
Introduction
Hamstring injury is a common muscle injury that affects many athletes associated with various sports.1–3 It has been acknowledged that the Nordic hamstring exercise (NHE) may prevent injuries to the hamstring, potentially decreasing 51% of all hamstring injuries for athletes competing at different levels and across multiple sports.4 Van Dyk et al4 support the use of the NHE in the prevention of hamstring injury programs, however, NHE may only reduce the number of hamstring injuries when executed accurately. Several authors have reported that a potential disadvantage of the NHE is that it is difficult to perform this exercise using the optimal form required for achieving the complete benefit.5–7 Athletes who are not strong enough to descend to a fully extended knee position may not be able to take the full advantage of this exercise. Therefore, the conventional NHE may not be optimal for preventing strain to the hamstrings in athletes of all levels.
Researchers have modified the NHE to eliminate its drawbacks.8–11 The results of a previous study showed that adjusting the slope of the lower leg support at 20° and 40° allowed the participants to perform the movement through greater amplitude in a controlled manner; peak joint torques being attained at longer hamstring lengths.8 Additionally, the peak joint torque occurred closer to full knee extension compared to the standard NHE.8 The movement close to full knee extension during NHE is similar to the movement occurring in hamstring injuries in the final part of the swing phase during sprinting.12 Since changes in the adjustable incline board or variations in the exercise angle can affect exercise performance and specific muscle activation,9 there is significant interest in examining muscle activation during the variations of the NHE.
There is controversy regarding whether the contractions during the final phase of the NHE are isometric or eccentric type of contractions. Although it was believed that the NHE produces an eccentric muscle action in all ranges of motion, one study13 demonstrated that some athletes lower to the extent where they briefly perform pause in the drop-down position. This movement may result in a change from an eccentric contraction to an isometric contraction.13 It is possible that the hamstrings act predominantly isometrically in the swing phase of kicking, thus incorporating isometric exercises may be more appropriate (than eccentric exercises) because the former strengthens the hamstrings in a specific manner. In addition, the application of the adjustable incline board allows both biceps femoris long head (BFlh) and semitendinosus (ST) muscles to be recruited during the NHE at shallow knee flexion angles, whereas the ST muscle works more during the conventional NHE than the BFlh.11
Performing NHE at the point closest to full knee extension is similar to the movement when hamstring injuries occur in the final part of the swing phase during sprinting.12 Investigating the relationship between muscle length and electromyographic activity of the muscles may be important for preventing hamstring strain injury. However, examining the effect of changes in muscle length during electromyography (EMG), which alters joint angles during motion leading to the moment arm (MA) changing continually, may be a confounding problem. To overcome this obstacle, it is necessary to compare the differences in hamstring length variations with the same MA at the knee, which is the dominant joint of the NHE. The moment arm of a force being defined as the minimum distance between its line of action and the axis of rotation.14
Therefore, the purpose of this study was to investigate the influence of changing muscle length on hamstring electromyographic activity during isometric NHE, while maintaining an equal moment arm. Moreover, isometric training exercise is widely used in the rehabilitation and physical preparation of athletes because of its safety and convenience. Hence, the secondary purpose of this study was to examine the effect of muscle length on isometric contraction during the NHE.
Methods
Subjects
Sample size was determined using G*Power 3.1.9.2 software (Heinrich Heine University, Dusseldorf, Dusseldorf, Germany) and 16 male volunteers were recruited to participate in this study. One participant had experienced a previous hamstring strain injury more than two years prior, while none of the others had any relevant past history of hamstring strain injury. The NHE was not included in the participants regular resistance training program, but were familiar with this exercise. The study protocol was approved by the institutional review board of Waseda University’s ethical committee and all procedures in this study were performed in accordance with the Declaration of Helsinki. All subjects were informed of the purpose and procedure of this study, and informed consent was obtained from all subjects.
Measures
Procedures
Electrodes were placed on the five target muscles, Biceps femoris (BFlh), semitendinosus (ST), Erector spinae (ES), Gluteus maximus (GM), and Rectus abdominis (RA), using wireless EMG sensors (m-BioLog2 DL-5000, S&ME Co., Ltd., Tokyo, Japan) before performing maximal voluntary isometric contraction (MVIC) and the NHE protocol. The electrodes were placed on these muscles based on the following landmarks: midpoint between the ischial tuberosity and the lateral epicondyle of the tibia (BFlh), midpoint of the line between the ischial tuberosity and the medial epicondyle of the tibia (ST), mid-point between the sacral vertebrae and the greater trochanter (GM), two fingers-width distance lateral from the spinous process of the L1 vertebra (ES), and two fingers-width distance lateral from the midline of the umbilicus (RA). Electrodes were placed parallel to the lines between these landmarks, as recommended by the Surface Electromyography for the Non-invasive Assessment of Muscles guidelines (SENIAM).15 To ensure accurate electrode placement on each muscle, the examiner palpated the muscle bellies and used ultrasonography imaging to confirm the location of the muscles.
Prior to electrode placement, the skin overlaying the muscles was shaved and cleaned with alcohol. After electrode placement, the participants were asked to contract the target muscles to test the muscles for accurate EMGs. The volunteers underwent MVICs during a leg curl in the prone position with knee flexion of 30° and 90° for both BFlh and ST. The GM, ES, and RA were measured using hip extension, trunk extension in the prone position, and trunk flexion in the supine position, respectively. These MVICs were used in previous studies that investigated the EMG activity of the hamstring muscles.16,17 Each MVIC protocol was for a period of five seconds and was performed twice with the mean value used for data analysis.
The EMG electrodes were pre-amplified (10×) and linked through the EMG mainframe, which further amplified it (100×) to a total gain of 1,000 × and was band-pass filtered (20-500 Hz). The root mean square (RMS) was redacted from the raw EMG data (the middle section; middle two seconds of the five second exercise) for further analysis. The maximum EMG values during MVIC of each muscle were used to normalize the EMG values during the NHE protocol.
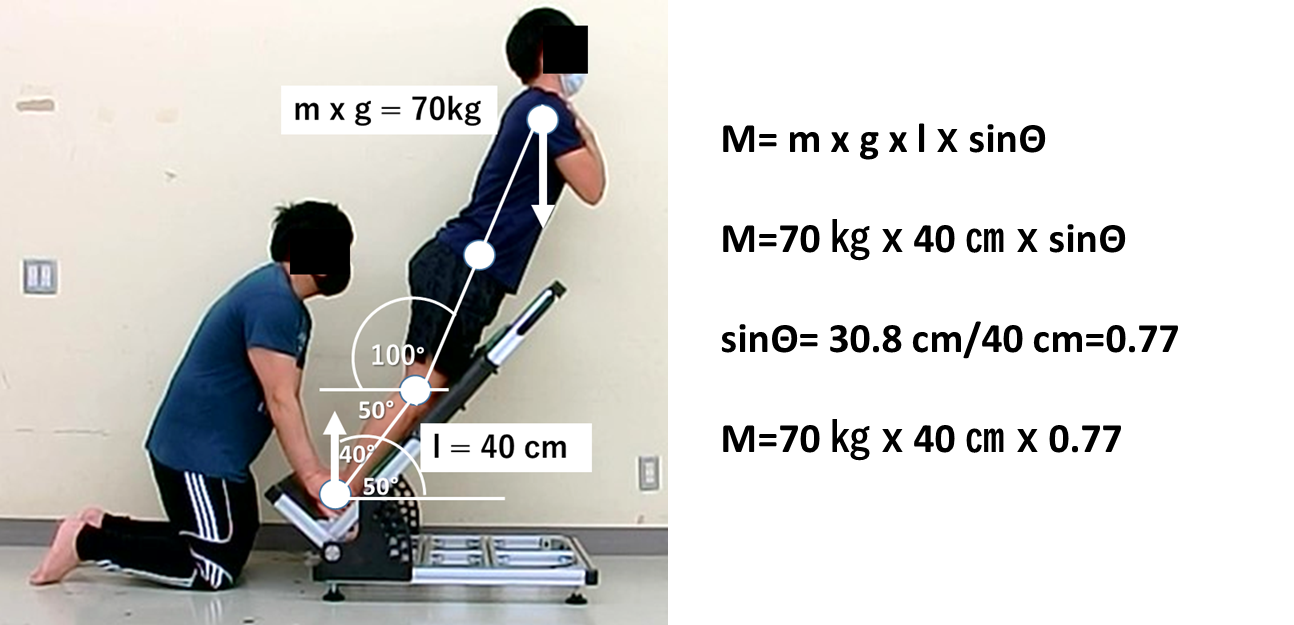
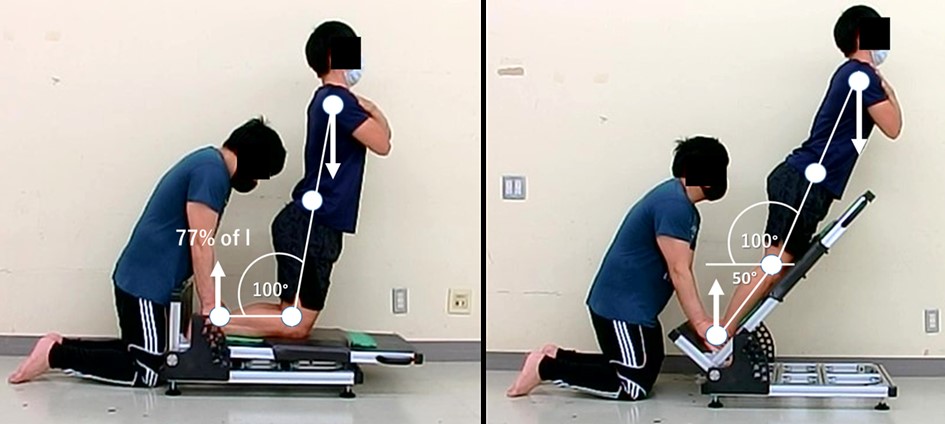
After the MVIC protocol, the participants were prepared for the exercise protocol. A marker was placed on each individual’s hip, knee, and ankle joint to measure the length of the lower leg from the knee to the ankle joint. To compare the effect of changing muscle length at an equal moment arm at the knee between NHE and NHEB, the examiner calculated and marked the point at 77% and 94% of the length of the lower leg. An example of these calculations is shown in Figures 1-3. The participants were randomized to perform the experiment protocol consisting of four variations of the NHE as follows: 1) NHE during isometric contraction at 100° of knee extension and the examiner providing stabilization at the mark point at 77% of lower leg length (NHE-77%), 2) NHE during isometric contraction at 100° of knee extension and the examiner providing stabilization at the mark point at94% of lower leg length (NHE-94%), 3) NHE on the adjustable incline board plane at 20° during isometric contraction at 120° of knee extension (NHEB-77%), 4) NHE on the adjustable incline board plane at 50° during isometric contraction at 150° of knee extension (NHEB-94%). The participants were asked to hold the isometric contraction for five seconds and performed two repetitions of each MVIC test (total of eight repetitions). A manual goniometer was used to monitor the knee joint angle during the NHE protocol. If a participant could not hold the targeted degree angle, the trial was discarded, and the participant was instructed to re-perform the trials.

_between_the_conventional_isometr.png)
_between_the_conventional_isometr.jpeg)
Statistical Methods
The average value (+SD) for each variation of NHE was calculated. The RMS data were normalized as a percentage of the maximum isometric values (normalized EMG [nEMG]). Two-way mixed repeated-measures analysis of variance (ANOVA) was used to compare between within-factor (Type of NHE; (NHE and NHE on incline board) and moment arm at knee (77% and 94%). In between factors (muscles; (between BFlh and ST)) were compared. The difference in nEMG between GM, ES, and RA were analyzed using the same procedure. Tukey’s post-hoc test was applied for the identification of any significant findings. All statistics were analyzed using SPSS for Windows (version 25.0; IBM Corp., Armonk, NY, USA) and statistical significance was accepted at the p < 0.05 level.
Results
A total of 16 male volunteers (age 24.25 ± 2.04 y, height 170.58 ± 5.46 m, weight 70.01 ± 10.12 kg, mean ± SD) were recruited to participate in this study.
Hamstring muscles (BFlh and ST)
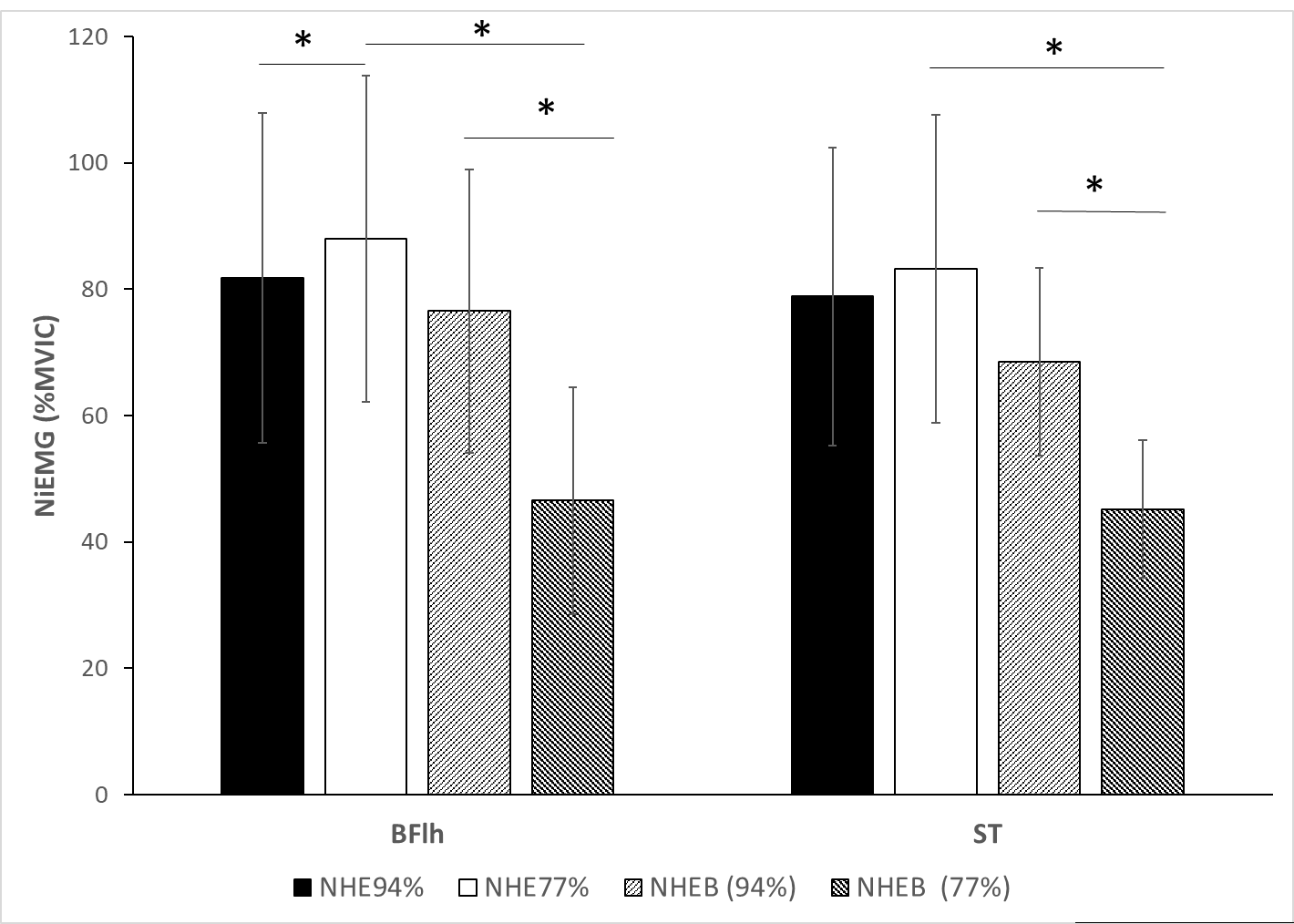
Differences in the nEMG between the four NHE variations and moment arm at the knee in BFlh and ST are shown in (Figure 4). The BFlh nEMG activity values for NHE-77% were significantly higher than those for NHE-94% (p=0.036) and NHEB-77% (p<0.001), while in ST a significantly higher nEMG was only found in NHEB-77% (p<0.001). Moreover, NHEB-94% was significantly greater than NHEB-77% for both BFlh (p<0.001) and ST (p<0.001.
_between_nhe_variation_and_moment_arm_at_the_knee.png)
Related muscles (GM, ES and RA)
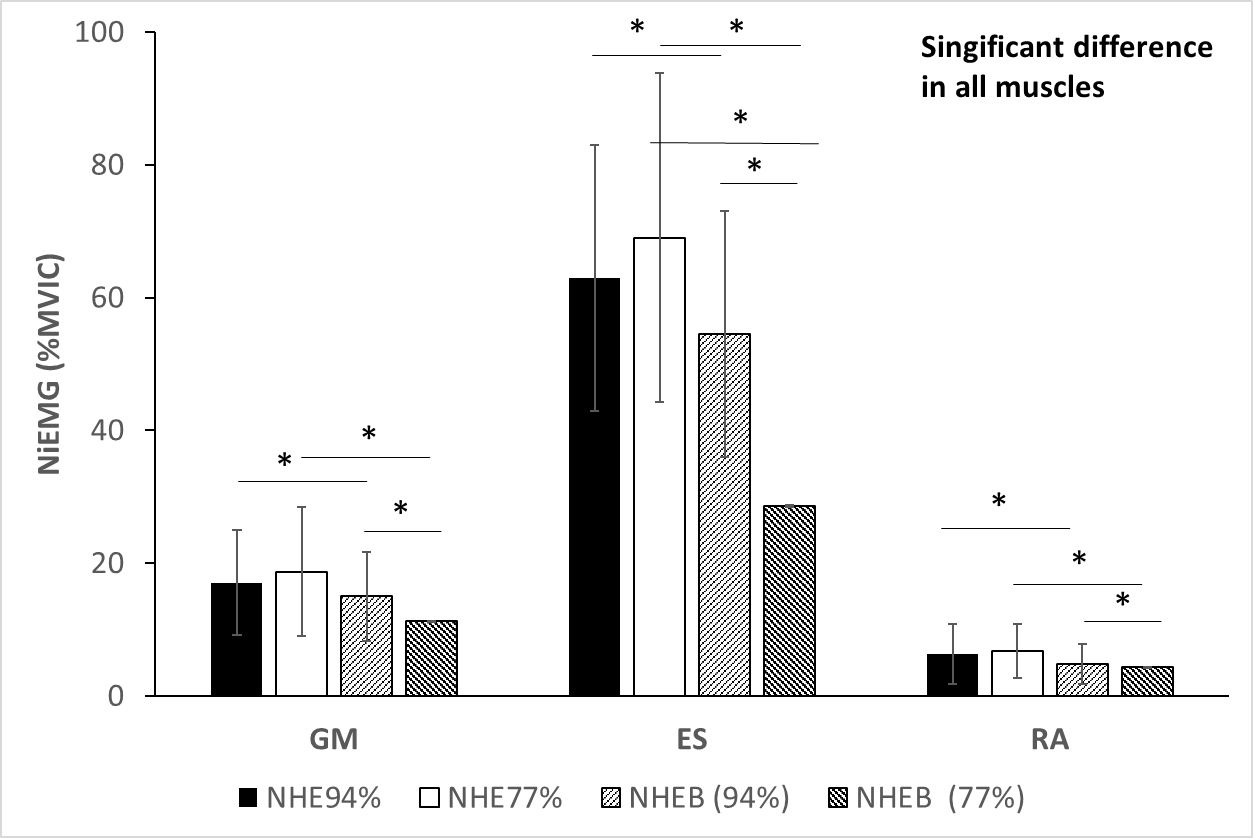
Differences in the NiEMG (%MVIC) between the four NHE variations and moment at in GM, ES, and RA are shown in Figure 5. In GM, ES, and RA, NHE-94% was significantly greater than NHEB-94% and NHE-77% was significantly higher than NHEB-77% (p<0.05). Moreover, NHEB-94% was significantly greater than to NHEB-77% (p<0.05).
_between_nhe_variation_and_moment_at_knee.png)
Discussion
This study aimed to examine the influence of muscle length on the hamstring and related electromyographic activity by modifying the knee angle during isometric NHE.
First, the present study found that the BFlh EMG activity level was not statistically different from ST between NHE-77% of moment arm at 100° of knee extension and NHE on the adjustable incline board plane at 20° at 120° of knee extension (NHEB-77%). And, NHE-94% of moment arm at 100° of knee extension and NHE on the adjustable incline board plane at 50° at 150° of knee extension (NHEB-94%) during isometric contraction. This current study confirmed the results reported by Ditroilo et al.6 as the BFlh activity during NHE at 100° of knee extension was very high (NHE77%; nEMG 87.93%MVIC, NHE94%; nEMG 81.85%MVIC). However, this finding contradicts the results of a previous study in which ST was activated to a greater extent during NHE.11,18–20 High BFlh and ST activity have been recorded during the conventional performance of the NHE.7 This discrepancy in findings may be due to variations in the normalization procedure of the hamstring EMG (e.g., maximal isometric voluntary contraction) to examine hamstring activation.21
Second, BFlh and ST were recruited to a greater extent during NHE-77% compared with NHEB-77% at the same moment arm at the knee. However, the results of the current study did not find a significant difference during the NHE-94%. The results indicate that performing the NHE on the adjustable incline board plane allowed participants to perform NHE at a greater knee extension angle and stimulate muscle activation at higher extent. Soga et al. reported that increasing the lower leg slope angle (0°–40°) shifted the break point angle ( the knee flexion angle at which subjects are no longer able to maintain the required tempo (10°/s) for descent) to the lower knee flexion angle.22 Furthermore, Hirose et al. demonstrated that BFlh and ST muscles did not statistically different in their activation during NHE at shallow knee flexion angles with the incline board plane, whereas the ST muscle was activated to a greater extent during conventional NHE than the BFlh muscle.11 A previous study showed that when the moment arm of the knee joint was set to be equivalent, the EMG activity of BFlh decreased while this muscle was lengthened during isometric knee flexion contraction.23 This previous study23 explained that when a muscle is lengthened, the passive muscle component produces the force during when hamstring muscle is in this stretched position, leading to fewer motor units being needed to work resulting in decreased EMG activity. Moreover, several authors have demonstrated an inverse relationship between hamstring EMG activity and hamstring length during the NHE, regardless of the intensity during isometric knee flexion and eccentric contraction.8,24,25 A recent study reported that muscle activity levels in the proximal and middle BFlh regions were higher at 30° and 60° of knee flexion rather than at 90° during maximal voluntary contraction of knee flexion.26 However, no differences in peak EMG activity during maximal voluntary knee flexion between various hamstring lengths was achieved by altering hip angles.27,28 This discrepancy in findings may be related to differences in joint dominance. Chleboun et al., indicated that the moment arm of the hamstrings is greater at the hip joint than at the knee joint29 affecting hamstring activity. In this study, the hamstring selectively demonstrated greater activity in the shorter muscle length (100° of knee extension during isometric NHE).
The current study found that BFlh and ST were preferably activated in both 77% and 94% at the knee during the NHE as compared to the NHEB. The results are consistent with those of Sarabon et al., who reported that the peak hamstring activity decreased while the peak knee and hip torques remained similar during modified NHE variations, with increased lower leg support slope than is seen in the standard NHE.8 Sarabon et al. explained that the non-contractile elements contributed to a larger proportion of the force, owing to the longer length of the hamstrings compared with the standard NHE.8 However, the present study observed that during NHE, BFlh and ST were recruited at higher level during performing 77% than 94%. A possible explanation is that during 77% of the moment at the knee, the examiner held the lower leg at a point around the gastrocnemius muscle, leading to a compression force. Compression-induced reductions in muscle displacement also correspond to a reduction in muscle activation.30 Thus, implying that hamstring muscles work harder to compensate for the decrease in gastrocnemius activity.
Among the additional muscles that were studied, the ES was recruited at a high level of nEMG (%MVIC) during the NHE. A previous study showing that when the degree of knee extension angle increased, EMG activity of ES was greater than Gmax and rectus abdominis.20 This is because when the distance of ES is decreased from ground level, ES has to work to maintain the trunk in an erect position against gravitational force provides more hip extension torque than Gmax.20 Moreover, ES and GM were recruited to a greater extent in NHE-77% than in NHEB-77%. This result is consistent with that of Sarabon et al., who found that increasing the angle of slope was associated with decrease in ES and GM muscle activity.8
This study had several limitations. First, the position of holding the leg was recorded with respect to the calculated moment arm, for comparing the same moment arm between conditions. However, the actual difference in lengths of holding positions between NHE of 77% and 94% were small. Future studies need to identify an effective way to compare the influence of different hamstring lengths at the same moment at the knee.
Conclusion
The results of this study indicate that isometric hamstring EMG activity decreased when the hamstring muscles were lengthened during NHE. The passive muscle component produces a force when the hamstring muscle is in a stretched position, and thus fewer motor units are required to work. According to the current results, NHE-77% may be better in terms of recruiting hamstring activity compared to NHEB-77% when the moment at the knee was equivalent.
Conflicts of interest
The authors declare no conflicts of interest.
Acknowledgements
The authors would like to acknowledge the facilities and the assistance of Graduate School of Sport Science, Waseda University.