
Introduction
Participation in overhead athletics occurs across a wide variety of age groups. Many sports, such as baseball, have become part of numerous youth communities. Previous reports have estimated that 4.8 million children between the ages of four through fifteen participate in some form of recreational baseball.1 This competitive atmosphere continues into higher levels of play, with 11.5 million athletes participating in high school or club baseball.2 Due to the repetitive demands of overhead throwing, injuries occur from participation in baseball. Between the years 1994 to 2006, it is believed that approximately 1,596,000 children under the age of eighteen were treated for baseball-related injuries in emergency departments in the United States.2 Specifically related to throwing, approximately 30% to 70% of youth throwers report having experienced throwing arm pain.3,4 More than 60% of these injuries can be found in the shoulder or elbow throughout a pitcher’s career.5,6 Contributing factors that have increased the risk of injury development for the young baseball athlete include several possibilities for over exposure to throwing. These comprise pitch counts, yearly participation, early sport specialization, playing on multiple teams, and altered throwing biomechanics.7–10
Due to the high occurrence of injury in the young baseball population, it is imperative to provide injury assessment to manage athletes for participation screening, and to measure response to treatment in rehabilitation settings. Patient-reported outcome (PRO) measures are often used to provide a reported assessment from the athlete on how they are performing specific tasks. This assessment quantifies response through item scoring, which in turn gives a finalized number that can guide clinical decision-making if the athlete is experiencing symptoms. These scales aid with providing assessment regarding the physical, psychological, and social domains and their influence on patient beliefs, experiences, and perceptions.11 Many region-specific PRO measures have been developed and validated through past literature. Concerning the upper extremity, many of these measures focus on the arm with lack of specificity for the shoulder and/or the elbow, and have been studied in a wide range of populations.12,13 Many of these scales are utilized for a general population, and were not created to address the high physical demands of throwing.14 For this reason, some researchers have attempted utilizing a combination of PRO measures, however this poses a dilemma to the patient with completing multiple scales, which can be a daunting process.6 Additionally, those PRO scales that focus on the upper extremity and are created for the general populace, have ceiling effects, lack specificity for asking baseball-related questions, or do not differentiate between body regions.6,15–17
More recent research has suggested the use of visual analog scales (VAS) to capture specific questions that address the physical demands of overhead athletes.5 The Kerlan-Jobe Orthopaedic Clinic Shoulder & Elbow Score (KJOC) includes 10 questions specific to the overhead athlete, each scored on a 10-point VAS, which can aid with determining if someone is throwing with or without pain.5 When all questions are added together the highest possible score is 100 points, with a higher score equating to a better outcome of throwing without symptoms. Items in the KJOC scale include questions on areas like presence of pain, weakness, fatigue, instability, or difficulty initiating activity; as well as impact of pain on throwing motion, velocity, power, endurance, control, and competition level. The scale also asks about effect of symptoms on sports relationships with others.5 However, this tool was created for the adult baseball athlete and was not originally validated for younger demographics. In its original validation, the KJOC was found to be more sensitive to detecting performance changes while participating in amateur and professional sports.5 The KJOC has now been studied in the adult throwing athlete and younger female softball players, and researchers have established a single score to separate groups between those that are throwing with pain to those that are throwing without pain.5,18,19 A “cut-score” has not yet been established for the male youth and high-school aged baseball athlete. Therefore, the purpose of this study was to determine if the scores on the KJOC are different between those throwing with and without pain in male youth and high school-aged baseball athletes. Additionally, this study aimed to establish a prediction score for whether a young baseball athlete is throwing with symptoms. The hypothesis was that the scores on the KJOC would be statistically different between groups in the young baseball athlete, and that there would be a predictive score that could determine if a younger athlete is throwing with or without symptoms.
Methods
Study Design
This was a quasi-experimental study of youth and high school-aged male baseball athletes. There were two groups of participants. The first group was allocated through retrospective design and had been in physical therapy previously due to complaints of pain with throwing during participation in baseball; data for this group was collected as part of usual clinical care procedures. The subjects recruited in the retrospective group had already completed the KJOC during the initial physical therapy evaluation prior to initiation of physical therapy treatment. The second group were prospective subjects who were currently participating in baseball and had no symptoms with throwing. All subjects filled out the KJOC questionnaire. The KJOC is a one-hundred millimeter VAS consisting of ten questions that postulate athletic performance, symptoms, and interpersonal relationships related to overhead sports. Additional questions were asked such as highest level of baseball participation, throwing arm dominance, positions played, and if the athlete was currently throwing with or without pain or could not participate due to arm pain.
Study Participants
Youth and high-school aged baseball players between the ages of 10 to 18 years were recruited through purposive sampling and were located in the Northeast Ohio area. Inclusion criteria for the retrospective group entailed prior attendance at a local physical therapy clinic and had attended physical therapy due to elbow or shoulder pain in their throwing arm, filled out the KJOC at the onset of care, and were active participants in competitive levels of play for baseball. Concerning the prospective group, subject recruitment focused on baseball athletes in the above age range, participating in competitive levels of play for baseball, and who were throwing with no complaints of pain. Exclusion from the study entailed subjects that did not meet the above criteria regarding age range and/or did not participate in baseball at a competitive league level of play. Institutional Review Board approval was obtained from Nova Southeastern University prior to subject allocation. Written informed consent was gained from all participants with parental consent and utilization of an adolescent assent form for both retrospective and prospective groups. An a priori analysis was run to determine the appropriate sample size to accurately detect differences between groups. A medium to high effect size of 0.7 was utilized based on prior literature.5,19–21 Previous research on different demographics using the KJOC has found statistically significant differences between those throwing with and without arm pain.5,19–21 The statistical analysis chosen for this study included a Mann-Whitney U and logistic regression. Statistical power analysis software, G*Power, was used to ensure satisfactory statistical power.22,23 Additionally, for a logistic regression analysis previous research has recommended 10 to 20 subjects per outcome variable.24–26 For the purpose of this research there are two outcomes, throwing with pain and throwing without pain. Therefore, a sample size of 56 subjects, 28 in each group, was found to provide the intended power, which was set at 0.8, for this study.
Study Procedure
A letter was sent out to all retrospective group participants and their parents outlining the intent of the study, which included the informed consent and assent forms. These forms were then completed in person or sent back to the lead author via mail. A research flyer was created for the prospective group. Local youth, high school, and travel baseball coaches were contacted by the lead investigator to pass this flyer out to all potential participants to contact the lead author. Once contact was established with subjects, each participant with a parent then met with the lead investigator at a local physical therapy outpatient clinic. Once informed consent was obtained, each participant filled out the KJOC, which took approximately 10 minutes to finish. All subjects in both groups were given standardized instructions to fill out the KJOC independently without parental or legal guardian influence.
Statistical Analysis
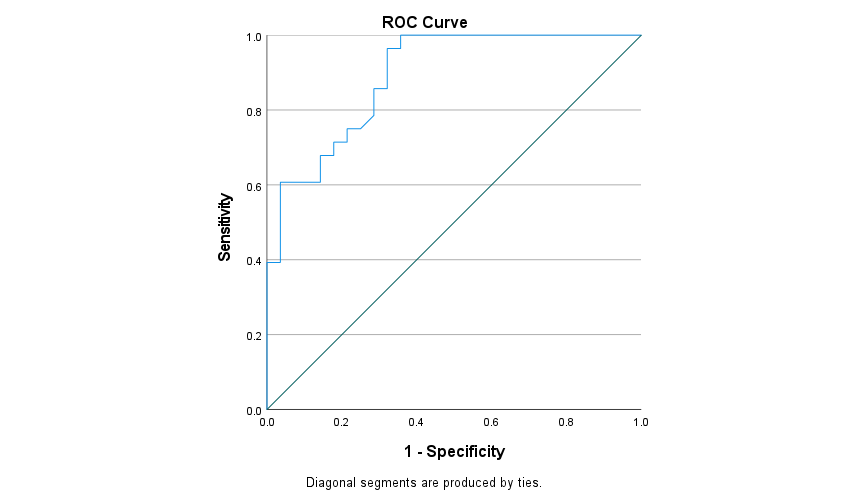
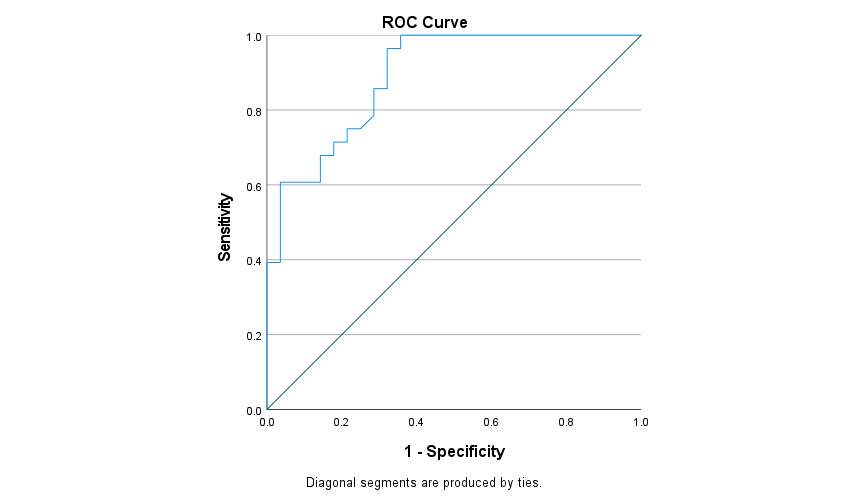
The study analysis was performed using SPSS software version 27 (Armonk, NY: IBM Corp). A Mann Whitney-U Test was used to compare the mean scores of the KJOC between the retrospective and prospective groups. A logistic regression was performed to aid with establishing a predictive score that would determine if subjects were throwing with or without pain. The predictive variable was the subject’s KJOC score, and a dichotomous outcome variable was created for those throwing with pain and those throwing without pain. A receiver operating characteristic curve (ROC) was created to graphically illustrate the diagnostic capability of the dichotomous outcome variable and aid with determining a threshold. The Youden’s J Statistic (J = sensitivity + specificity -1) was then utilized to aid with diagnostic capability and decide on the exact threshold or “cut-score” for the KJOC. The significance level for all statistical tests was set at 0.05.
Results
A total of 56 participants were recruited with 28 subjects in the retrospective group and 28 participants in the prospective group. The characteristics of the participants studied can be found in Table 1. Most recruited subjects were right-hand dominant and participated in sport as a pitcher and additionally played other positions in the field. The retrospective throwing with pain group have been further classified in Table 1 as shoulder pain, elbow pain, or shoulder and elbow pain with throwing. The mean score on the KJOC in those throwing with pain was 61.9 points (+/- 19.7), while the mean for those throwing without pain was determined to be 88.7 points (+/- 9.2); as seen in Table 2. Figure 1 represents the KJOC scores found throughout each group.

The results of the Mann Whitney U indicated that the groups were significantly different from one another (U = 698.5, p < 0.001). The results of the logistic regression with creation of an ROC curve revealed that the KJOC was able to discriminate between those throwing with pain and those throwing without pain (Area Under Curve (AUC) .891), as represented in Figure 2. Youden’s J statistic was then utilized to establish a predictive threshold score for identifying young baseball athletes who are throwing with and without pain. The results indicate this threshold score to be at 68.6 points, which signifies anyone scoring above this threshold would be throwing with no pain and a score below this number indicating throwing with pain.
In considering that the age range of the subjects encompasses a variety of stages of growth and musculoskeletal development, the authors have also provided a breakdown of the data in Tables 1 and 2 into younger (10-13 years old) vs older ages (14-18 years old). The age demographic was split to display different levels of participation: ages prior to high school and the high school-aged athlete. As can be observed in Table 2, the scores for pain and no pain were very comparable when age was taken into consideration. According to Mann-Whitney-U tests, the distribution of KJOC scores was not significantly different across age categories for both the no pain (p = 0.286) and the pain (p = 0.853) groups, indicating that age subgroup was not a major factor impacting the KJOC threshold determination.
Discussion
Injury assessment can entail various objective and subjective measures. A patient-reported assessment tool can aid with participation screening and guide clinical decision-making in physical therapy. PRO measures provide a quantified score to determine if an athlete is experiencing pain with participation. The intent of this study was to determine if utilization of the KJOC in youth baseball players can differentiate and predict those throwing with and without symptoms. The validation of such a number could further communication if a youth baseball athlete is throwing with pain, and provide guidance with management, as well as being useful in monitoring treatment success or supporting return to sport decisions. This is the first study to utilize the KJOC with male baseball athletes between the ages of 10 through 18 and compare groups between those with and without upper extremity symptoms. Prior literature has validated the KJOC’s use in the professional adult baseball athlete. During the original research, a score of a 81.3 was found to be 95% accurate with separating groups of pain and no pain in adult baseball athletes.5,18 Beyond its original validation, a respondent score of 90 on the KJOC determined asymptomatic throwing in the adult baseball thrower.27 Concerning the younger softball pitcher, research on female athletes in Canada has indicated that those with KJOC scores lower than 90 in the preseason had significantly greater risk of reporting an in-season injury.19 Additionally, Wei et al studied a small sample (n=9) of younger throwing athletes with clinical symptoms of little league elbow utilizing MRI, and recorded their KJOC scores.28 The authors reported that an average score of 60.3 on the KJOC indicated that subjects reported trouble with play or were no longer throwing due to pain.28 Thus, the literature utilizing the KJOC in youth baseball players is scarce and shows considerable variability in what scores are considered predictive or how they can assist decision-making; and does not include comparisons between those throwing with pain and those who are pain-free. The current study specifically looks at this comparison and shows that there is a statistical difference in KJOC scores between those throwing with and without symptoms. The between-groups analysis provides a way to identify a predictive threshold score for symptoms with throwing, with a cutoff score of 68.6 being the most appropriate threshold score to distinguish between these two groups.
The use of the KJOC in the youth baseball athlete population is clinically relevant and provides an important tool to guide decision-making. Choosing the right PRO measure for a patient may pose a challenge to many clinicians. To identify which PRO measures are better suited to the assessment of young baseball throwers, it is important to understand the intent of each PRO measure, interpretability, validation, reliability for testing, responsiveness to change, and response scaling. Other PRO scales that focus on the upper extremity, such as the Disability of Arm, Shoulder and Hand (DASH) and the Pennsylvania Shoulder Score (PSS) have ceiling effects, lack specificity for asking baseball-related questions, or do not differentiate between body regions.6,29 Previous research has challenged the KJOC and its use with the younger thrower regarding interpretability and the use of a VAS due to the younger reader simply choosing extreme end points for each question.7 In response to this, the development of the Youth Throwing Score (YTS) was created, which uses a Flesch-Kincaid reading level for the younger demographic and uses a Likert scale for response.7 However, further research has concluded the use of either a VAS or Likert scale can still provide dichotomous extremes for answers in a young population.30
The application of a PRO measure, such as the KJOC, can provide valuable and clinically relevant information for the healthcare provider concerning many International Classification of Functional, Disability, and Health (ICF) enablement model constructs. Specifically, the KJOC provides information regarding body function and structure, activity and participation, and environmental factors that are associated with participation in baseball. Critics of the KJOC assert that this scale focuses only on impairments and activity limitations and does not address other domains of emotional or social factors.31 However, children may have a difficult time answering questions within the emotional or social domain. Additionally, the KJOC scale does ask how much the athlete’s arm problems have affected their relationships, which does provide an environmental/contextual factor construct of the ICF model.
The use of a PRO measure can also help enhance communication between the provider and the patient so that the clinician further explores subjective information on the patient’s throwing pain patterns. The establishment of a cut-score offers a predictive number that guides the likelihood that throwing is reproducing the athlete’s upper extremity symptoms. This information can help the clinician initiate a more detailed conversation with the subject regarding their pain patterns and activity/participation limitations. It can also further guide clinical decision-making to continue with a current plan of care, such as a throwing progression program, or to modify the program based on the response to this questionnaire.
The results of this study support the use of the KJOC in the young baseball athlete, and its usefulness in predicting the presence of symptoms with throwing via a threshold score. However, there are some limitations to be considered. Further research should address the interpretability of this scale compared to other published PRO measures, such as the YTS. The demographic studied includes a large range from 10 to 18 years of age, which could provide a limitation regarding the wide range of interpretability of questions across levels of education. Finally, lack of random sampling in this study reduces generalizability, however, the samples chosen include real-life representations of youth athlete demographics with and without pain that are readily available, and which provide important information with clinical applicability. A randomized prospective study would be limited by the lack of control over the occurrence of symptoms and other considerations such as natural history. Additional research could employ the KJOC throughout this populations’ participation in sport that could include the beginning, during, and end of their baseball season and retesting at the initial complaint of arm pain with throwing. Finally, in this study there is a wider range of variability in KJOC scores for those throwing with pain (Interquartile Range (IQR) = 35.30) versus those throwing without pain (IQR = 15.48), which results in an overlap of scores and complicates group separation. Future research could address scores on the KJOC at different age ranges or levels of play for the youth baseball athlete, in an attempt to obtain narrower variability and enhance predictive ability for those throwing with symptoms.
Conclusion
The results of this study reflect that the KJOC can differentiate between younger baseball athletes throwing with and without pain. The predictive threshold score of 68.6 points can be used in a clinical setting to aid in determining if a youth or high school-aged athlete is suffering from pain while participating in overhead throwing. Lack of subjective communication given by patients of a younger age can pose a challenge to assess response to treatment. The results of this research can aid with improving communication between a younger demographic reporting pain and assessing subjective levels of function. Additionally, the KJOC can be utilized with the youth baseball athlete population to monitor progression of treatment and aid with documentation.
Conflict of Interest
There are no conflicts of interest to disclose.