INTRODUCTION
Soccer is a sport that requires high-intensity sprinting, kicking, and rapid changes in direction at high speed,1–4 which can be important causes of injury.5 It has been reported that in soccer, the most common injuries are to muscle, particularly the hamstrings and adductor longus.6
Injury surveys of soccer players show that groin pain is relatively common and accounts for 11% of all injuries.7 In addition, 55% of male soccer players are reported to have experienced groin pain in the past.8 Groin pain in soccer players is typically caused by kicking or running,9 and is associated with adductor muscle weakness.10 Furthermore, most groin pain in soccer players has been reported to be minor to moderate with no time loss related to training or games.11
With respect to groin pain, the Doha agreement classifies pain into adductor-related, iliopsoas-related, inguinal-related, pubic-related, and hip joint-related pain.12 Adductor-related pain is considered to be the most common category accounting for 61% of all groin pain,13 and the most frequent cause in soccer players.14
The incidence of groin pain can be reduced by up to 41% through groin pain prevention programs such as the Copenhagen adduction exercise (CAE) in semi-professional soccer players.15 Despite this, there is a lack of information on the effects of injury prevention programs in younger soccer players. Functionally, the hamstring muscles have an auxiliary effect on the hip adductor muscles.16,17 Both muscle groups have been shown to demonstrate high activity during kicking, jumping, and cutting movements that occur specifically in soccer.18 Despite this, it is unclear whether training the hamstring muscles enhances the effect of the CAE in groin pain injury prevention.
Therefore, the purpose of this study was to evaluate the preventative effects of exercise on groin pain in high school soccer players in three groups comprising NHE alone, combined NHE and CAE, and a control group.
METHODS
Study design and participants
Participants were male high school students participating in a Japanese under 18 soccer leagues. Participants were competing at the highest level in the prefecture and national league, and the top teams were targeted. We contacted 10 schools with teams in this league for potential inclusion. Consent was obtained from the principal and coach from each school. Following such approval all parents and players were required to provide written informed consent. All rights of the participants were protected. This study followed the Declaration of Helsinki and was approved by the University Ethics Committee at the Saitama Medical University, Saitama, Japan (M-98).
Randomization
This cluster randomized controlled trial was registered with the University Hospital Medical Information Network at The University of Tokyo Hospital (Registration number 000036863) and was conducted from August 2019 to December 2019. The authors determined it would be difficult to blind subjects through individual subject randomization, so each high school team formed a cluster group which were then randomized using the envelope method. After a team agreed to participate, the principal investigator opened a sealed envelope revealing their group assignment. Group A received the CAE alone, group B received the CAE and NHE, and group C received no interventions other than continuing their normal practice. The group randomization procedure used is not considered optimum in randomized clinical trials. However, this procedure is widely used and accepted in sports injury prevention trials as a way to limit contamination between intervention and control groups.15 In addition, each school insisted that any intervention must be offered to team members as a group rather than as individuals. Two high schools that did not respond, one high school that could not start at the right time, and four others absent from club activities for some reason were excluded.
Blinding
It was not possible to blind players, coaches or the principal investigator to group allocation. Recorded data with encrypted numbers were collected by the principal investigator alone. However, the research assistant was not informed of the randomization, and outcome measures were not available to any party until all data had been collected.
Intervention
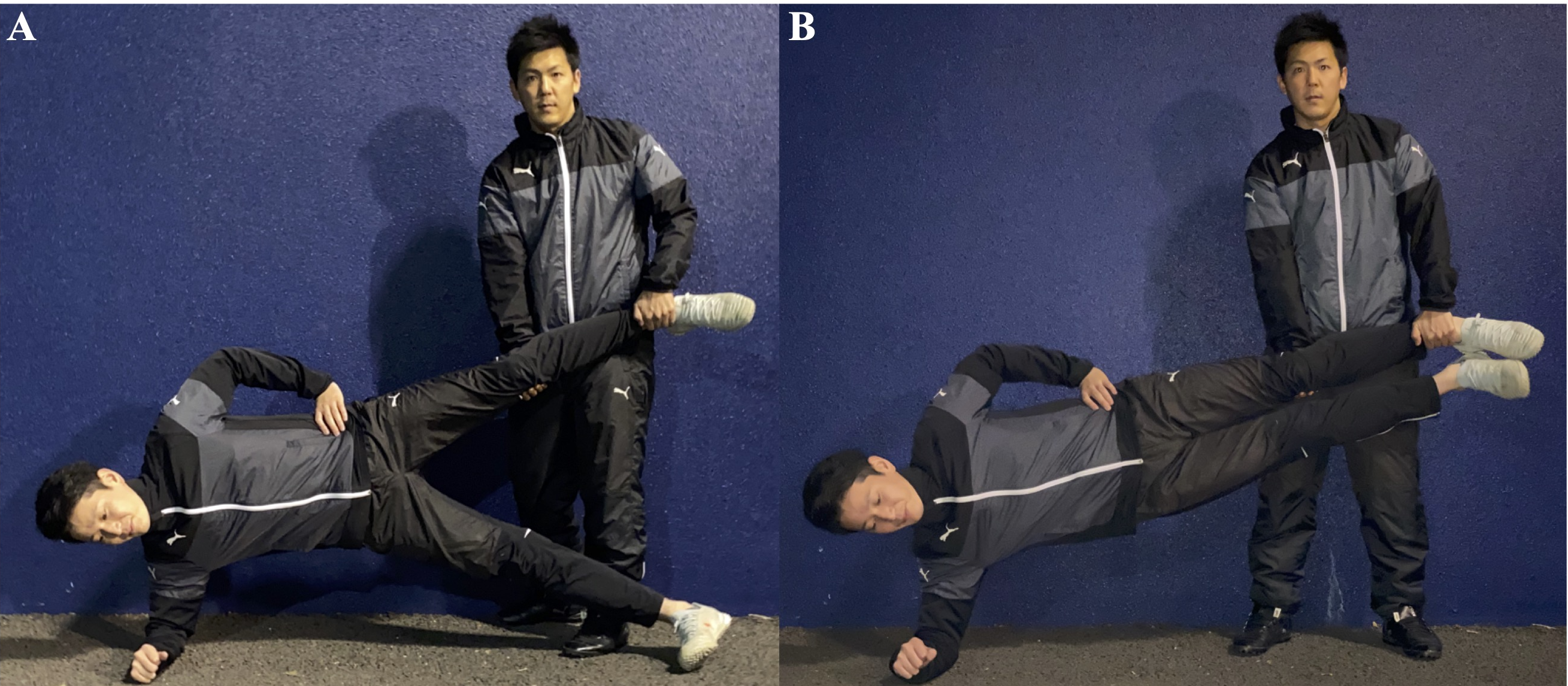
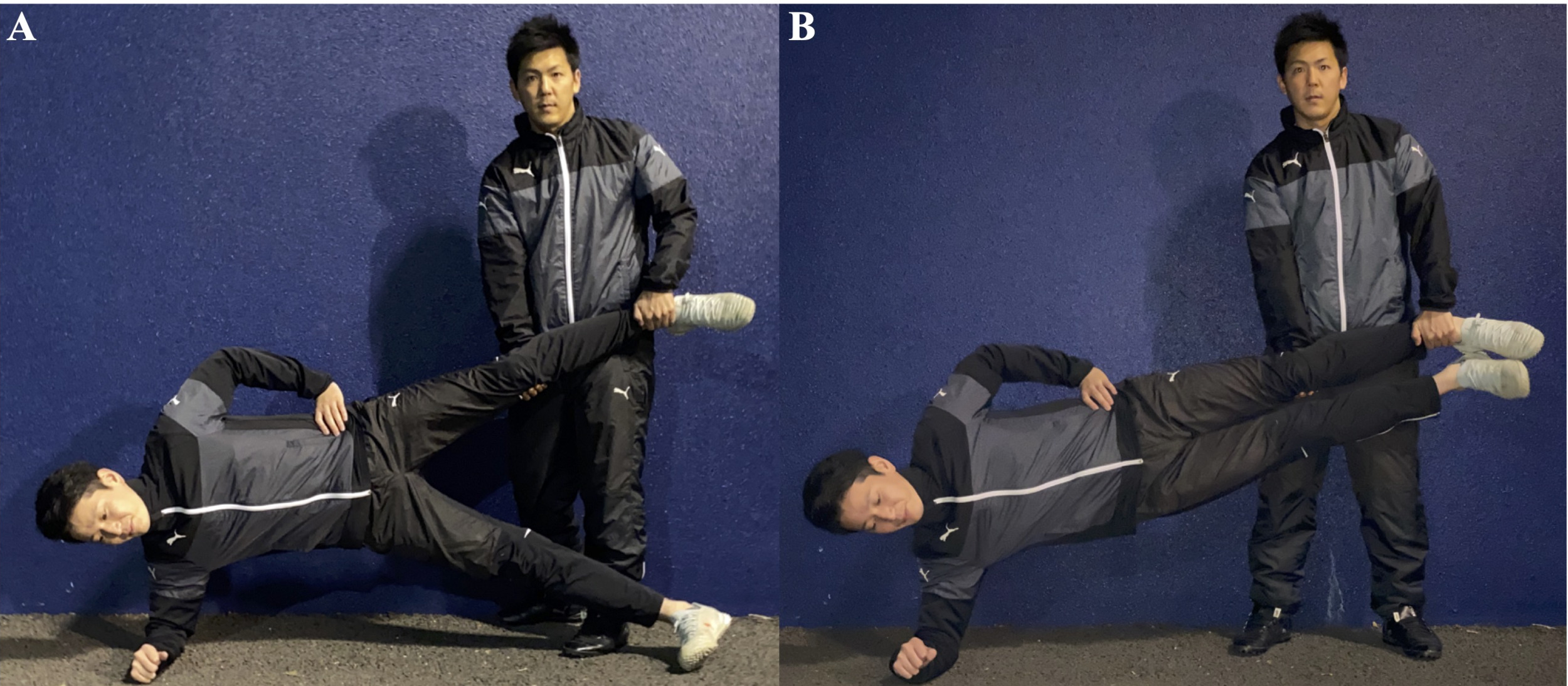
The CAE was performed as follows. The athlete lay on their side, their forearm on the ground to stabilize the trunk, while their other arm was placed with their hand on their pelvis. A team mate supported the player’s uppermost leg at the ankle and knee. The athlete was then required to lift their body off the ground, by adducting their upper hip, until the upper leg and trunk were horizontal, following which they lifted their lower leg off the ground to touch ankles. This was counted as one repetition, each lasting three seconds. (Figure 1).19 Based on previous studies,20,21 players were instructed to stop if they experienced more than 3/10 pain while performing the exercise. For the CAE, players were asked to carry out the exercise program 1-3 times a week for 16 weeks as part of their regular warm-up.
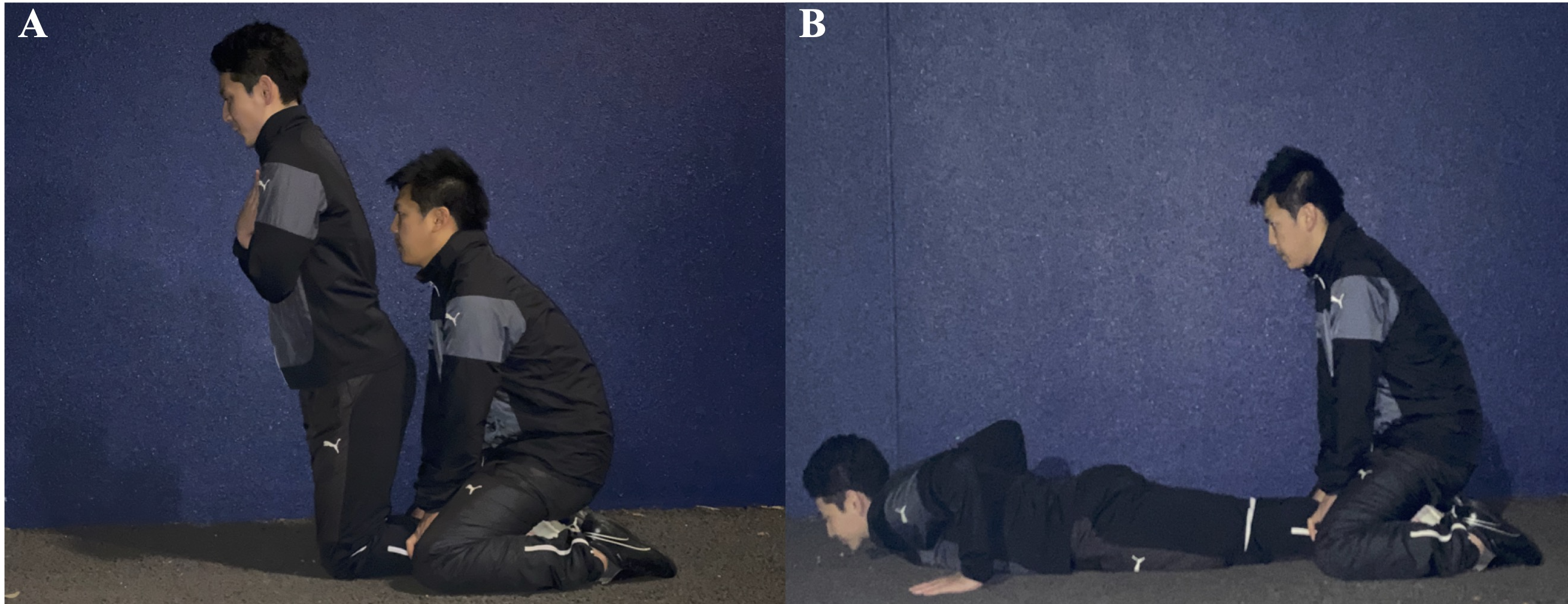
For the NHE, the player started in a high kneeling position with their lower legs stabilized by an assistant. The player then slowly lowered their body until parallel with the ground. The exercise was completed once their hands touched the ground (Figure 2).22 Again, if pain of greater than 3/10 was provoked during the exercise the player was told to stop. For the NHE, players were asked to carry out the exercise program 1-3 times a week for 16 weeks as part of their regular warm-up.

The number of repetitions was based on previously reported effective injury prevention programs (Table 1).15,22 The principal investigator explained the exercises to the coach, athletic trainer, and athletes before commencement of the study. During the intervention, the researchers visited each team once a week to observe the exercises and give advice if necessary. Subjects were informed that the exercise had to be conducted under the supervision of a coach or athletic trainer, and that the principal investigator was to be contacted if problems or adverse events occurred during the exercise program.
Compliance
Exercise compliance was recorded daily by athletes on a recording sheet. To calculate overall compliance, the total number of completed sessions was summed and divided by the number of respondents. Once a week, we contacted managers, athletic trainers, and athlete representatives to keep track of exercise progress. The principal investigator collected recording papers with encrypted numbers.
Outcome measures
The intervention period was 16 weeks. Data collection sheets were distributed to athletes and completed by individuals to record their exercise compliance and injuries. Any presentation or development of groin pain was conveyed to the athletic trainer or physiotherapist. The details of the injury were self-reported, but when the athlete was uncertain about what to report, he was advised by an athletic trainer or physiotherapist, who was informed of the details by the chief investigator. Reports were collected weekly by the principal investigator. The definition of groin pain in this study was a condition in which pain occurs in the groin during sports activities, regardless of time loss or need for treatment, with reference to previous studies.23,24
The principal investigator explained the Doha classification method to the trainers and physiotherapists of each team and let them determine the type of groin pain for each athlete in pain. The number of injuries and the injury rate indicates the frequency and probability of groin pain. The analysis was performed using an intention-to-treat (ITT) analysis.
Exposure
To calculate the exposure time individually, the athletes were asked to record daily practice time, match time, and time lost due to injury, and the total for each group was summed for each category. Once a week, managers, athletic trainers, and athlete representatives were contacted, and worked closely with the researchers to review the status of the recording and injury report forms. The principal investigator entered and matched the data from record sheet with personal information.
Sample size
The sample size calculation was based on the average prevalence of all groin problems among male football players (29%).25 On the basis of these data, a groin pain rate for this study of 29% in the group C, 17% in the intervention group A, and 12% in the intervention group B was projected. Using these rates, the sample size to determine statistically significant differences by using cluster randomization as well as a 2-tailed test with α = .05 and 1-β = .80 was calculated. The estimated sample size for this study thus obtained was 189 (63 patients per group).
Statistical analyses
χ2 test was performed to compare the number of injuries to groin pain among the three groups A, B, and C. Following that, Bonferroni correction was performed as a post-hoc analysis for the items for which a significant difference was found. The injury rate per 1000 hours was calculated from the number of injuries. Relative risk (RR) was calculated to show the risks of developing groin pain for groups A and B relative to group C. Injury severity was determined by counting the calendar days lost because of the groin pain. Groin pain was classified as minor (1-7 days lost), moderate (8-21 days lost), or severe (more than 21 days lost), with reference to previous studies.23,24 The effect size for the effect size of the number of injuries was calculated as φ. Effect size <0.1 is rated as small, 0.3 rated medium, and >0.5 rated large.26 IBM SPSS Statistics for Windows, Version 26.0 (Armonk, NY: IBM Corp Released 2018) was used for statistical analysis.
RESULTS
Participants
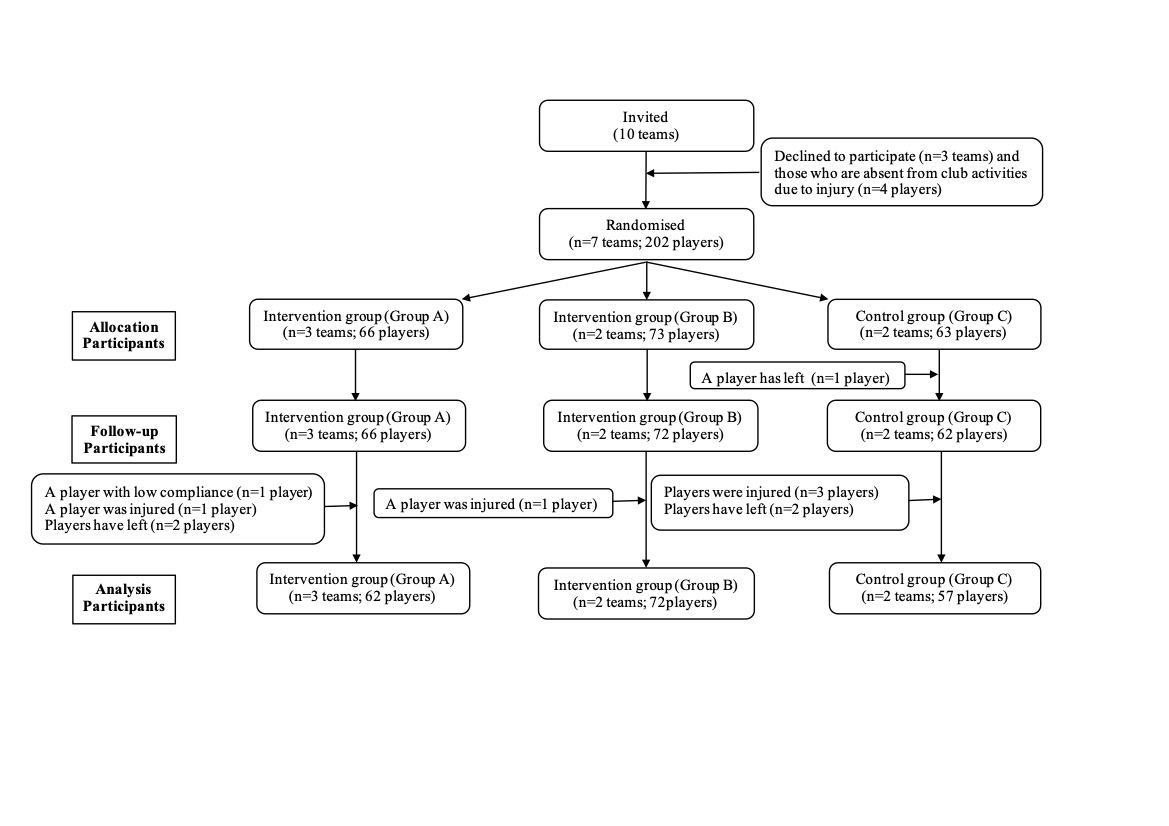
A total of seven high school soccer clubs (202 players) were enrolled in the study. The flow of the players through the phases of the study is shown in Figure 3. There was a total of 11 dropouts, four in Group A, one in Group B, and six in Group C. The reasons were retirement, injury, and low compliance. Baseline characteristics for players included in the ITT analysis are shown in Table 2.

Number of injuries
Table 3 shows the number of cases with groin pain. The frequency of groin pain during the intervention period was significantly lower in group B than in group C. The number of players with groin pain who lost time due to injury was significantly less in groups A and B than in group C.
When comparing groups, A and B, a small effect size was observed in groin pain, although there was no significant difference.
The injury rate of groin pain and relative risk with time lost to sport
Table 4 shows the groin pain injury rate and the injury rate with time lost RR. The incidence of groin pain per 1000 hours was lower in groups A and B than in group C. Furthermore, RR of groin pain was significantly lower in groups A and B than that in group C according to the 95% confidence intervals. The injury rate for groin pain with time lost per 1000 hours was lower in groups A and B than in group C. Furthermore, RRs of groin pain and groin pain with time lost per 1000 hours were significantly lower in groups A and B than that in group C according to the 95% confidence intervals.
Severity of groin pain
Table 5 shows the severity of reported groin pain (mild, moderate, or severe). The average number of days lost was 5.5 ± 5.2 days in group A, 10.3 ± 6.4 days in group B, and 14.4 ± 8.3 days in group C. The rate of minor groin pain in the intervention groups was higher than in the control group (66% in group A vs 33% in group B vs 25% in group C), whereas the rate of moderate groin pain was lower in the intervention group than in the control group (33% in group A vs 66% in group B vs 68% in group C).
Fisher’s exact test was used to determine if there was a significant difference in the distribution of injury severity between both groups (group A and B vs group C). However, due to the low number of players with groin pain in the moderate and severe categories, these categories were combined into one category. No difference was detected in the severity of groin pain between groups (p = 0.21).
Compliance with the exercise program
The CAE compliance rate was 97% in group A and 95% in group B. The NHE compliance rate was 98% in group B.
DISCUSSION
The CAE has been reported to reduce the incidence of groin pain,15 which is consistent with the findings of the current study. In this study, the combined intervention of CAE and NHE reduced the number of injuries, and CAE alone reduced the number of cases with time lost to sport as shown in Tables 3 and 4. This supports the effectiveness of CAE in preventing groin pain in high school soccer players. The results also indicate that CAE and NHE were effective in preventing severe groin pain. From these results, it is likely that the NHE enhances the effect of the CAE. One explanation for this is that the adductor muscle and the hamstrings also assist in hip adductor, and conversely, adductor muscles also assist in hip extension,16,17 so it is possible that NHE enhanced the effect of CAE through this mechanism. Another explanation is combining exercises together likely had an enhanced strengthening effect on the adductor and hamstring muscle groups which reduced the occurrence and severity of injury. From the above, the combination of CAE and NHE exercises may be more effective in preventing groin pain than CAE alone.
In a report of factors related to the occurrence of groin pain and reduction in physical function in professional soccer players, it was reported that isometric strength of the adductor muscle is an important factor.10 The CAE has been shown to improve both eccentric adductor and eccentric abductor muscle strength.17 In addition, it has been reported that muscle damage in the thigh is reduced by the stability of the trunk,27,28 and it is possible that a combination of CAE and NHE programs may increase resistance to injury by increasing the extensibility and stability of soft tissues, including muscles, on the anterior, posterior, medial, and lateral sides of the hip joint and trunk. Since this study did not measure trunk stability or motor control, additional studies from such a viewpoint should be conducted in the future.
Kicking is important in soccer, and during this movement, the adductor muscles show maximum tension from the position of hip extension to flexion in the swing phase.29 In addition, the hamstring muscle are highly active during maximal hip and knee extension and flexion,30 suggesting a potential for injury. From this, it is predicted that the adductor and hamstrings muscles are likely to work strongly together at the same time, and that the hamstrings act cooperatively with the adductor muscle in the hip flexion phase. Strengthening both groups of muscles may enable greater protection during kicking activities which may be effective to prevent pain.
One of the goals of this study was to determine whether a muscle strengthening exercise program utilizing the CAE alone or a combined intervention including the CAE and NHE would reduce the severity of groin pain. The effect of the CAE intervention on groin pain severity has not been previously reported. Previous studies were used to assess severity.31 The results of this study found that CAE and NHE did not affect the severity of groin pain. Specifically, it did not reduce the average number of days lost and did not affect the intensity of groin pain development, which was classified as mild, moderate, or severe. Interestingly, the rate of minor groin pain was greater in the intervention groups vs the control group yet the overall injury rate was lower in the intervention group vs the control. One interpretation of this discrepancy is that CAE reduces the severity of groin pain, so that there are more minor injuries. A similar finding has been reported for the NHE in reducing the severity of hamstring injuries.32 The number of cases categorized according to higher severity of injury is small in the current study, hence further study is required to determine the effect of CAE on injury severity.
Comparing intervention groups, A and B, the number of groin pain injuries was lower in group B. Furthermore, the injury rate was lower in group B than in group A, but there was no significant difference in RR. Both groups A and B had a significantly reduced risk of injury compared to group C. This suggests that both forms of exercise may be effective in reducing the incidence of injury, although the CAE alone appears to influence the risk of injury.
Limitations
This research was conducted using a cluster randomized controlled trial. Even with the mixed-effects statistical analysis that attempts to account for this clustering, this design can result in high Type I error rates. Also, the results may include Type II errors due to the limited sample size. Since the research was targeted only at top-team high school soccer players, it may have led to a selection bias. Also, all injuries were self-reported, which can lead to measurement bias, and results may vary if all injuries were diagnosed by a healthcare professional. Interventions for inguinal pain prevention exercises were limited to 16 weeks, so it is essential to examine the effects of these exercises over a longer period. In addition, a larger and more diverse sample would help to better understand the impact of CAE and NHE on injury rate and loss time.
CONCLUSION
A 16-week program incorporating the CAE in training sessions in high school soccer players reduced the incidence of groin pain and severity of injury according to time-lost to soccer, however the combination of both the CAE and NHE may be more effective than the CAE alone.
Conflicts of interest
The authors report no conflicts of interest.
Acknowledgements
The authors thank all players and coaches who participated in the study, as well as the team medical staff.