherence to the program in terms of the number of exercises completed or other parameters regarding the specific execution of the program was not evaluated.
The 11+ program has been shown to reduce the relative risk of ACL injuries in male soccer players to about 1/4th that of control athletes,6 and the risk of acute severe knee injuries in female athletes by almost half.24 Although the efficacy of the program to prevent female ACL injuries has, to the author’s knowledge, not been reported, the injury preventative effects are similar in magnitude to the reduction in Early Peak frequency observed in intervention team 2; a 45% decrease post-intervention (Table 1). Two previous analyses from the same sample did not find evidence of a mechanism of effectiveness of The 11+,25,32 but those studies used peak values during weight acceptance.25,32
Extracting peak values is common practice in biomechanics studies and is how risk factors have been identified by prospective studies.13,16,17 Two characteristics of ACL injuries makes the peak extraction method problematic: timing and rarity. The extracted peaks generally occur later in the stance phase than an ACL injury would.33 And since the ACL injury is a rare event during a common movement,23 it is likely that some element of rarity also applies to potential risk factors. After all, if the risk factor occurs all the time, why doesn’t the ACL injury? The Early Peaks in the current study are not limited by these aspects. The timing of the Early Peak is consistent with the timing of ACL injury,11 and Early Peaks were the least common waveform – occurring only in 9% of trials.
The lateral shuffle had the highest frequency of Early Peaks in this study. The lateral shuffle change of direction includes a strong hip-abduction but no rotational component.34 Studies have suggested that hip abductor muscles are able to reduce the knee valgus moment.35 Although speculative without direct evidence, higher demand on those muscles may explain the higher frequency of Early Peaks. The lateral shuffle was also the only test movement not specifically trained in The 11+,24 which may contribute to a higher frequency of Early Peaks if training the other movements has reduced their Early Peak frequency. Change of direction tasks that place higher demands on the hip abductor muscles may be ideal tasks for biomechanical studies on ACL injury risk. However, this study was not sufficiently powered to examine the interaction between the different tasks and the intervention to assess if the two movements trained with The 11+ had greater reductions in Early Peak frequency than the lateral shuffle change of direction.
Limitations
This secondary analysis is subject to several limitations that affect the generalizability of the findings. Only one of the two intervention teams saw a large effect consistent with the expected magnitude of change from injury prevention studies,6 while the other team had no effects. As explained above, this may be due to adherence to the intervention protocol.
Only three trials were collected per movement. As is common with motion capture, not all participants had three valid trials due to technical difficulties which were only evident in post-processing. This results in the potential for under-estimatation of the frequency of each waveform since some collections will have a maximum frequency of two but others three. Previous studies have shown that Early Peak waveforms are relatively rare18,21 which was also true for Early Peaks in this study. Collecting three trials per movement is likely not sufficient to reflect the true Early Peak frequency of the athlete.
It is likely that athletes with higher pre-season frequencies of Early Peaks would display greater decreases due to the intervention compared to athletes with baseline lower frequencies since a similar pattern has been observed with the landing error scoring system.36 This interaction effect between the pre-season knee valgus moment Early Peak frequency during athletic tasks and the intervention was not included in the analysis as the statistical models failed to converge on a solution due to the small sample size.
CONCLUSIONS
Post-intervention reductions in the number of early peak knee valgus moments seen in some athletes during athletic tasks may explain a mechanism of effect of The 11+ intervention program. Future studies are required to establish a link between early peak knee valgus moment counts and risk of ACL injury. Future studies should include tasks more likely to result in a higher frequency of knee valgus moment early peaks, and with enough repetitions to reflect how frequently each athlete displays knee valgus moment early peaks.
Conflicts of interest
The authors have no conflicts of interest.
Funding
Research reported in this publication was supported by the National Institute of Arthritis and Musculoskeletal and Skin Diseases of the National Institutes of Health (award number R01AR072034). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. This work was also supported by grant R37-HD037985 from the National Institute of Health. This work was supported by the Icelandic Research Fund, grant numbers 120410021, 903271305, 1203250031, and 185359051.
Acknowledgements
The authors would like to acknowledge the work of Holly Silvers-Granelli and Amelia J. H. Arundale who collected the data for the study.