INTRODUCTION
Orthopedic surgeons are the third highest opioid prescribers among all physicians.1 Opioids are routinely prescribed for pain relief during the postoperative recovery process after orthopedic surgery. In recent years, regulatory agencies, including state governments, have enacted initiatives to decrease the use of opioids in the perioperative setting. These include legislative reforms,2,3 institutional reforms such as educational programs and prescribing guidelines,4,5 and physician-led practice-based reforms. Recent evidence suggests that state-level legislation is effective in decreasing opioid use in the postoperative period for patients undergoing orthopedic procedures.6–9 Orthopedic patients traditionally have the most in-person ‘face time’ with their clinicians. Therefore, orthopedic surgeons can have a direct role in not only patient education, but also in improving pain management strategies and decreasing the opioid burden on society.10,11
The use of opioids for pain management after major surgery has been linked to subsequent prolonged opioid dependence.12,13 As a result, the growing concern for opioid misuse and abuse has increased in the general public. Thus, reducing postoperative pain by other means could decrease opiod consumption.14 Apart from counselling patients and establishing reasonable expectations for pain control as part of the treatment plan, several non-opioid alternative strategies exist for pain management. Physical therapy may be used to increase exposure to nonpharmacological treatments for people with musculoskeletal pain conditions.15 In recent practice guidelines, nonpharmacological treatments have been emphasized for initial pain management of musculoskeletal pain, and physical therapists are providers who routinely deliver nonpharmacological treatments such as ice, heat, tape and therapeutic exercise.15 Additionally, same day physical therapy following orthopedic surgery leads to decreased inpatient opioid consumption.16 Therefore, it may be possible that, if implemented in addition to regularly scheduled physical therapy, these non-pharmacologic interventions can provide sufficient postoperative pain relief to reduce opioid use.
Cryotherapy, a common recovery modality easily used at home, has consistently been shown to alleviate pain.17–20 Cryotherapy works to reduce pain by reducing skin surface temperature, which can promote a reduction in nerve conduction velocity.21 A popular, and sometimes more user friendly, substitute to cryotherapy is Biofreeze.22 Biofreeze is a menthol-based superficial cooling product which has previously been shown to effectively reduce pain in a variety of musculoskeletal conditions.23,24 Although the active ingredient in Biofreeze, menthol, does not lower tissue temperature, it stimulates cold thermoreceptors25–28 through a chemical reaction resulting in pain relief 29 through a counterirritant effect.30 Heat packs are also commonly utilized at home when individuals seek comfort and pain relief.31–34 Ultimately both cold and hot modalities provide an analgesic effects and successfully, albeit temporarily, reduce pain.
Other alternative recovery modalities capable of indirectly reducing pain include elastic adhesive tape and elastic resistance exercises. Elastic adhesive tape, commonly known as kinesiology tape, is superior to minimal intervention for pain relief, but this effect does not hold true when compared to other treatment approaches in individuals with chronic musculoskeletal pain.35 Conversely, elastic resistance exercises involve the participation of the patient, and are commonly used to build strength, increase range of motion, and reduce pain in the physical therapy setting. Although potentially counterintuitive to individuals experiencing symptoms of pain, elastic band exercises can be low-impact and when dosed appropriately will not exacerbate pain. Elastic resistance exercises have been shown to reduce pain and improve range of motion in knee arthroplasty patients.36 In general, exercise programs that improve one’s strength not only lessen pain but also improve functional ability.37,38
Nonpharmacologic therapies might be of greater interest to the patient concerned with, or opposed to taking opioid medication, and could potentially provide a comparable analgesic effect, particularly if used in a multimodal pain management strategy. Therefore, the purpose of this study was to determine the effect of a multimodal non-pharmacological ‘pain relief kit’ on pain, function and opioid medication consumption in individuals recovering from orthopedic surgery. It was hypothesized that patients who were provided with the pain relief kit would consume less opioid medication, report lower pain levels, and have better functional outcome scores than the control group.
METHODS
Patients were included in the study if they underwent an orthopedic surgery that included bone drilling as part of the procedure. Exclusion criteria for this study included any patient who was currently already taking opioids or had a history of alcohol or substance abuse. Based on the variability between patients in opioid use after total knee arthroplasty39 and ACL reconstruction,40 it was estimated that with 25 patients per group there would be 80% power to detect a 60% lower use of opioids in the pain relief kit group at p<0.05.
Patients were randomized to receive either standard care without (control) or with the addition of the pain-relief kit (treatment). The treatment duration was four weeks, beginning on the first postoperative physical therapy visit which took place within one week post-op. Patients in the control group received usual care in the clinic but did not receive any components of the pain relief kit as part of their home program. The treatment group received standard care in addition to the pain relief kit. Treatment group patients were shown how to properly use each item in the kit at the first physical therapy visit. All patients were prescribed physical therapy two to three days per week. Patients kept a daily log of the volume and rate of opioid and non-opioid pain medication consumption, VAS pain score, and a log of compliance with each of the items in the pain relief kit (if in the treatment group). All patients completed the Short Form 36 Health Survey Questionnaire (SF-36) questionnaire in addition to DASH (Disabilities of the Arm Shoulder and Hand) scores for upper extremity procedures, or the LEFS (Lower Extremity Functional Scale) scores for lower extremity procedures at baseline or the first post-op physical therapy visit and at four weeks post-op.
NON-OPIOID INTERVENTION - PAIN RELIEF KIT
Each item in the pain relief kit was recommended to be utilized up to three times daily or every 6-8 hours. Joint specific exercises were initially performed against gravity and progressed to elastic resistance using yellow and then red TheraBands (Theraband Akron, OH, USA).
BioFreeze Roll-On 4% menthol (BioFreeze Warrenville, IL, USA) was recommended to be applied during the morning hygiene routine or up to 3 times throughout the day in response to pain. Additionally, it was recommended to be applied five minutes prior to and following exercise or any other moderate intensity activity. Kinesiology tape was recommended to be applied to the affected area at 25% elongation and reapplied every three days or as needed when tape failed to adhere. Upper extremity patients were instructed to apply the tape across the trapezius in accordance with tightness or pain and lower extremity patients instructed to apply the tape along the quadriceps. Thermal Therapy [warm or cool was delivered using the TheraPearl (Bausch & Lomb Inc., New York, USA)], was recommended to be applied during the morning hygiene routine and as needed throughout the day in response to pain. Application of heat was recommended for 30 minutes prior to engaging in exercise and application of cold was recommended for 20 minutes following exercise.
DAILY MEDICATION LOG
Most patients were prescribed oxycodone/acetaminophen (5 mg/325 mg) to be taken every six hours as needed. Six patients were not prescribed oxycodone, instead four were prescribed hydrocodone/acetaminophen, and two Tramadol. Patients were asked to keep a daily log of prescription and non-prescription analgesics taken. Opioid use is reported in this research as Milligram Morphine Equivalent (MME) or the amount of morphine in milligrams equivalent to the strength of the opioid dose prescribed.
DAILY PAIN LOG - Visual Analog Scale (VAS)
Perceived pain was recorded daily using a 10 cm VAS with anchor statements on the left (no pain) and on the right (extreme pain).41 The VAS is widely accepted as a reliable standard for self-reporting of pain post operatively for a wide range of surgical and orthopedic procedures in a clinical setting.42–45 The patient was asked to mark their average pain over the previous 24 hours on the line at the same time each day.
OUTCOME SCORES
Lower Extremity Functional Scale (LEFS)
Lower extremity outcomes were evaluated using the LEFS. The LEFS is a self-report questionnaire that asks patients to answer the question “Today, do you or would you have any difficulty at all with:” in regard to twenty different everyday activities. The LEFS has shown sufficient reliability to administer and is applicable for research purposes and clinical decision making for individual patients.46
Disabilities of the Arm, Shoulder and Hand (DASH)
Upper extremity outcomes were evaluated using the DASH. The DASH outcome measure is a 30-item, self-report questionnaire designed to assess the patient’s health status. The DASH questionnaire is used as an indicator of the impact of an impairment on the level and type of disability. It assesses the whole person’s ability to function, even if the person is compensating with the other limb. Beaton et al.47 has shown strong validity, test-retest reliability, and responsiveness of the DASH questionnaire in both proximal and distal disorders of the upper extremity, confirming its usefulness for assessing disability in the upper extremity.
Short Form 36 Health Survey Questionnaire (SF-36)
Patients’ global rating of health status and quality of life was assessed using the SF-36. The SF-36 is a self-reported questionnaire evaluating eight aspects of the patient’s perception of health: physical functioning, bodily pain, role limitations due to physical health problems, role limitations due to personal or emotional problems, emotional well-being, social functioning, energy/fatigue, and general health perceptions. The SF-36 has been widely validated and has been shown to have high reliability for measuring health perception in a general population.48
STATISTICAL ANALYSIS
The effects of the pain relief kit on opioid use, over the counter pain medication, VAS pain scores, functional outcome scores, and SF-36 scores were assessed using mixed model analysis of variance with repeated measures for time (weeks 1-4) and treatment as a between-subjects factor (pain-relief kit versus control). Within the treatment group the relationship between use of the pain relief kit and opioid and non-opioid medication use was assessed using the Pearson correlation coefficient. Difference in opioid use between patients having arthroplasty versus other procedures was tested using an independent t test.
RESULTS
There were 28 patients in the pain-relief kit group (9 women, 19 men) and 25 in the control group (9 women, 16 men). Twelve patients had total joint arthroplasty (4 pain-relief kit, 8 control) and the remaining 41 patients (24 pain-relief kit, 17 control) had various procedures requiring bone drilling (23 ACL reconstructions, 12 shoulder arthroscopies, two other knee procedures, three elbow procedures and one ankle procedure). Procedures performed on the patients in the pain relief kit group included 15 ACL reconstructions, four arthroplasties, seven shoulder arthroscopies, and two other procedures (n=28). The patients in the control group included eight ACL reconstructions, eight arthroplasties, five shoulder arthroscopies, and four other procedures (n=25). There were three dropouts in the control group and none in the pain relief kit group. Data are reported for the remaining 50 patients (28 treatment, 22 control). The treatment group was younger than the control group (31±18 yrs vs. 45±20 yrs, p=0.015). Groups were not significantly different in body mass (75.8±20.9 kg vs. 77.6±25.9 kg, p=0.822) or height (1.71±0.12 m vs. 1.72±0.13 m, p=0.851).
Compliance with the pain-relief kit varied between the different components, with the elastic resistance exercises having highest compliance (4±3 days per week) followed by the topical heat treatment (3±3 days per week), BioFreeze (2±2days per week) and the elastic tape treatment (1.5±1 days per week). Use of pain-relief kit was not correlated with opioid (r=0.211, p=0.280) or non-prescription pain medication use (r=0.053, p=0.715), or the combination of opioid and non-prescription pain medication use (r=0.076, p=0.602).
There was no statistically significant difference in total opioid use between the treatment group (108±252 MME) and control group (132±158 MME; p=0.696) over the four weeks of the study. Opioid use declined from week one to week four (Time effect p<0.001) with no difference between groups (Treatment by Time p=0.982). Non-opioid pain medication (p =0.24) and total medication (p=0.20) were not statistically significantly different between groups. Thirteen of 28 patients in the pain relief kit group (46%) and nine of 22 patients in the control group (41%) did not use any opioid medication.
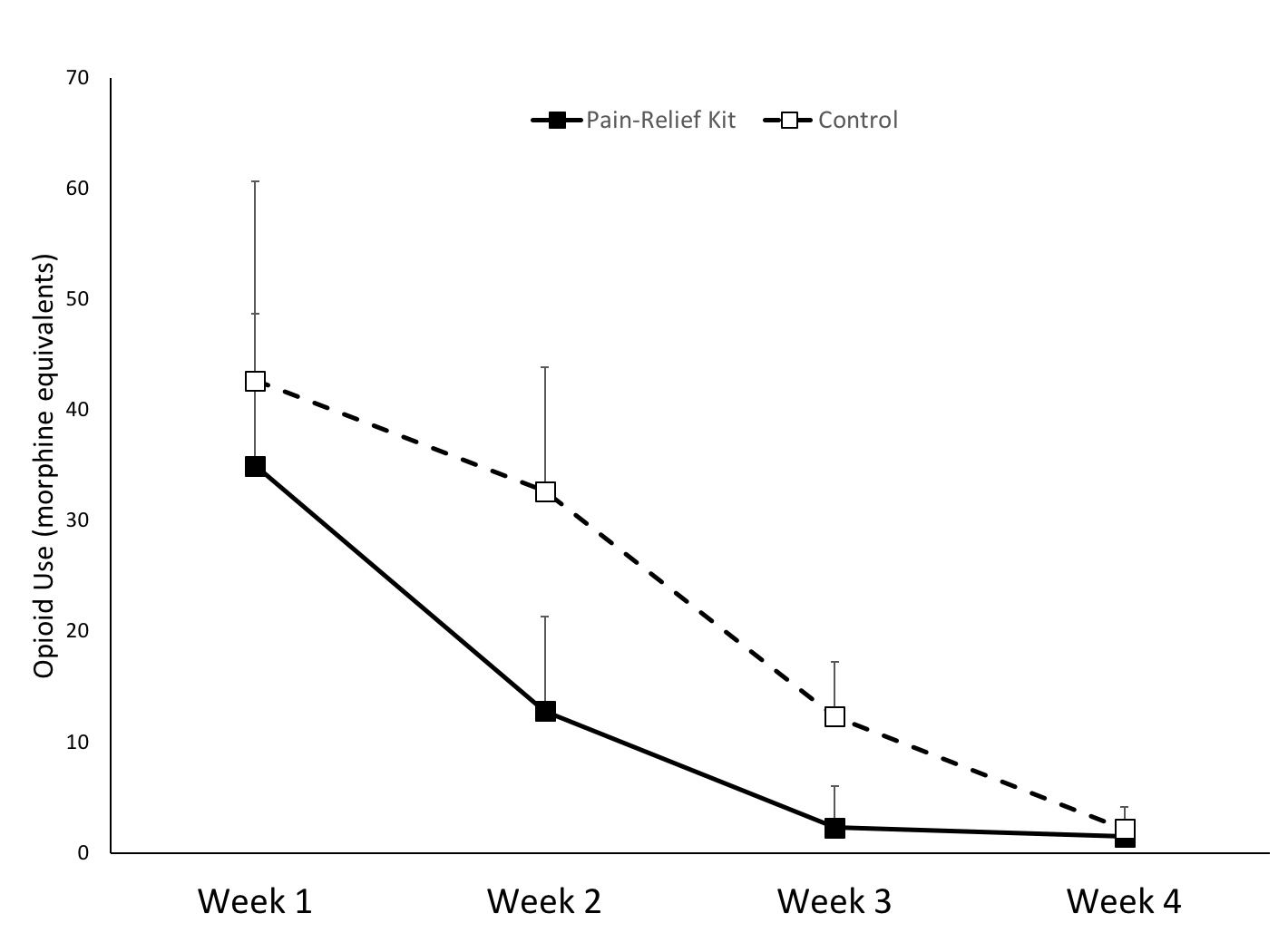
Opioid use was much higher in the 12 patients who had total joint arthroplasty (285±340 MME) versus those with other procedures (66±120 MME; p<0.049). The sample size (12) was too small to statistically analyze the effect of the pain relief kit treatment in the patients who had total joint arthroplasty. Opioid use for the remaining 38 patients was analyzed separately (Figure 1). For these 38 patients opioid use declined over the four weeks of the intervention (p<0.001) with no statistically significant difference between the pain relief kit group and control group (Treatment effect p=0.352, Treatment by Time p=0.653).

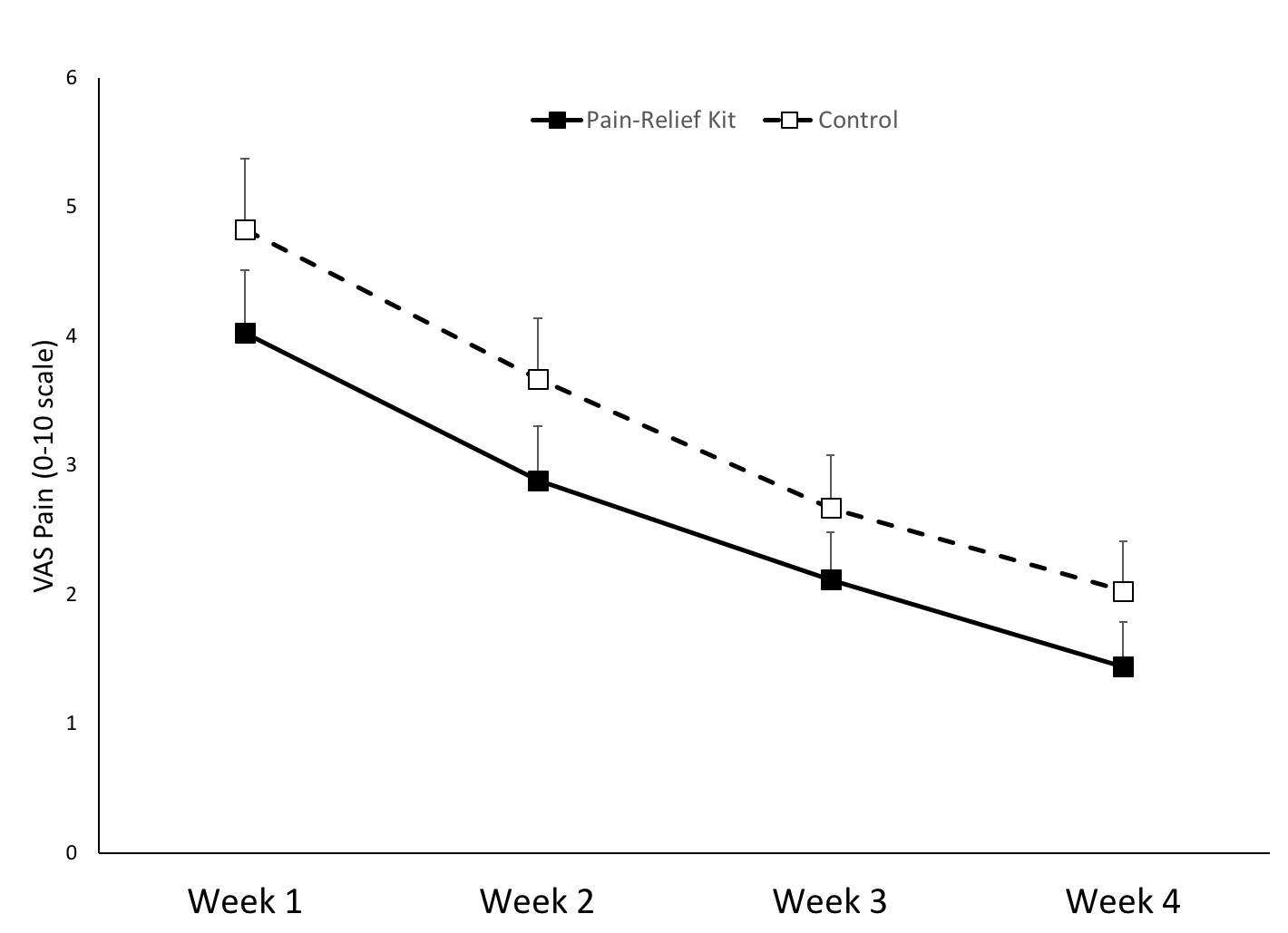
Pain declined steadily from week one to week four (p<0.001; Figure 2) with no significant difference between the pain-relief kit group and controls (Treatment effect p=0.205, Treatment by Time p=0.942).
Outcome scores also improved from week one to week four (p<0.001) with no difference between the pain-relief kit group and controls (Treatment effect p=0.788, Treatment by Time p=0.277). SF-36 scores improved from week one to week four (p<0.001) with no difference between the pain-relief kit group and the control group (Treatment effect p=0.272, Treatment by Time p=0.427).

DISCUSSION
This study investigated the effect of a multimodal pain relief kit on pain, patient reported outcomes, and opioid consumption in the four week period following various orthopedic surgical procedures. Contrary to the hypothesis, opioid use was not different between the pain relief kit group and the control patients. Furthermore, there was no difference in the VAS pain scores, SF-36, and outcome scores between the pain relief kit and control groups. Both groups had similar declines in pain and improved outcomes over the four weeks after surgery.
The ability to detect a reduction in opioid use with the pain relief kit may have been affected by lower than expected opioid use in these subjects. Dwyer et al.39 reported opioid use of 851±607 MME over two weeks after total knee arthroplasty. Total opioid use in the present study for the 12 patients who had joint arthroplasty was 285±340 MME. Similarly, Forlenza et al.40 reported opioid use of 349±256 MME over 15 days after ACL reconstruction. In the present study opioid use for patients that had procedures other than arthroplasty was 65±120 MME. The combination of a lower-than-expected opioid use and a higher than estimated inter-subject variability in opioid use likely indicates that there was insufficient power to detect an effect of the intervention. The high variability in opioid use was due to a substantial proportion of patients (44%) not taking any opioids during the four weeks of this study. Since this was a physical therapy-driven intervention the pain relief kit was introduced on the patient’s first visit for physical therapy. This occurred on average 8±6 days after surgery, during which time opioid use would have been highest. However, time from surgery to enrollment in the study at first physical therapy visit was not correlated with opioid use (r=-0.029, p=0.841). This indicates that patient-related factors drove opioid use in this study rather than the delay between surgery and study enrollment. The fact that so many patients did not take opioids indicates that the public awareness of the risks associated with opioid use may have been a factor.
A second issue to consider in assessing the lack of effectiveness of the pain relief kit is the compliance with the multimodal approach. The four-pronged intervention was in addition to all that was expected in physical therapy. The in-person physical therapy visits alone (two to three times per week) may have reduced pain to an extent that the addition of four pain relief strategies (used on average on two to four days in the week) did not provide further pain relief. As would be expected there was a 50% reduction in pain from week one to week four for both groups.
Postoperative pain control with a non-opioid pain regimen consisting of ibuprofen, acetaminophen, and other common anti-inflammatory agents has been successfully achieved in patients undergoing commonly performed orthopedic arthroscopic procedures.49,50 Gimbel et al.50 demonstrated that patients prescribed only a nonsteroidal anti-inflammatory drug experienced greater pain relief and fewer adverse events than those prescribed opioid analgesia after ambulatory orthopedic surgery. Similarly, Daniels et al.5 concluded that 82% of patients who undergo arthroscopic partial meniscectomy and/or chondroplasty can achieve satisfactory pain control with non-opioid pain management. A majority of patients undergoing arthroscopic procedures might be successfully managed with a non-opioid pain medication, including ibuprofen and other common anti-inflammatory agents. It remains to be determined if a pain relief kit such as that employed in this study could help reduce use of non-opioid pain medication where opioids are not being prescribed.
There is evidence to support the use of cryotherapy to reduce pain following orthopedic surgery.51–55 Ice or cold-water recirculation is a mainstay of outpatient care after knee arthroscopic surgery and can effectively reduce reported pain without increased risk of adverse events.56 However, neither were shown to be effective after elective total knee arthroplasty.57,58
Conversely, there is a paucity of evidence on the use of heat packs on pain control or opioid consumption following orthopedic procedures. Nevertheless, the participants in the treatment group of the present study utilized the heat pack at a greater rate per week compared with the topical analgesic (3.0±2.6 vs 2.0±1.7 days per week). There still was no difference in the pain management whether they used heat or cold.
The elastic bands were the most frequently used tool in the pain kit (3.8±2.5 days/week). Elastic resistance exercises are very commonly integrated into the physical therapy routine following both arthroscopic and arthroplasty procedures. The study participants received exposure to this intervention during their physical therapy, and thus they felt most comfortable using it. Strength training exercises, implemented shortly following arthroplasty, have proven to be feasible without exacerbating postoperative symptoms such as pain,59 and the elastic bands are a user-friendly way for patients to perform their resistance exercises at home. However, the extent to which the use of elastic bands following orthopedic procedures might reduce opioid use has not been examined.
Ultimately, physical therapy itself has been shown to decrease inpatient opioid consumption following orthopedic surgery16As there was no difference in total opioid use between the treatment group and control group of the present study over the four week follow up period, it is possible that the patients simply benefitted from their physical therapy sessions and there was no added benefit of the pain kit. However, this analysis was beyond the scope of this study. Further, it seems that the timing of physical therapy following surgery matters most.16 In a recent review Brown-Taylor et al. concluded that although early physical therapy reduced subsequent opioid use there is limited and inconclusive evidence to establish whether the content and/or location of the physical therapy interventions improves outcomes because of heterogeneity between studies.60
This study is not without limitations. The variability in opioid use between patients was much larger than expected and significantly limited the power to detect a difference between the treatment groups. For the patients who had procedures other than total joint arthroplasty the overall opioid use was much lower than expected. There were various levels of usage of the individual modalities within the kit across the patient population, with no one modality being preferred by all patients. It is possible that the outcome would have been more beneficial towards the pain kit had the researchers controlled for frequency of use of all modalities to make their use even across all participants. However, the approach taken in this study was intended to observe how patients choose to manage their own pain using recovery modalities.
Finally, the treatment group was significantly younger than the control group. Previous research60 suggests that younger patients (in the age range of 30-39 years) had a significantly higher reported mean opioid consumption for joint procedures compared with older patients (80-89 years), while the youngest adult patients (18-19 years) who received treatment for fracture fixation reported the highest mean consumption. Given the limitations of the present study, further research is necessary to investigate how other alternative pain-relieving modalities could be applied in clinical practice to reduce opioid use and possibly reduce use of non-opioid medications.
CONCLUSION
The results of this study indicate that there is no difference in post-operative opioid consumption in a group who utilized a multimodal pain kit as compared to the control group. This non-pharmacological pain relief kit did not significantly reduce opioid use in this patient population. In general, opioid consumption was very low over the four weeks following surgery and both groups displayed marked symptom relief over the four weeks of the study. While the public’s awareness of the opioid epidemic will help further reduce opioid use over time, it is important to continue to search for alternative pain control methods for patients.
Conflicts of Interest
All authors declare that they have no conflicts of interest.