
BACKGROUND
Shoulder pain is a prevalent musculoskeletal complaint that is often associated with reduced shoulder function, difficulty sleeping, and difficulty completing activities of daily living.1,2 Subacromial impingement Syndrome (SAIS) is the most common cause of shoulder pain accounting for 45-65% of all reported shoulder pain.3 The prevalence of SAIS is higher in the overhead athlete population, the military, and in occupations where an overhead position must be maintained.1,2 In Denmark, one study found that on average 27 work days were lost due to SAIS during the first six months from the time of initial onset of diagnoses. This was three times higher than any other shoulder diagnosis and presents a concern for work time lost due to SAIS.4
There is debate over best practice when it comes to the treatment of individuals presenting with SAIS.3,5 Currently, experts agree that non-surgical management is the recommended treatment approach for individuals experiencing SAIS.2,3,6,7 According to clinical practice guidelines, best practice interventions include exercise, manual therapy, psychosocial interventions, heat or cold applications, acupuncture, and transcutaneous electrical nerve stimulation.8–10 However, despite these recommendations, more than 50% of all patients with diagnosis of SAIS have pain that persists for greater than three years.11 The current literature indicates that current best practice is insufficient for more than half of all patients seeking treatment for SAIS, and therefore this population requires modifications or novel approaches to treatment guidelines.
Blood flow restriction (BFR) is a training method used during exercise where an external pressure system or cuff is applied to an extremity with the intent of partially restricting the arterial blood flow and fully restricting venous blood flow.12–14 Historically, heavy exercise loads of approximately 70% of an individual’s one repetition maximum (1RM) have been deemed necessary to elicit muscle hypertrophy and strength gains.12,13,15 However, with BFR similar gains in strength and hypertrophy with lower loads can be achieved.12,13 Research in BFR has predominantly focused on the benefits it has towards strength and its ability to limit atrophy. Much of this literature has focused on the lower extremity, however a shift has been noted in newer studies showing similar benefits in the upper extremity.16 Results of recent studies examining BFR in the lower extremity indicate that not only does BFR assist with increasing strength, but also has a pain-relieving effect post-BFR.17 Consequently, BFR may represent a novel modification to the rehabilitation process of individuals presenting with SAIS with the potential to improve upon current outcomes by allowing muscle strengthening below the pain threshold. The purpose of this case series is to describe the inclusion of BFR in the treatment of two patients with SAIS.
CASE DESCRIPTIONS
Two patients, referred to physical therapy by primary care sports physician’s secondary to gradual onset of shoulder pain prior were included in this case series. Both patients reported a decrease in daily function, increase in shoulder pain, and altered satisfaction with quality of life during the subjective portion of their evaluation and through patient reported outcomes.
Both patients denied significant past medical history including prior history of shoulder pain, shoulder surgery, or neck pain. Patients denied systemic pathologies such as diabetes, hypertension, or peripheral neuropathy.
Patient A was a 51-year-old right hand dominant female who reported an insidious onset of left shoulder pain four weeks prior to the initiation of physical therapy. During the initial examination, she reported 8/10 with activity located over the posterior lateral aspect of her shoulder without radiating symptoms, that would require her to rest for 1-2 minutes for her pain level to drop to 5/10, followed by another 2-3 min before her baseline pain dropped to 1-2/10. Patient reported her pain never dropped below a 1 or 2 out of 10 and her pain was worse with reaching overhead, sleeping on shoulder, and reaching behind her back during dressing activities. Pain decreased minimally with rest and ice. Patient A’s goal for physical therapy was to improve her ability to perform dressing activities behind her back, and to increase her ability to perform reaching and lifting activities.
Patient B was a 46-year-old right hand dominant male, who reported an insidious onset of right shoulder pain three weeks before the initiation of physical therapy. During the initial examination, he reported sharp pain of 3/10 at rest, and 6/10 with activity, which was located over the anterior lateral aspect of his shoulder without radiating symptoms. Pain was worse with lifting >50 pounds to shoulder height and >10 pounds overhead, with reaching behind his back to put on a belt. Patient also reported an increase in pain with weightlifting and tennis activities that he normally completed 4x a week. At initial evaluation he reported having to modify workouts by eliminating overhead pressing, decreasing the number of workouts per week, and decreasing tennis frequency. Pain decreased with rest, modification of lifting activities, and ice. Patient B’s goal was to decrease pain associated with lifting, carrying, and reaching activities, and to return fully to his workout and tennis routine.
OUTCOME MEASURES
Participants were evaluated at initial evaluation and discharge from physical therapy.
Patient-reported outcomes
To assess pain, function, and satisfaction with current function, the Pennsylvania Shoulder Score (PENN) was used, which is a validated tool for patients with shoulder pain. The PENN includes a 3-item pain subscale, a 1-item satisfaction subscale, and a 20-item function subscale. Scores in each subscale were added resulting in a total score from 0 to 100 with higher scores reflecting less pain and greater function and satisfaction with function.18 The PENN has a minimal clinically important difference (MCID) of 11.4 points.18
The American Shoulder and Elbow Surgeon Shoulder Assessment Form (ASES) was used to assess patient’s upper extremity function, activities of daily living, and pain. The ASES contains a single 11-point numeric rating scale anchored with 0= no pain at all to 10= pain as bad as it can be to assess pain and a 10-item functional scale with activities scored from 0 unable to do to 3= not difficult. The pain and function subscales are each weighted at 50 points and combined resulting in a total ASES score of 0 to 100 with lower scores indicating higher levels of pain and disability.19 This outcome measure has been shown to be reliable, valid, and responsive in upper extremity injuries with an MCID of 6.4 points.20
The Single Alpha-numeric Evaluation (SANE) was used to evaluate patients’ current functional level compared to pre-injury function on a 0-100 scale with 100 reflecting normal function. The SANE has an established MCID of 28.8.21
Function was further assessed using the Patient Specific Functional Scale (PSFS). Patients were asked to identify three important activities currently limited by their shoulder pain and score each from 0= unable to perform the activity to 10= able to perform the activity at their preinjury level.22 The PSFS is valid, reliable, and responsive for upper extremity injuries and has an MCID across three activities of 1.2 points.22
Pressure Pain Threshold
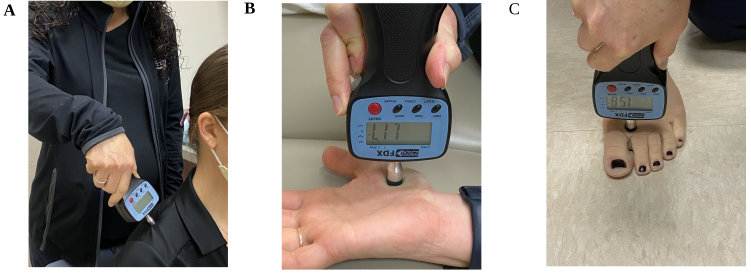
Pressure pain threshold was assessed as a measure of local (at the shoulder) and remote (distant site) pain sensitization. Immediate changes in pain levels with functional activity have been observed in studies that assessed the effects of BFR on anterior knee pain suggesting a hypoalgesic effect.17 Therefore, pressure pain threshold (PPT) was assessed prior to and immediately following combined exercise and BFR at each session to assess local and remote changes in pain sensitization within session and between sessions to determine if similar results could be achieved in the upper extremity. This was done using a handheld digital pressure algometer (Wagner Instruments FPX 25, Greenwich, CT) with a 1 cm diameter rubber tip applied at 1 kgf/cm2 to ipsilateral supraspinatus, ipsilateral thenar eminence, and contralateral dorsal web space between toes 1 and 2 (Figure 1). These locations were selected to assess effects of BFR on pain sensitivity locally (ipsilateral supraspinatus) and remotely (ipsilateral thenar eminence and contralateral web space between toes 1 and 2). The minimal detectable change (MDC) for PPT in patients with SAIS is 1.16 kgf/cm2.23

Impairment-based outcomes
Maximal voluntary isometric strength was measured using a handheld dynamometer for external rotation, horizontal abduction, and scaption for BFR intervention. Internal rotation and abduction were also measured for between session comparison. The MDC for external rotation in asymptomatic patients is 6.44 lbs, and 8.77 lbs for internal rotation.24
Active range of motion was also measured in flexion, external rotation, internal rotation, and abduction. The MDC in asymptomatic patients for flexion is 8 degrees, while abduction is 4 degrees. External and internal rotation was measured in functional patterns with patients reaching behind the back, however no MDC has been established for these movements.25
EXAMINATION
Before determining the shoulder as the primary cause of symptoms, the patients were screened for cervical pathology, bony pathology via radiographs, and systemic pathology as the cause of their shoulder pain.26 Both patients denied a history of cancer, unexplained weight loss, fever associated with symptoms, night sweats, and non-mechanical night pain. Both patients presented with full, pain free cervical range of motion, intact light touch sensation in dermatomal patterns, and weakness that did not follow myotome patterns suggesting the symptoms were not arising from the neck.27
Subject A
Active range of motion (AROM) was limited to 120 degrees of flexion with 6/10 pain, 100 degrees of abduction 7/10 pain, inability to place hand behind her back higher than the posterior superior iliac spine with 9/10 pain and could reach behind her head to the level of the spinous process of the first cervical vertebrae with 5/10 pain. Passive range of motion was limited to 165 degrees of flexion with muscle guarding and 2/10 pain, 150 degrees of abduction with muscle guarding and 4/10 pain, 76 deg off external rotation at 90 deg of abduction with 1/10 pain, and 40 deg of internal rotation with 4/10 pain. She presented with pain and weakness during strength testing using a hand held dynamometer in scaption with 4/10 pain, abduction with 6/10 pain, and external rotation with 6/10 pain, and required 30-60 second rest breaks between handheld dynamometer to allow for patients pain levels to return to baseline levels of 1-2/10 at rest. Subject A also had positive findings on the Neers impingement test, Hawkins-Kennedy, Empty can test, Painful arc sign, and External rotation resistance test. Table 1 summarizes these findings.
Subject B
Subject B presented with symmetrical shoulder AROM, however reported pinching at end range abduction and external rotation which was <2/10 pain for both, while also presenting with painful arc sign with flexion. Subject B presented with decreased shoulder strength via handheld dynamometer for scaption, external rotation, internal rotation, and abduction secondary to reports of pain. Subject B also had positive findings on the Neers impingement test, Hawkins-Kennedy, Empty can test, Painful arc sign, and External rotation resistance test. Table 1 summarizes these findings.
CLINICAL IMPRESSION
SAIS was suspected as the underlying cause of both subjects’ complaints based on the subjective findings of insidious onset of pain along with pain with overhead activities.5 Labral injury, rotator cuff tears, and frozen shoulder were considered less likely as neither subject reported associated trauma or significant loss of ROM.28,29 SAIS was further confirmed as their primary medical diagnosis based on a cluster of tests that assist with identifying diagnosis of SAIS.30 These tests include Neers impingement test, Hawkins-Kennedy, empty can test, painful arc, and external rotation resistance test with three or more positive tests helpful in ruling in SAIS with a specificity of 0.75 and positive likelihood ratio of 2.93.30
Both subjects clinical presentation included impairments commonly seen in patients with SAIS which include shoulder weakness, and pain that limits AROM. Subject A presented with high irritability as her clinical presentation included high levels of pain (>7/10 pain), high levels of resting pain, night pain, pain occurring prior to end ranges of motion, and a significant decrease in function as measured by patient reported outcomes.26,31 Subject B presented with moderate irritability as his clinical presentation included moderate levels of pain(3-6/10 pain), intermittent resting pain, pain at end range of AROM, and moderate decrease in function as measured by patient reported outcomes.26,31
Due to the clinical presentations of decreased strength, and maximal to moderate irritability, the modality of BFR with exercise was considered as the first line of treatment during exercise interventions for three reasons: 1) the clinical practice guidelines for treatment of patients presenting with SAIS recommend strength training at >60% of 1 RM which was not considered attainable due to high irritability with resisted movements.8–10 2) BFR literature in the upper extremity shows improvements in strength for proximal shoulder muscles with <20% of 1 RM.32 3) BFR literature in the lower extremity shows a decrease in resting pain post BFR.17 Therefore, as BFR could allow for a strengthening effect at a lower dosage of exercise as well as the potential for pain modification, it was included in the plan of care as the first line of treatment.
INTERVENTION
Subject A was seen for three visits over three weeks and completed one follow up via phone call, while Subject B completed four visits over four weeks. Both subjects were educated on and agreed to the use of BFR at initial evaluation and best practice guidelines were used when applying BFR.12,13
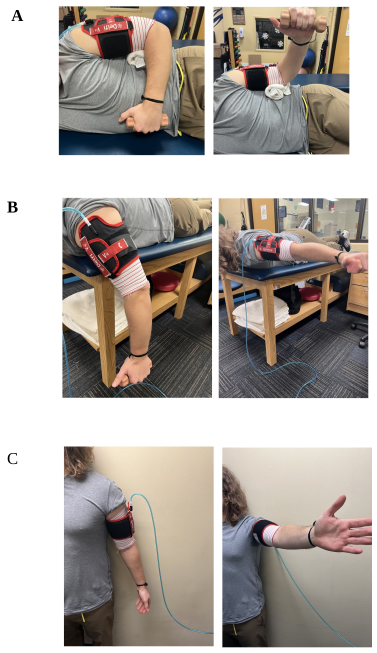
The Delfi Personalized Tourniquet system (Delfi Medical, Vancouver, Canada) was used, with cuff placed around proximal humerus (Figure 2) during three common therapeutic exercises in standard of care of patients presenting with SAIS: side lying external rotation, prone horizontal abduction, and standing scaption.8 Figure 3 demonstrates start and end positions for all three exercises. Prior to BFR, both subjects completed six minutes of warm up on the upper body ergometer. After completion of warm up, the physical therapist measured maximal isometric strength in scaption, external rotation at side, and prone horizontal abduction with a handheld dynamometer to determine 20% of their peak isometric strength.12,13 For consistency, strength testing was completed in the same order each time as follows: side lying external rotation, prone horizontal abduction, and scaption. The physical therapist repeated the maximal isometric testing at the beginning of each treatment session to progress loads appropriately during each exercise. Immediately after, the subject’s limb occlusion pressure was taken in supine to achieve a personalized Personal Tourniquet Pressure which was set to 50% of limb occlusion pressure per BFR standards. Each exercise was completed for a total of four sets, with one set of 30 repetitions, and three sets of 15 repetitions. After each set, subjects were given 30 second of rest with the cuff inflated. After completion of each exercise, subjects were given one minute of rest time, with the cuff deflated per standard practice.12,13 Both subjects were given a home exercise program to be completed on days that they did not come in to PT which included three sets of 12 of side lying external rotation, prone horizontal abduction, and scaption with the weight used during that session’s BFR treatment. These sets and reps were selected in order to achieve the high volume required to induce muscle hypertrophy and compliment the use of BFR. No other interventions were provided during home exercise sessions.


OUTCOMES
Clinically meaningful improvements and changes beyond measurement error were observed in all patient reported outcomes, pain sensitization locally and remotely, and resting pain levels. Both subjects achieved their goals set out at initial evaluation.
Patient-reported outcomes
A variety of patient reported outcome measures were used to track changes in variables including pain, function, satisfaction, and ADL’s. These outcome measures included the PENN, ASES, SANE, and PSFS (Table 2). Both subjects met all MCID’s for each patient reported outcome measure, and per subject report met goals. Subject A had a change of 46, 13, 30, and 3/6/7 respectively on the patient reported outcome measures. Subject B had similar outcomes with a change of 36, 22, 15, 3/2/5 respectively on the patient reported outcome measures. Subject A reported having no pain or limitation with dressing and grooming activities or work-related activities. While subject B reported returning fully to his weightlifting regimen without pain or limitations. He also reported returning to tennis without limitations due to pain.
Pressure Pain Threshold
Pressure pain threshold was assessed locally (at the shoulder) in two locations, and remotely (dorsal web space of contra lateral foot) as a measure of the effects of BFR on pain sensitization proximal and distal to the cuff. Both subjects demonstrated within session changes, after deflation of the cuff at the end of the third exercise (Table 3). Subject A demonstrated large changes in PPT that exceeded the MDC of 1.16 kgf/cm2 every session, but not at every location as noted by not meeting MDC for local sites in Visit 2. Her largest change was Visit 3, over the ipsilateral supraspinatus of her affected UE, with a PPT of 2.09 kgf/cm2. Conversely, Subject B had small changes within session to PPT, and only exceeded MDC twice, 1.54 kgf/cm2 on Visit 2 to the remote site, and 2.16 kgf/cm2 on Visit 4 to the ipsilateral supraspinatus of his affected UE.
However, between session changes for both subjects surpassed the MDC of 1.16 kgf/cm2 with an average change of 4.06 kgf/cm2 for Subject A, and 2.54 kgf/cm2 for subject B (Table 2).
Impairment-based outcomes
Maximal voluntary isometric strength was measured using a handheld dynamometer for external rotation, horizontal abduction, and scaption for BFR intervention, while internal rotation and abduction were measured for between session comparison. While both subjects demonstrated improvements in external and internal rotation strength compared to baseline, subject B was the only one to meet and exceed MDC for external rotation (6.44 lbs) and internal rotation (8.77 lbs) with a change of 9.3 lbs, and 8.8 lbs (Table 2). There were no established MDC values for scaption, horizontal abduction, and abduction, however both subjects demonstrated improvements in strength for all directions.
Active range of motion was also measured in flexion, external rotation, internal rotation, and abduction. Subject A met and exceeded MDC for AROM flexion (8 degrees), and abduction (4 degrees), with an improvement of 30 and 60 degrees respectively. Subject B had no limitations in flexion or abduction at initial evaluation, however, was able to report a decrease in pain at end range AROM.
Table 2 includes a summary of between session changes for patient reported outcomes, PPT, strength via HHD, and AROM. Table 3 includes a summary of within session changes to PPT.
DISCUSSION
This case series describes improvements beyond measurement error and clinically important changes in multiple outcome domains which were associated with the inclusion of BFR in the management of two subjects with a working diagnosis of SAIS. This included improvements in patient-reported outcomes, pressure pain thresholds, and impairment-based outcomes such as strength. Importantly, the rationale for including BFR included: its effects on pain, and its ability to assist subjects who are load compromised and judged to have difficulty following SAIS standards of care due to pain and high levels of irritability.8
The clinical practice guidelines for treatment of patients presenting with SAIS recommends strength training at >60% of 1 RM which was not considered attainable due to high irritability with resisted movements in these two subjects.8–10 Subsequently, BFR was incorporated as BFR is associated with improvements in strength at a much lower dosage (i.e., < 30% of the one repetition maximum).12 Improvements beyond measurement error were found in shoulder strength for both subjects. Specifically, scaption strength improved by 87% and horizontal abduction strength improved by 39% for Subject A, while baseline ER and IR strength did not change significantly from baseline. Subject B, however, demonstrated improvements in external rotation and internal rotation strength by 69% and 67% respectively. Specific to the upper extremity, the results of a prior study of healthy participants demonstrated up to 30% improvement in strength in the shoulder musculature following a six-week program of upper extremity strengthening exercises combined with BFR at 30% of their one repetition maximum.33 These results of greater gains in strength observed in the two subjects could be due to lower baseline levels as reflected in their clinical status and/or the influence pain may have had on force production which would have influenced the initial strength findings.
The decision to include BFR in the treatment of these subjects was further driven by the perception of high irritability and concern for their ability to tolerate the strength training parameters set by standard of care in this population, which exceeds 60-70% of 1RM. Prior authors have observed hypoalgesia accompanying BFR applied during lower extremity exercise leading to the suggestion of BFR as a treatment modification for patients in whom pain limits exercise tolerance.13,34 For example, in a study of healthy participants, greater hypoalgesia (assessed with PPT) lasting 24 hours was observed in response to a unilateral leg press performed with BFR than when the exercise was performed without BFR.32 Furthermore, this effect was observed in the exercised lower extremity as well as in remote sites.32 Similarly, these subjects presented with increased PPT (i.e., decreased pain sensitivity) beyond measurement error at both local and remote sites associated with the inclusion of BFR in a typical strengthening program for a patient with SAIS. These findings add to this body of literature by describing a local and remote hypoalgesic effect in response to upper extremity exercise in two patients presenting with SAIS. Additionally, two studies of participants with anterior knee pain found lessening of clinical pain intensity following the application of BFR during exercise.17,35 Similarly, these findings demonstrate improvements in clinical pain associated with the inclusion of BFR to an exercise program for two subjects presenting with SAIS.
In addition to changes in strength beyond measurement error and clinically meaningful improvements in pain, the two subjects also demonstrated clinically meaningful improvements in function. According to clinical practice guidelines, even the application of best practice leads to >50% of all patients to continue to have significant loss of function due to symptoms more than three years after treatment.8,9,11 Additionally, in this population satisfactory results are only achieved in 60% of cases at two-year follow up.3 Furthermore, one study demonstrated functional improvement through the increase in Penn shoulder scores in patients with SAIS.36 They found improvements from a score of 59 to 81 at two-year follow up.36 While the time frame in these cases were shorter than the aforementioned study, both subjects demonstrated similar improvements in Penn shoulder scores, and met MCID with the use of BFR.
Limitations of this case series include the inclusion of only two subjects, as is typical of a case series, a short duration of care and follow up, and findings that may not translate to other patients presenting with SAIS. The case series design does not allow determination of cause and effect. Nonetheless, this case series is helpful in describing the clinical decision-making process and application of two patients with SAIS in whom treatment modification was considered necessary due to their high levels of irritability during the initial presentation.
CONCLUSION
Incorporating low load resistance training with BFR was demonstrated to be a useful adjunct for treating two patients with SAIS as it promoted exercise-induced hypoalgesia, a decrease in resting pain, and increase function in the upper extremity as noted by improvements subjectively and through patient reported outcomes. This case series describes clinically meaningful results when incorporating low load resistance training with BFR in patients with SAIS presenting with high levels of baseline irritability suggesting the need for consideration of modifications of recommended best practice for such patients. BFR was selected as the treatment modification as it has been associated with hypoalgesia and results in strength gains at lower intensities. BFR warrants further clinical consideration as an alternative intervention in patients who are unable to participate in standard of care secondary to pain and high levels of irritability.
Subject Consent
Subjects were informed prior to treatment that data concerning the case would be submitted for publication.
Resident’s Case Report
Case report was completed during University of Florida Health Sports Residency approved by the American Board of Physical Therapy Specialties (ABPTS)
COI
The authors have no conflict of interest to disclose.