INTRODUCTION
Hip-related pain is commonly associated with hip chondrolabral pathology, and typically presents as pain in the groin and anterior hip regions. It is a cause of reduced quality of life (QOL)1 and may progress to hip osteoarthritis (OA).2 The Doha agreement classified groin pain into five categories, the fifth being “hip-related pain”.3 More recently, a consensus paper has suggested that hip-related groin pain be further subdivided into three sub-categories; femoroacetabular impingement syndrome (FAIS), hip dysplasia and other (incorporating chondrolabral pathology).4 Changes in hip muscle function are associated with hip OA5–10 and FAIS,11–13 where greater hip muscle weakness and between limb asymmetry is associated with poorer function and lower hip-related QOL.9,14,15 Little is known about muscle function in patients with hip-related pain that do not have hip OA or FAIS (the ‘other’ category of Zurich agreement4). This information may inform rehabilitation providers to improve treatment outcomes for people with hip-related pain.
Hip movement and dynamic joint stability might reflect the complex interaction between superficial and deep hip muscles,16 however this interaction is poorly understood. Superficial muscles with large physiological cross-sectional areas and long lever arms can generate high forces,17 while deeper hip muscles are more suited to stability due to their morphology and proximity to the joint.16,18,19 Gluteus maximus (GMAX) and gluteus medius (GMED) are important prime movers of the hip,17 and commonly targeted in hip rehabilitation programs. GMED muscle size is impaired in people with advanced hip OA,5,7,8,10,20 however, beyond this, little is known about muscle size or structural changes within the muscle that may indicate reduced performance (i.e., fatty infiltrate that is lipid accumulation within the muscle belly) in people with non-OA hip-related pain.
Hip muscle function, particularly of the deeper hip muscles, is difficult to measure accurately. Segmenting specific muscle bellies and creating a three-dimensional likeness from magnetic resonance (MR) images is a reliable, non-invasive and valid method21,22 used to determine muscle volume. In addition, muscle volume may be used as a “proxy” for force generating capacity. There is some evidence that altered hip muscle volume is associated with hip-related musculoskeletal disease. For example, hip muscle volume is lower in those with high OA severity, but not in people with less severe OA.6,7 In women with chronic hip-related pain (including chondrolabral pathology and FAIS) and no hip OA, hip abductor muscle volume (determined by pooling GMIN, GMED, TFL and part of GMAX volumes) is larger than in asymptomatic controls, despite lower hip abductor strength.23
MR imaging also allows for the grading of fatty infiltrate within the muscle, which may be associated with disuse and influence muscle strength.24 Patients with hip OA have greater fatty infiltrate in GMIN and GMAX than healthy controls.8 Greater fatty infiltrate has been observed in people with knee OA,25 post whiplash disorder26 and cervicogenic headaches,27 compared to controls. Greater fatty infiltrate within lumbar multifidus in young athletes with lower-back pain is associated with less future sporting participation.28
Therefore, the purpose of this study was to (i) compare the volumes and fatty infiltrate of hip muscles (GMAX, GMED, GMIN, TFL, QF) between symptomatic and less-symptomatic sides of participants with hip-related pain; (ii) compare the volumes and fatty infiltrate of hip muscles between healthy controls and symptomatic participants; and (iii) explore the relationship of hip muscle volumes to muscle strength and patient-reported outcome measures (including pain, function and QOL) in individuals with hip-related pain.
Study design
This cross-sectional study was conducted the Laboratory for Movement Control and Pain Research at the University of Queensland and compared hip muscle volumes between individuals with hip pain and healthy controls. Ethics approval for the study was obtained from the University of Queensland (#2013001448). All participants provided a priori written consent.
Participants
Participants with hip-related pain were recruited from patients scheduled to undergo hip arthroscopic surgery for intra-articular hip lesions performed by a single surgeon (PW). All participants had engaged in non-surgical management (including hip muscle strengthening) prior to being assessed, in order to be eligible for surgical management. Participants were invited to participate via mail prior to the planned hip arthroscopic procedure. Healthy control participants were recruited from the Brisbane community via advertisements in the media and posters. To be eligible, participants with hip-related pain and healthy controls were required to be aged between 18 to 60 years and be able to walk and ascend/descend stairs without aid. Participants with hip-related pain were included if they had: (i) persistent hip/groin pain (>3 months) reproduced by physical activities (e.g., walking, stair climbing), and positive physical examination findings in hip joint provocation testing (combined hip movements; Flexion-Adduction-Internal Rotation test and Flexion-Internal Rotation); (ii) the treating surgeon determined that they did not have FAIS based on imaging findings, clinical signs and symptoms. Where participants had bilateral hip-related pain, the hip scheduled for arthroscopic surgery was deemed the study hip. Control participants were included if they: (i) had no current lower limb or low back pain; (ii) no history of hip/groin pain in the prior 12 months or previous hip surgery. The exclusion criteria for all participants included the following: (i) contraindications for MR images and (ii) inability to understand written and spoken English. The control participants were age, gender and body mass index (BMI) matched, as closely as possible, to the hip pain participants.
Procedure
A single investigator (TR) not blinded to group but blinded to the side of hip pathology in hip pain participants, performed all physical measures.
Participant characteristics
Age, gender, leg dominance, height, and weight data were collected, and BMI was calculated. All participants provided a written informed consent prior to data collection.
Hip muscle strength testing
All participants underwent hip muscle strength testing on both limbs. Isometric hip abduction, adduction, internal rotation, external rotation and extension strength were measured (in that order) using a Commander Power track II handheld dynamometer (JTECH Medical Industries, Midvale, UT, USA). The investigator resisted the movement in the contraction direction and provided feedback to the participant to increase their force over ~2 seconds to their maximum, and then hold for ~3 seconds before returning to rest. Each direction was assessed three times, with 10 seconds rest between each test. This method has been previously proven to be reliable.29–31 Maximum strength data (single maximum trial) were converted to torque values using the lever arm measurement (N.m).31
Magnetic resonance imaging acquisition
Hip MR images were taken at a private radiology clinic (Queensland X-Ray, Coorparoo, Queensland) with a standardized protocol, optimized for visualization of cartilage and muscle morphology on a 3T Siemens Medical MRI scanner (Siemens Healthcare, Erlangen, Germany) and read by a single radiologist. Dedicated hip flex coils and sequences are designed to provide very high-resolution imaging with the ability to detect early chondral loss and optimize viewing of muscle volumes. A large field of view axial T1 weighted sequence was performed to permit muscle segmentation. Sequences obtained included coronal proton density with and without fat saturation; axial and axial oblique proton density fat saturated sequences and sagittal proton density fat saturated sequence.
Measurement of hip muscle volumes
The volumes of the GMAX, GMED, TFL and QF were measured on axial MR images by manually segmenting muscle boundaries using commercially available software (Amira 6.3.0 FEI, part of Thermo Fisher Scientific, Hillsboro, Oregon, USA). GMIN volume was not included in the analysis of this study as the quality of the images (fascial borders) did not easily allow for measurement along the entirety of the muscle. For each muscle, the cross-sectional areas were summed, and the total sum was multiplied by the slice thickness to obtain the muscle volume. A trained investigator (HH), who remained blinded to the study groups, performed all segmentations. The research team determined the intra-rater reliability of the muscle volume measurement technique to be excellent (ICC 0.995-0.997) by completing segmentation of five MR images twice, consistent with previously established inter-rater reliability (ICC 0.87-0.99).6,7
Rating of fatty infiltration
A single assessor (AS) graded the degree of fatty infiltration using the Goutallier classification system.32 This system has good inter-rater (ICC=0.9) and intra-rater reliability (weighted kappa 0.72-0.81)8,33 for hip muscles. This system rates each muscle from 0 (normal muscle) to 4 (more fat than muscle) (Table 1). These values were then dichotomized to indicate no fatty infiltration (score of 0 and 1), or fatty infiltration (2 or more). The landmarks used for grading each muscle have been reported previously.24 Briefly, GMIN, GMED and upper GMAX were each assessed on axial images at the level of the greater sciatic foramen, and 2/3 the distance from the top of the iliac crest to the proximal tip of the greater trochanter. They were further divided into two equal segments consistent with previous studies.34–36 The average of the Goutallier scores across the three sections of GMIN, GMED and upper GMAX indicated the level of fatty infiltrate for each muscle. TFL was assessed at the level of the fovea capitus, and QF was graded at the level of the largest cross-sectional area.
Patient-reported outcomes
Participants in the hip pain group were administered several questionnaires including the International Hip Outcome Tool (iHOT-33),36 the Hip Dysfunction and Osteoarthritis Outcome Score (HOOS),37 the Arthritis Self Efficacy (ASE),38 the Tampa Scale for Kinesiophobia (Tampa),39 the Hospital Anxiety and Depression Scale (HADS),40 the Tegner Activity Level Scale (TAS),41 the Visual Analogue Scale (VAS),42 the Pain Catastrophizing Scale (PCS)43 and The Photograph Series of Daily Activity (PHODA).44 The questionnaires were either filled in electronically or via paper-based forms, depending upon preference.
The HOOS and iHOT-33 were used to assess health-related symptoms and function. The HOOS consists of five subscales on pain, symptoms, function in activities of daily living (ADL), sport and recreation function (Sport/rec) and hip-related QOL. A normalized score is calculated for each subscale (0 to 100), where 100 indicates no hip-related limitations, and zero indicates maximum hip-related limitations. The iHOT-33 measures symptoms and functional limitations, sports and recreational physical activities, job-related concerns and social, emotional, and lifestyle concerns on a scale from 0-100, with 0 indicating maximum hip-related limitations. The ASE was used to assess perceived confidence in ability to perform behaviours that would modify joint pain on a scale from 1-10. A score of 10 on ASE indicates the optimal score. The Tampa scale quantifies fear of movement and re-injury due to movement and physical activity. It consists of 17 statements of subjective experience of injury and activity on a scale from 0 to 68, where a score of 68 indicates greater fear of re-injury due to movement. The PCS, a 12-item instrument, was used as a measure of perception of pain on a scale between 0-52 for the total score. The PCS sub scales of Rumination (0-16), Magnification (0-12) and Hopelessness were also used. For all the PCS items, 0 is the optimal score. Physical activity level was assessed using the TAS with a scale from 0-10, where a score of 0 is where a participant is on sick leave or disability pension because of their hip problems and 10 is a participant performing as a nationally elite sportsperson. Participants were also asked to rate their average daily pain over the last week and the worst pain they experienced in the last week on separate 10cm VAS. The scale was anchored by “no pain” (score of 0) and “worst pain” (score of 10). Anxiety and depression were assessed using the HADS. The Anxiety and Depression sub scales are both scored from 0-21 where scores in the range 0-7 are normal. Perception of the harmfulness of daily activities was assessed using the PHODA, a questionnaire involving scoring 40 photographs of activities from ‘not harmful’ at all to ‘very harmful’ along a 10 cm horizontal line. The questionnaire is scored between 0-100 with 0 the optimal score.
Statistical analysis
All data were analysed with the Statistical Package for the Social Sciences (SPSS Statistics Version 21, IBM Cooperation. Armonk, NY). All data were normally distributed, therefore parametric tests were used. Between-group differences in participant characteristics were assessed using independent t-tests or chi square tests as appropriate. To control for the influence of body size, muscle volumes and muscle strength were normalized to body mass. In the hip-related pain group, the muscle volumes were compared between the symptomatic and less-symptomatic limbs with paired t-tests. To evaluate between-group differences in muscle volumes, the data from the most symptomatic hip from the hip pain group was compared to the data from the matched hip from the control group using One Way Analysis of Co-Variance (ANCOVA) with gender as a co-variate.45 To determine if differences in fatty infiltrate exist between the more and less symptomatic leg, the McNemar’s test was used for paired data. When comparing fatty infiltrate between the symptomatic limb of the hip-related pain group and matched healthy controls, Fishers exact test was used for non-paired data. Within the hip-related pain group (n=16), eight reported greater pain on their dominant limb, while eight had greater pain on their non-dominant limb. As such, to match the groups for dominance, the data is reported from the dominant side of eight, and the non-dominant side of seven of the healthy controls (n=15). Spearman’s ρ correlation analyses were performed to determine the relationship of hip muscle volumes to patient-reported outcome measures (hip-related pain group) and to determine the relationship of hip muscle volume to hip muscle strength. Correlation coefficients (ρ) were classified as follows: 0 to 0.25, little or no relationship; 0.25 to 0.5, fair degree of relationship, 0.5 to 0.75 moderate to good relationship; and 0.75 to 1.0, good to excellent relationship.46 Significance was set at p<0.05.
RESULTS
Participants’ characteristics
Between April 17, 2014 and April 14, 2015, 16 participants with hip-related pain (eight with greater pain on the dominant limb) and 15 healthy controls were invited to participate in this study. All participants were part of a larger cohort study.31 There were no statistically significant differences in participant characteristics between the hip-related pain and control groups (Table 2). In the hip-related pain group, 11 participants (69%) underwent arthroscopic surgery in the year after testing – of these, 100% had chondrolabral pathology at hip arthroscopy. Participants with hip-related pain had moderate to severe limitations due to hip-related pain (Table 3).
Comparisons of hip muscle volumes and fatty infiltrate
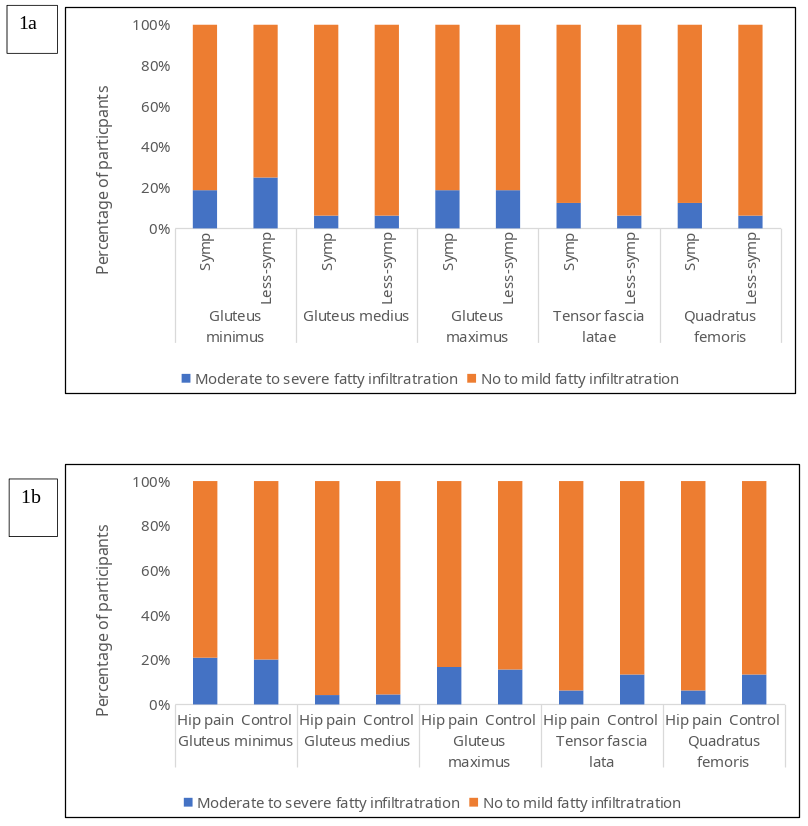
There were no statistically significant differences in GMAX, GMED, TFL and QF muscle volumes nor fatty infiltrate between symptomatic and less-symptomatic limbs in individuals with hip-related pain (Table 2 and Figure 1a), or between hip-related pain and control participants (Table 2 and Figure 1b).

Hip muscle volumes and patient-reported hip-related limitations
There were moderate to good associations between GMED muscle volumes and hip-related patient-reported outcomes in individuals with hip pain (Table 3). Those with greater GMED muscle volumes had less symptoms (HOOS-symptoms: ρ=-0.566 p=0.04, i-HOT-33 symptoms: ρ = -0.591, p=0.03) and greater function (HOOS-ADL: ρ = -0.522, p=0.05, HOOS-Sport/rec: ρ = -0.552, p=0.04), social health status (i-HOT-33: ρ =-0.579, p=0.04) and QOL (HOOS-QOL: ρ = -0.617, p=0.02). There were no significant associations between GMAX, TFL and QF muscle volumes, and patient-reported outcome measures.
Hip muscle volumes and muscle strength
There were several significant associations between hip muscle volumes and strength in individuals with hip-related pain (Table 3). Greater GMAX volumes correlated with greater hip abduction (rho= 0.624, p=0.01) and internal rotation (rho= 0.507, p=0.045) strength. Those with greater hip GMED volumes had greater hip extension strength (rho= 0.547, p=0.03) and those with greater QF volumes had greater hip abduction strength (rho= 0.638, p=0.008).
DISCUSSION
The results of this study determined that people with hip-related pain and no clinical signs of FAIS, who were scheduled for hip arthroscopy, had no difference in volume for the muscles measured in the study on the symptomatic limb when compared to their less-symptomatic limb or matched healthy controls. There were also no differences in hip muscle fatty infiltrate between symptomatic and less-symptomatic hips or when compared to healthy controls. In the hip-related pain group, reduced GMED muscle volume correlated with poorer function (HOOS-ADL and HOOS-Sport/rec), symptoms (HOOS-symptoms and i-HOT-33 symptoms) and QOL (HOOS-QOL). Smaller muscle volume of GMAX was associated with lower abduction and internal rotation strength, smaller QF volume with lower hip abduction strength and smaller GMED volume with lower hip extension muscle strength.
Hip muscle volume
Lack of muscle volume differences (both between groups and between limbs in the hip-related pain group) is unexpected given the known hip muscle strength deficits in this population,31 and in people with FAIS.12 This finding was consistent with findings of no differences in muscle volumes in people with mild OA6,7 and women with hip-related pain,23 with only one prior study reporting smaller muscle volumes in 50 people with unilateral FAIS.47 It is possible that muscle volume differences only become evident in those with moderate to severe hip OA.6–8 Direct comparisons with prior studies are hampered by key differences in methodology, for example normalizing muscle volume for weight and pooling of muscle groups.23 The current results strengthen the notion of a continuum of hip pathology where younger people with less severe symptoms and/or less marked joint changes have hip muscle weakness but no change in muscle size. As the symptoms and joint degeneration progress, measurable muscle volume changes may occur.
Hip muscle volume in participants with hip-related pain cannot fully explain the observed hip muscle weakness. Pain inhibition might explain the strength deficit, but a prior report by this group found no association between muscle strength and patient reported pain.31 Changes in the motor control of the hip muscles may provide an alternative explanation. Although no studies to the authors’ knowledge have investigated changes in motor control in people with hip-related pain with no FAIS, there is a growing body of research investigating motor control changes in people with hip-related pain with FAIS.48–50 Results from these studies report changes in the timing and activation of the deep hip muscles with functional movements such as squatting and walking. It is unclear whether these other findings could be interpreted as a strategy to reduce hip impingement or another mechanism.48–50 Studies of other peripheral and axial joints in patients have demonstrated selective changes in muscle function associated with joint pain; including timing of onset and cortical representation of these muscles.51–55 Specific strategies for hip rehabilitation could be explored in future studies.
Fatty infiltrate
Muscle fatty infiltrate appears to be rarely evident in people with hip-related pain. Similar to hip muscle volume, muscle fatty infiltrate may be a sign of disuse accompanying advanced joint disease, greater BMI9 or aging.24 While the current findings indicated no difference in fatty infiltrate between limbs or between groups, further studies of fatty infiltrate in different groups with varying disease severity are warranted.
Muscle strength
Greater hip muscle volumes were moderately associated with higher muscle strength, especially hip abduction strength. Hip abductor strength will be influenced by the primary synergists, the upper portion of GMAX, GMED, GMIN, and TFL. Furthermore, the deep hip external rotators (including QF) have been shown to be active during hip abduction,18,56 potentially contributing to efficient force transfer from the more superficial lateral muscles. Strengthening programs that target all synergistic hip abductors and hip stabilizer muscles may be important for the restoration of normal muscle function at the hip joint.
Patient reported outcomes
Lower GMED volume was associated with greater symptoms, poorer function in sport and activities of daily living (HOOS, i-HOT-33) and lower QOL. The mechanism explaining how smaller muscle volume might affect patient reported outcomes is unclear, and it is possible that greater symptom severity is the driver of disuse and smaller muscle volume. Rehabilitation strategies targeting hip muscle size and strength deficits are certainly justifiable in this population. But, the moderate levels of symptoms, patient-related disability, kinesiophobia and lower than normal QOL may indicate that a more holistic approach is required. This may include patient information and advice, aerobic exercise and for some with fear avoidance and unhelpful beliefs about pain, more specific cognitive training.57 Patient information and advice needs to be tailored to the patient, with recent qualitative research indicating that patient expectations, active coping strategies, information about structure and pain, and appropriate guidance on returning to physical activity may be important.57–59
Limitations
The study had several limitations in addition to the relatively small sample size. Although the hip group had clinical and radiographic evidence of hip pathology, it is difficult to be absolutely certain that the participants in the hip-related pain group had pain coming from the hip joint. A limitation of the within-subject comparisons was that one participant in the hip-related pain group had bilateral symptoms. In this case, the comparison was most symptomatic to less symptomatic, not symptomatic to asymptomatic. In addition, the recruitment of the participants with hip-related pain from only one surgeon may have led to selection bias. The cross-sectional study design means temporal and causative relationships cannot be established. Further, although there were not statistically significant differences between the groups, the healthy control group was on average six years younger than the hip-related pain group. This age difference may reduce the strength of the conclusions that can be made about hip strength and hip muscle volume. Some, but not all, of the superficial and deeper hip muscles were examined. The study may have been strengthened by including superficial muscles such as the hip adductors and flexors which have been shown to be weak in people with hip-related pain60 and other deeper hip muscles such as iliocapsularis which may have an important stability role in movement and gait.50,61 Lastly, while all of the participants had engaged in non-surgical management, there were no records of program duration, or how much hip-muscle strengthing was performed, therefore the authors cannot be certain whether the pre-operative management may have had an influence on the study findings.
CONCLUSION
Individuals with hip-related pain and no clinical FAIS have hip muscle volumes and hip muscle fatty infiltrate that are not significantly different to matched healthy controls or to their less-symptomatic limb. Smaller muscle volume of GMAX was associated with lower abduction and internal rotation strength, smaller QF volume with lower hip abduction strength and smaller GMED volume with lower hip extension muscle strength. Smaller hip muscle volume, particularly of GMED, was associated with poorer hip function, greater symptoms, and lower QOL. This information may inform rehabilitation professionals programs to improve treatment outcomes for people with hip-related pain.
Conflicts of interest
The authors report no conflicts.
Funding
The authors acknowledge Wesley Medical Research, Brisbane, Australia for financial support of this study.